
[box type=”bio”] What to Learn from this Article?[/box]
In cases of high-grade open olecranon injuries Ilizarov half ring and olive wire fixation allows stable fixation, immediate initiation of range of motion, optimal wound care and good long term outcome.
Case Report | Volume 5 | Issue 1 | JOCR Jan-March 2015 | Page 19-22 | Pradip Sharad Nemade, Kumar Kaushik Dash, Tanvi Yeshwant Patwardhan, Pravin Vasant Londhe. DOI: 10.13107/jocr.2250-0685.246
Authors: Pradip Sharad Nemade[1], Kumar Kaushik Dash[1], Tanvi Yeshwant Patwardhan[2], Pravin Vasant Londhe[1]
[1] Department of Orthopaedic Surgery, Seth G.S. Medical College & K.E.M. Hospital, Mumbai. India.
[2] Consultant Physiotherapist, Marve Nursing Home & Polyclinic, Marve Road, Malad (W) Mumbai. India.
Address of Correspondence:
Dr. Pradip Sharad Nemade, Department of Orthopaedic Surgery, Seth G.S. Medical College & K.E.M. Hospital, Parel, Mumbai – 400012. India. Email: pradipnemade@hotmail.com
Abstract
Introduction: External fixator application can be difficult for olecranon fractures in presence of large degloving injuries. We describe use of simple Ilizarov ring fixator construct for grade IIIB open olecranon fracture management.
Case Report: A 45-year-old female with Grade III B open comminuted olecranon fracture (30*15cm degloving area) and ulnar nerve palsy was treated with a novel ring fixator construct. Two cut-end olive wires were passed from the proximal olecranon across the fracture site in intramedullary fashion exiting dorsally at mid-ulnar level through healthy skin and were attached to an Ilizarov half ring secured by perpendicular wires. The olive wires were tensioned, achieving compression and stability. Range of motion (ROM) exercises could be started quickly as the elbow was not spanned. Wound healed after skin grafting and at one-year follow-up the patient has good functional results (PRE 7, DASH 9.48), elbow ROM 100-1300, 750 pronation and 850 supination. The patient returned to pre-injury occupational activities and had no pain. At three-year follow-up, the x-ray and CT showed union of olecranon fragment with well-maintained congruency.
Conclusion: Internal fixation in most cases may be precluded by the soft tissue trauma and risk of infection. In addition, the small proximal fragment precludes a stable external fixation. In this technique, the hardware is kept away from the open wound allowing better wound inspection and care. The intramedullary olive wires provide compression and stability, and thus allow early ROM. Ilizarov half-ring and olive wire fixation can be an useful option for management of high grade open olecranon fractures because of its advantages, viz. stable fixation, minimal internal hardware, optimal wound care, immediate initiation of range of motion, and good outcome.
Keywords: Ilizarov, Open Olecranon Fracture, External Fixation, Elbow Trauma.
Introduction
Open olecranon injuries are complicated by risk of infection, inability to use internal fixation devices and wound complications. Most of the times, these injuries can be managed by temporary external fixation, till the wound heals, followed by definitive internal fixation. However these devices are difficult to apply in presence of large degloving injuries. We describe a case of Grade III B Gustilo Anderson Open olecranon fracture managed with Ilizarov external fixation construct; along with its surgical technique.
Case report
A 45-year-old female gardener presented to the emergency department after a direct injury to right elbow in a road-traffic accident. On examination, general condition of the patient was stable. She had a 30cm*15cm area of de-gloving wound on posterior aspect of upper extremity, extending from mid-arm level to mid-forearm, which was severely contaminated with dust and gravel. Comminuted bony pieces were directly visible in the wound, along with extensive stripping of periosteum and some loss of common flexor muscle mass. The ulnar nerve was exposed in the wound and showed few contusions. The wound was cleaned with plenty of plain saline lavage and patient was started on broad-spectrum antibiotics. Neurological examination revealed sensorimotor deficit along the ulnar nerve distribution.
