
[box type=”bio”] What to Learn from this Article?[/box]
Freiberg infraction is a relatively rare osteochondrosis of the metatarsal head. Early diagnosis can lead to complete recovery. Athletes with later stages of Freiberg infraction can find relief with conservative management but ultimately may require surgical intervention.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 12-14 | Johnnie Faircloth, Jennifer J Mitchell, David S Edwards. DOI: 10.13107/jocr.2250-0685.295.
Authors: Johnnie Faircloth[1], Jennifer J Mitchell[2], David S Edwards[2].
[1] Pediatrics & Sports Medicine, Texas Tech University Health Sciences Center 1400 Coulter Amarillo, TX 79106.
[2] Family and Community Medicine & Sports Medicine, Texas Tech University Health Sciences Center 3601 4th Street Lubbock, TX 79430.
Address of Correspondence
Dr. Johnnie Faircloth
Assistant Professor, TTUHSC School of Medicine , 1400 Coulter, Amarillo, TX 79106.
E-mail: johnnie.faircloth@ttuhsc.edu
Abstract
Introduction: Freiberg infraction is a relatively rare osteochondrosis of the metatarsal head. The etiology of Freiberg infraction is poorly understood but likely involves factors such as, repetitive trauma and vascular compromise. When discovered early, Freiberg infraction can be cured with conservative measures but late presentations require surgical intervention. We present a case of stage V Freiberg infraction in a Division I collegiate tennis player that responded to conservative treatment.
Case Report: A 20 year old female tennis player presented with worsening of her chronic foot pain. She had tenderness to palpation and diminished range of motion at the second metatarsophalangeal joint. Radiographs revealed late stage Freiberg infraction of the second metatarsal. This patient’s pain was successfully treated with conservative measures; prolonging her collegiate tennis career.
Conclusion: Surgical intervention is required for definitive treatment of late stage Freiberg infraction. Conservative treatment can be effective in prolonging the athlete’s career.
Keywords: Osteochondrosis, Freiberg infraction, Metatarsal, Foot pain.
Introduction
Freiberg infraction is a relatively rare osteochondrosis of the metatarsal head [1-5]. The etiology of Freiberg infraction is poorly understood but likely involves factors such as, repetitive trauma and vascular compromise [1-5]. When discovered early, Freiberg infraction can be cured with conservative measures but late presentations require surgical intervention [1-5]. Smillie staging, based upon the level of bone and joint degradation found on radiograph, can aid in the prognosis and treatment planning [1, 5]. Early stages, I-III can be cured with conservative measures but later in the course of the disease, stages IV and V, surgical intervention is required for definitive cure [1, 4, 5]. We present a case of stage V Freiberg infraction in a Division I collegiate tennis player whose pain was successfully treated with conservative treatment.
Case Report
The patient is a 20 year old female tennis player who presented with a complaint of worsening of her chronic foot pain. She stated that she had a condition with a “funny name” affecting her right foot that began around age thirteen. The condition caused pain in the top of her foot that worsened when she participated in tennis. Forcefully pushing off on the right foot, while making lateral direction changes from right to left, exacerbated her pain. The pain previously occurred only with tennis but for over a year had been present most of the time with variable intensity. The quality of the pain was aching