
[box type=”bio”] What to Learn from this Article?[/box]
It is a simple & very effective technique to remove the stripped headed or jammed locking screws.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 35-37 | Harpreet Singh, Rohit Sharma, Sachin Gupta, Narinderjit Singh, Simarpreet Singh. DOI: 10.13107/jocr.2250-0685.302.
Authors: Harpreet Singh[1], Rohit Sharma[1], Sachin Gupta[1], Narinderjit Singh[1], Simarpreet Singh[1]
[1] Department of Orthopaedics, SGRD Medical College, Amritsar. India.
Address of Correspondence
Dr. Harpreet Singh
B-/274, Staff Road Chander Nagar, Near Puran Singh Depoo, Batala, Dist: Gurdaspur – 143505. India.
E mail – drhp.singh@yahoo.com
Abstract
Introduction: The advent of locking plates has brought new problems in implant removal. Difficulty in removing screws from a locking plate is well-known. These difficulties include cold welding between the screw head and locking screw hole, stripping of the recess of the screw head for the screwdriver, and cross-threading between threads in the screw head and screw hole. However, there are cases in which removal is difficult. We describe a new technique for removing a round headed, jammed locking screws from a locking plate.
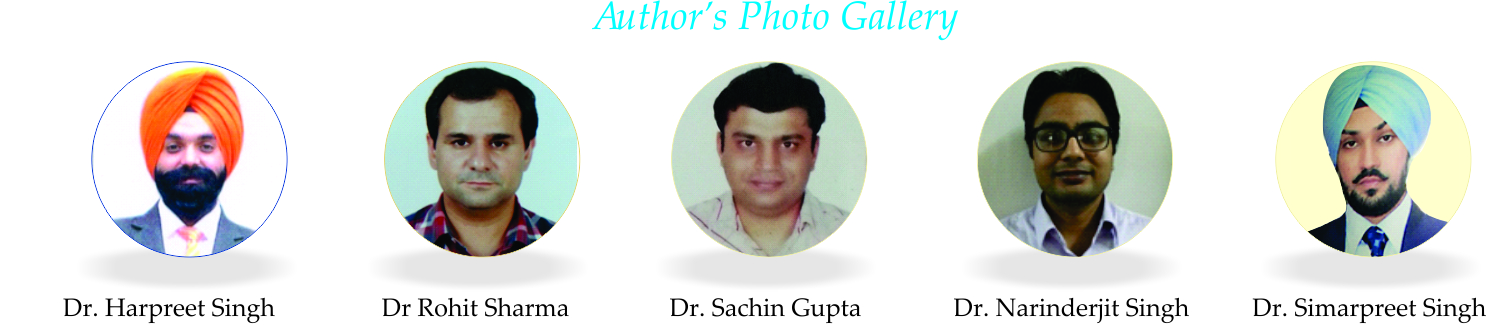
Case Report: 55 years old male patient received a locking distal tibial plate along with distal fibular plate 3years back from UAE. Now patient came with complaint of non-healing ulcer over medial aspect of lower 1/3rd of right leg from past 1 year. Non operative management did not improve the symptoms. The patient consented to implant removal, with the express understanding that implant removal might be impossible because already one failed attempt had been performed at some other hospital six months back. We then decided to proceed with the new technique. The rest of the proximal screws were removed using a technique not previously described. We used stainless steel metal cutting blades that are used to cut door locks or pad locks to cut the remaining stripped headed screws.
Conclusion: This technique is very quick, easy to perform and inexpensive because the metal cutting blades which are used to cut the screws are very cheap. Yet it is very effective technique to remove the stripped headed or jammed locking screws. It is also very less destructive because of very less heat production during the procedure there is no problem of thermal necrosis to the bone or the surrounding soft tissue.
Keywords: Round headed screws; jammed locking screws; interlocking plate.
Introduction
The advent of locking plates has brought new problems in implant removal. Difficulty in removing screws from a locking plate is well-known. These difficulties include cold welding between the screw head and locking screw hole, stripping of the recess of the screw head for the screwdriver, and cross-threading between threads in the screw head and screw hole. Several reports described risks, tips, and techniques to remove these locking plates. These include using a conical extraction screw, cutting the plate, and using high-speed carbide drill bits and burrs to remove the screw heads, and removing the shanks with conical extraction screws. The available screw removal kits make implant removal successful more often than not. However, there are cases in which removal is difficult. We describe a new technique for removing a round headed, jammed locking screws from a locking plate..