Radiographs revealed a comminuted fracture of olecranon with some bone loss on medial side (Schatzker type D fracture, AO/OTA 21-B1.3) [Fig 1]. 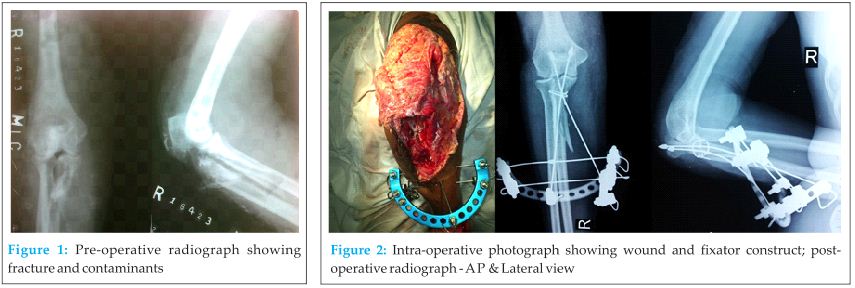 The coronoid process was also fractured and displaced towards volar aspect.
The coronoid process was also fractured and displaced towards volar aspect.
Under general anaesthesia, initially the wound was cleaned meticulously and all visible contaminants were removed. Debridement of nonviable tissues was undertaken and extensive lavage with normal saline was perfomed. The fracture anatomy was reassessed. Bone loss on medial aspect of olecranon was noted. The coronoid process fragment was found to have a long distal beak, which was reduced to the shaft and fixed with encerclage wiring. The proximal fragment was fixed with the reconstructed distal fragment using Ilizarov fixator [Fig 2]. One cut-end olive wire was passed from the proximal olecranon across the fracture site in an intramedullary fashion exiting out at mid-ulnar level through healthy skin dorsally. We faced technical difficulty in controlling the exit of this wire at desired level due to its long intramedullary course. Hence we initially made a track in retrograde fashion using another long K-wire and later on passed the olive wire with slightly bent tip through the same track, in antegrade fashion. An ilizarov half ring was then secured to the ulna using two tensioned wires passed perpendicular to the shaft. The longitudinal olive wire was then attached to the half-ring and tensioned, achieving reduction. Another olive wire was passed in antegrade fashion at an angle to the longitudinal wire to increase the stability of construct.[Fig 2]. This entire construct was away from the fracture and no hardware was present directly in the wound.
The ulnar nerve showed some contusions but was morphologically intact. The soft tissue was approximated as much as possible, covering the nerve and encerclage wire. The skin was tagged using non-absorbable sutures over a drain.
Post-operatively range of motion exercises were encouraged within the tolerance limit of patient. Third day onwards, majority of skin had showed progressive discoloration. However, there were no signs of infection. On seventh day, the dead skin flap was debrided and daily dressing continued. The wound started granulating and split thickness skin grafting was done on third week. The graft was accepted in most part of the wound except a small area 2 cm2 distal to the fracture site, which was left for healing by secondary intention. The second olive wire was then removed and active range was encouraged. Wound healed completely over 6 weeks, at which point patient had 900 of flexion. Ulnar nerve had fully recovered by this time, however patient started developing mild symptoms of CRPS, which was managed by physiotherapy and resolved with time. The fixator was removed at 5 months and physiotherapy was continued.
At one-year follow-up, the CRPS was subsided and the patient had elbow ROM of 100 to 1300, with 750 pronation and 850 supination.[Fig 3]. 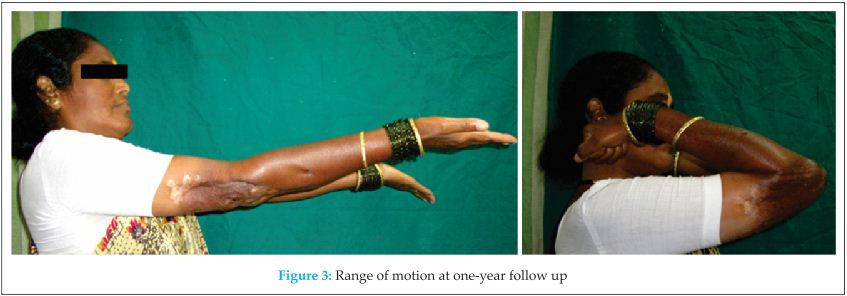 PREE score [1] was 7 (0 is best score, 100 is worst) and DASH score [2] was 9.48 (0 is no disability, 100 is severe disability). The patient returned to pre-injury occupational activities. The dynamic x-ray did not show any inter-fragmentary distraction. [Fig 4].