and usually only moderate in intensity. It did not affect her activities of daily living but had affected her practice. She guarded against putting direct pressure on the mid foot by planting more medially or laterally during direction change in practice. She did not let the pain affect her push off during competition and usually had the most severe pain post competitive play. She had recently increased the intensity of her practices from a relative rest over the summer. She denied any mechanical symptoms of the foot. She had used various over the counter non steroidal anti inflammatory medications without much relief. She did get some relief from prescription carbon fiber shoe inserts and padded insole supports (Fig 1), prescribed by a podiatrist, and regularly replaced her tennis shoes. She wanted to know if anything more could be done to relieve her pain. She had a past medical history of forearm fracture at around one year of age. Her family history was non-contributory. Her social history found that she enjoyed competitive tennis, was doing well in school, and denied substance abuse. Review of symptoms was negative. She was a healthy appearing female. There were no lower extremity color changes or edema. Ankles had symmetric active eversion, inversion, dorsiflexion and plantarflexion. Active dorsiflexion and plantarflexion of the toes revealed a limitation in the range of motion of the second toe of the right foot (Fig 2). Passive dorsiflexion of the second toe was blocked at 30 degrees and plantarflexion was painful at 30 degrees. She had dorsal and plantar tenderness to palpation over a bony deformity at the second metatarsophalangeal joint but no other tarsal, metatarsal or phalangeal tenderness. Single leg toe raise was painful on the right. She had normal arches and gait. The lower extremity neurovascular exam was normal.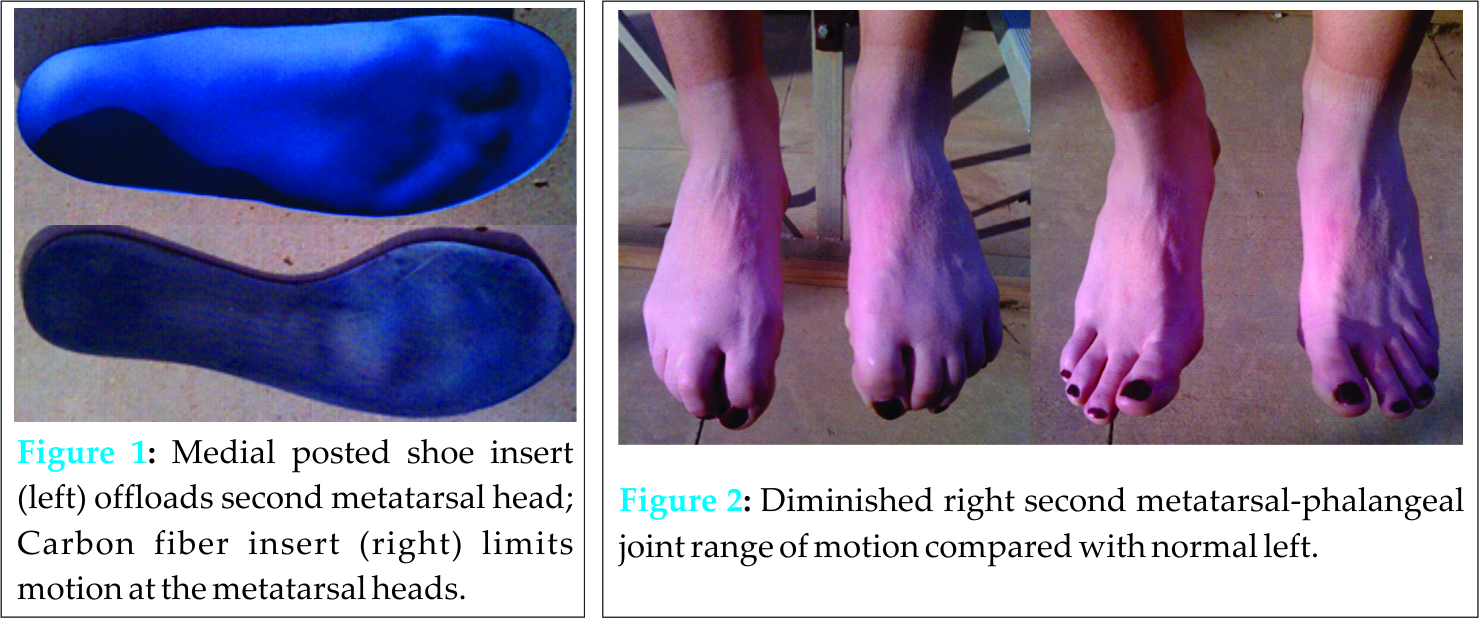
The differential diagnosis included metatarsalgia, Morton neuroma, stress fracture, Freiberg infraction
X-ray of the right foot revealed second metatarsal head bony changes which included flattening of the bone, sclerosis, and fragmentation. The final diagnosis was osteochondrosis of the second metatarsal head – Freiberg infraction (Fig 3). She was unwilling to give up competitive tennis at the time. She was advised to continue her carbon fiber foot plate which limits motion at the metatarsal head and continue her medial posted shoe insert to offload the second metatarsal head. Additionally, the athletic training staff worked with her on additional custom padding for comfort and offloading of the painful foot. We also prescribed scheduled oral indomethacin 75-mg extended-release capsules once daily for three weeks. We discussed the possibility of future steroid injection into the diseased joint. The patient was evaluated at three weeks post initial consultation. She had just returned from a tournament where she won second place and stated that she was back to her baseline level of symptoms.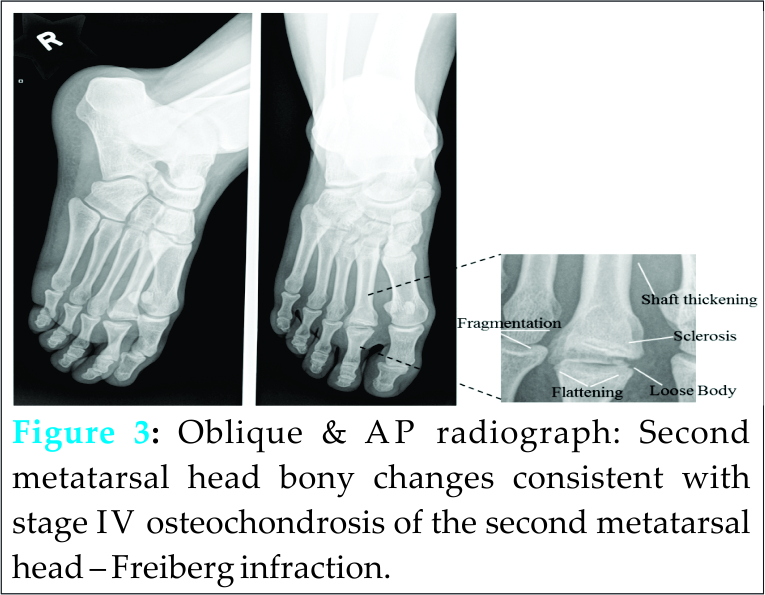
Discussion
Freiberg infraction is a relatively rare osteochondrosis of the metatarsal head [1-5]. It is the fourth most common osteochondrosis and the second most common in the foot [1]. The second metatarsal head is most commonly affected but any can be involved and the condition can occur bilaterally [1, 2, 4]. The condition is five times more common in females when compared to males [1]. Freiberg infraction can occur at any age but the peak onset is in adolescence [1, 3]. The etiology of Freiberg infraction is poorly understood but likely involves factors