Case report
The 55 years old male patient received a locking distal tibial plate along with distal fibular plate 3years back from UAE. Now patient came with complaint of non healing ulcer over medial aspect of lower 1/3rd of right leg from past 1 year. 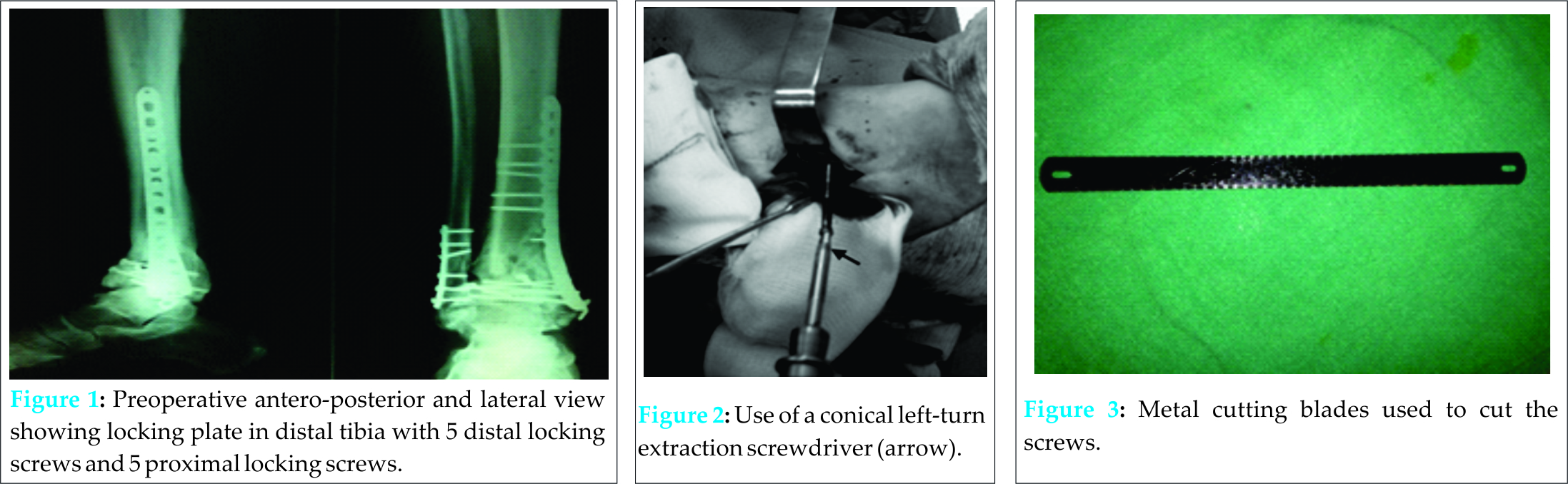 Patient was also type 2 diabetic diagnosed 5 years back. Non operative management did not improve the symptoms. The patient consented to implant removal, with the express understanding that implant removal might be impossible because already one failed attempt had been performed at some other hospital six months back. One of the 5 proximal locking screws was removed using the standard screwdriver. Rest of the proximal screws were stripped headed. For their extraction we used the AO synthes screw extraction kit along with conical extraction screw (AO Synthes) but the screws did not come out. The carbide drill was not available at that time. We then decided to proceed with the new technique. The rest of the proximal screws were removed using a technique not previously described. We used stainless steel metal cutting blades that are used to cut door locks or pad locks to cut the remaining stripped headed screws. Firstly, after exposing the plate to be removed a space is created between locking plate and bone adjacent to screws to be cut with the help of sharp osteotome. Then an iron cutting blade which was previously autoclaved introduced between plate and bone adjacent to screws to be cut and with to and fro motion all the remaining screws were cut. The remaining threaded parts of screws were left in the bone because there removal may further weaken the bone.Overall 2 blades were used to cut the 4 screws. Screws were cut with care with slow to and fro motion of blades but with firm pressure on blade to avoid any unnecessary soft tissue injury. It only takes 10 minutes to cut all the remaining 4 proximal screws and there was no heating problem during the cutting of screws as there is with other procedures such carbide drills and high speed burrs. At the end of the procedure, the surgical wound was washed thoroughly with normal saline to remove metal debris. We name this technique as Rohit’s technique for removal of stripped headed/jammed interlocking screws.