PREE score [1] was 7 (0 is best score, 100 is worst) and DASH score [2] was 9.48 (0 is no disability, 100 is severe disability). The patient returned to pre-injury occupational activities. The dynamic x-ray did not show any inter-fragmentary distraction. [Fig 4].
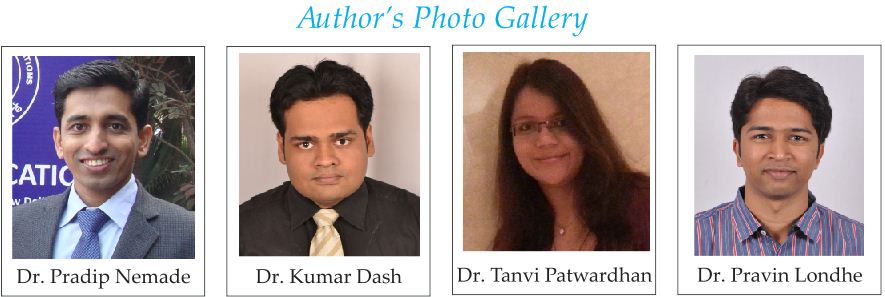
CT scan showed union of coronoid fragment with the shaft. However there was a firm fibrous non-union of olecranon with well-maintained congruency at one-year follow up. [Fig 4]. Considering the condition of soft tissue and bone; along with good functional status, a decision for conservative management for the non-union was made after discussion with the patient. At three-year follow-up, the x-ray and CT Scan showed union with well maintained congruency. [Fig 5] 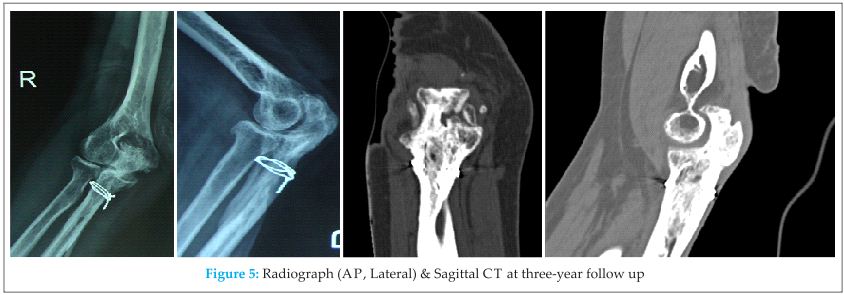 The patient is able to do all her occupational activities (including heavy activities such as lifting water-bucket of 20 Kg. without pain).
The patient is able to do all her occupational activities (including heavy activities such as lifting water-bucket of 20 Kg. without pain).
Discussion
Open olecranon fracture management has dual difficulties. Firstly the internal fixation in most cases may be precluded by the nature of soft tissue trauma and skin condition, with inherent high risk of infection. Secondly, if the high energy trauma leads to a small and comminuted proximal fragment, it becomes biomechanically unfavorable to achieve an external fixation stable enough to allow early range of motion. This problem is further complicated in grade III B open fracture wherein the patient has severe skin loss and exposed fracture site.
Various approaches have been used to deal with this situation. Non-operative management leads to articular incongruity, loss of range and limitation of power of extension. [3] Delaying internal fixation till wound healing causes fibrosis and shortening of triceps. [3] Temporary elbow spanning fixator allows better wound care, however it leads to severe elbow stiffness.
Continuing range of motion while the wound heals is therefore desired in open olecranon injuries. Multiple devices have been described in literature that can be used as a temporary or definitive management to achieve this aim. Tapasvi et al [4] have described a pyramidal configuration external fixator construct for open proximal ulnar fractures. However, small proximal fragments often will not accommodate at least two pins that are required for stability.[4] Moreover, if comminuted (which is often a result of high energy trauma), the proximal fragment will not allow optimal hold for Schanz pins.[4] Kundu et al used a clamp-cum-compressor device in a series of 17 patients with grade I and II open olecranon fractures.[3] Although this device is particularly useful in small wounds; a massive skin loss over olecranon may preclude the use of this clamp as it is applied directly over the olecranon surface through the normal skin. All these devices, being applied near to/ in the wound, will make wound inspection and management difficult in grade III B open injuries.