such as, repetitive trauma and vascular compromise [1-5]. A longer and less mobile second metatarsal may take more stress during gait and athletic activities with the resulting effusion also contributing to compromised blood flow [1]. Chronic illness and prescription steroid use are risk factors [1, 3]. The patient will present with pain, usually near the second metatarsal, that is worsened by activity [1-4]. There may be associated swelling, mechanical symptoms like crepitus and clicking, and lost range of motion [1-4] (Fig 2). Diagnosis of Freiberg infraction is by x-ray and is best seen with a forty five degree oblique view [1-5]. Joint space widening may be the first visible sign [1, 3, 4]. Late in the course radiographic findings include joint depression, loose bodies, fragmentation and sclerosis [1, 3, 4, 5]. Magnetic resonance imaging may be necessary if the patient presents very early in the course or if planning surgical intervention [1].
Smillie staging can be useful in prognosis and in planning treatment [1, 5]. In stage one an ischemic epiphysis develops fissure type fractures [1, 5]. An altered articular contour of the metatarsal head results from central bone resorption in stages two and three [1, 5]. In stage four loose bodies form due to fracturing of the lateral and dorsal projections [1, 5] (Fig 3). Stage five is marked by complete metatarsal head flattening and a deforming arthrosis is present [1, 5]. Early in Freiberg infraction, stages one through three, conservative treatment includes activity modification, insoles, metatarsal pads, casting or controlled ankle motion walking boot and non-steroidal anti-inflammatory medications and patients may spontaneously improve [1-4] (Fig 1). Local steroid injection may also provide some relief. Surgical intervention is reserved for stages four and five and may include debridement, bone grafting, osteotomy, or joint replacement if the disease is advanced or if symptoms are severe [1, 4, 5].
Conclusion
Conservative measures can be successful in treating and curing early stage Freiberg infraction, while later stages require surgical intervention. Although she had late stage Freiberg infraction, our patient’s pain responded well to conservative treatment. It is unknown at this time how long these temporizing measures will last. Eventually, she may require alteration in her activity level and/or surgical correction.
Clinical Message
Freiberg infraction is a relatively rare osteochondrosis of the metatarsal head. Early diagnosis can lead to complete recovery. Athletes with later stages of Freiberg infraction can find relief with conservative management but ultimately may require surgical intervention.
Reference
1. Cerrato, R.A. Current Management of Lesser Toe Disorders: Freiberg’s Disease. Foot Ankle Clin. 2011 Dec; 16(4): 647-58.
2. Atanda, A., Shah, S.A. O’brien, K. Osteochondrosis: Common Causes of Pain in Growing Bones. Am Fam Physician. 2011 Jan; 83(3): 285-91.
3. Love, J.N., O’Mara, S. Freiberg’s Disease in the Emergency Department. J Emerg Med. 2010 Jan; 38(4): e23-e25.
4. Waldman, S.D., Campbell, R.S.D. Freiberg’s Disease. In: Imaging of Pain. 1st ed. Philadelphia, PA: Saunders; 2011. p 447-448
5. Smillie, I.S. Treatment of Freiberg’s Infraction. Proc. R. Soc. Med. 1967 Jan; 60: 29-31.
| How to Cite This Article: Faircloth J, Mitchell JJ, Edwards DS. Late Stage Freiberg Infraction in a Division I Collegiate Tennis Player. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 12-14. Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-295-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