Aktuglu described use of Ilizarov ring in 3 cases of open acute olecranon fractures (two grade II, one grade IIIA), each managed with a different arrangement of Ilizarov ring constructs. [5] Our technique is based on one of those constructs, where the ring is kept away (distally) from the olecranon which allowed better wound inspection, continuous care and further procedures for skin cover. The intramedullary olive wire holding the proximal fragment provided reduction and compression at fracture site. It also prevented distraction and allowed range of motion throughout the treatment. Thus, the distinct advantage of this system is that all hardware is away from the wound while at the same time achieving adequate stability to allow ROM exercises.
Although initially this construct was planned as a temporary measure till wound healing, due to CRPS we preferred not to perform any surgical procedure of definitive internal fixation for the fear of worsening the symptoms.[6,7] When at the end of one year when CRPS subsided, the patient had firm fibrous non-union of elbow the excellent function. There are multiple surgical procedure described for managing nonunion of olecranon fracture, however no surgical treatment is an acceptable option for painless “fibrous nonunion” with 90 degrees or more of flexion.[8] Asymptomatic nonunion with adequate elbow joint function requires no active treatment.[8] Patient was satisfied with the achieved functional result and decided against the any further surgical procedure for non-union and continued having good functional result till the latest follow-up visit at three-years, at which time union was observed on the x-rays and CT-Scan.
Conclusion
We propose this Ilizarov half-ring and olive wire fixation as a useful tool in the armamentarium of an orthopedic surgeon for high grade open olecranon fractures because of its advantages, viz. stable fixation, minimal internal hardware, optimal wound care, immediate initiation of range of motion, and good outcome.
Clinical Message
When facing a scenario of open olecranon fractures with severe wound contamination and/or soft tissue loss, where internal fixation is not possible, the surgeon has to decide which mode of external fixation to use. In that situation, this Ilizarov half-ring and olive wire fixation is a good option. This allows the surgeon to achieve good stability without compromising on ease of wound care (the ring is away from wound site) or sacrificing elbow motion (the fixation device does not span elbow joint).
References
1. Dowrick AS, Gabbe BJ, Williamson OD, Cameron PA. Outcome instruments for the assessment of the upper extremity following trauma: a review. Injury 2005 Apr;36(4):468-76.
2. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med 1996 Jun;29(6):602-8. Erratum in: Am J Ind Med 1996 Sep;30(3):372.
3. Kundu ZS, Kamboj P, Sangwan SS, Siwach RC, Singh R, Walecha P. Management of open olecranon fractures using clamp-cum-compressor device. Ind J Orthop 2009;43(1):50-4.
4. Tapasvi S, Diggikar MS, Joshi AP. External fixation for open proximal ulnar fractures. Injury 1999;30(2):115-20.
5. Aktuglu K,Ozsoy H. llizarov circular external fixator for open olecranon fractures-a report of 3 cases. Acta Orthop Scand 1999;70(1):93-6.
6. Katz MM, Hungerford DS: Reflex sympathetic dystrophy affecting the knee. J Bone Joint Surg Br 1987;69:797–803.
7. Veldman PH, Goris RJ: Surgery on extremities with reflex sympathetic dystrophy. Unfallchirurg 1995;98:45–8.
8. Papagelopoulos PJ, Coonrad RW, Morrey BF. Nonunion of the Olecranon and Proximal Ulna. In: Morrey BF, editor. The Elbow and Its Disorders. 4th Ed. Philadelphia: Saunders Elsevier; 2009. p. 401-18.
| How to Cite This Article: Nemade PS, Dash KK, Patwardhan TY, Londhe PV. Use of Ilizarov Fixator for Grade III B Open Olecranon Fracture: a Case Report and Surgical Technique. Journal of Orthopaedic Case Reports 2015 Jan-March;5(1): 19-22. Available from: https://www.jocr.co.in/wp/2015/01/28/2250-0685-246-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