Patient was also type 2 diabetic diagnosed 5 years back. Non operative management did not improve the symptoms. The patient consented to implant removal, with the express understanding that implant removal might be impossible because already one failed attempt had been performed at some other hospital six months back. One of the 5 proximal locking screws was removed using the standard screwdriver. Rest of the proximal screws were stripped headed. For their extraction we used the AO synthes screw extraction kit along with conical extraction screw (AO Synthes) but the screws did not come out. The carbide drill was not available at that time. We then decided to proceed with the new technique. The rest of the proximal screws were removed using a technique not previously described. We used stainless steel metal cutting blades that are used to cut door locks or pad locks to cut the remaining stripped headed screws. Firstly, after exposing the plate to be removed a space is created between locking plate and bone adjacent to screws to be cut with the help of sharp osteotome. Then an iron cutting blade which was previously autoclaved introduced between plate and bone adjacent to screws to be cut and with to and fro motion all the remaining screws were cut. The remaining threaded parts of screws were left in the bone because there removal may further weaken the bone.Overall 2 blades were used to cut the 4 screws. Screws were cut with care with slow to and fro motion of blades but with firm pressure on blade to avoid any unnecessary soft tissue injury. It only takes 10 minutes to cut all the remaining 4 proximal screws and there was no heating problem during the cutting of screws as there is with other procedures such carbide drills and high speed burrs. At the end of the procedure, the surgical wound was washed thoroughly with normal saline to remove metal debris. We name this technique as Rohit’s technique for removal of stripped headed/jammed interlocking screws.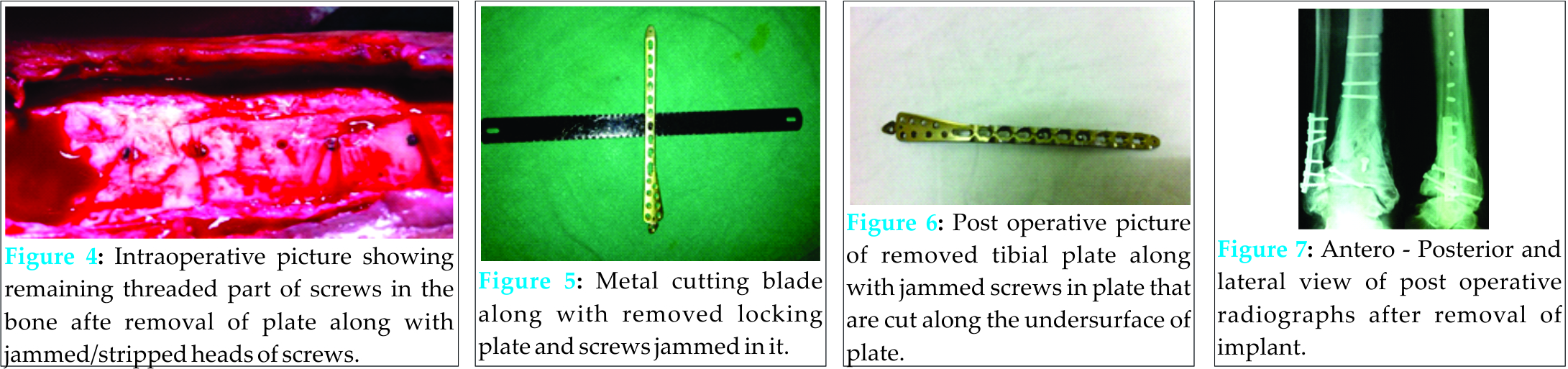
Discussion
Implant removal is considered for pain related to implants, part of treatment, and patient-requested implant removal. Removing implants is often more difficult than the index operation to insert the implant. Risks of implant removal include wound-healing problems [8], neurovascular injury [8], failure to remove all of the implant [9], and refracture [10]. Difficulties in removing a titanium locking screw include jammed screws, damage to the recess in the screw head (stripping) for the screwdriver, and broken screws. Tips, techniques, and pitfalls of implant removal are well described [5]. Instruments including conical extraction screws, hollow reamers, extraction bolts, modular devices, and carbide drill bits have been described in the methods used for removing locking screws [2, 6]. It also is accepted that no one technique can solve all problems in implant removal. The more options available the better. We believe failure to remove the distal screws directly with the conical extraction screw was attributable to the following factors: [1] jamming of the screw head in the locking screw hole, owing to cross-threading and not necessarily cold welding; [2] grip of the screw threads in the far cortex; [3] bony growth over the titanium screw at the far cortex; and [4] as the conical extraction screw was inserted, the screw head jammed farther in the screw hole by expanding the screw head. There is always the danger of thermal bone necrosis or iatrogenic bony injury when using high speed burrs and discs. But our technique is less destructive as produces very less heat as compared to any others because it is not mechanical but a manual procedure. It is essential to have all the appropriate implant removal instruments, including carbide drill bits and high-speed burrs and discs, and prepare for a long procedure [11]. A conical extraction screw is not always successful in removing the jammed screw [2]. The risks of high-speed burrs and discs are high local temperature and metal debris. This technique requires running normal saline solution and continuous suction to remove all the metal debris.
Conclusion
This technique is very quick, easy to perform and inexpensive because the metal cutting blades which are used to cut the screws are very cheap. Yet it is very effective technique to remove the stripped headed or jammed locking screws. It is also very less destructive because of very less heat production during the procedure there is no problem of thermal necrosis to the bone or the surrounding soft tissue.
Clinical Message
Inexpensive & effective method for removal of such implants which are extremely difficult as a result of round headed, cold welding and jammed locking screws heads.
Reference
1. Kumar G, Dunlop C. A technique to remove a jammed locking screw from a locking plate. Clin Orthop Relat Res. 2011 February; 469(2): 613–616. doi: 10.1007/s11999-010-1508-0.
2. Ehlinger M, Adam P, Simon P, Bonnomet F. Technical difficulties in hardware removal in titanium compression plates with locking screws. Orthop Traumatol Surg Res.2009;95:373–376. doi: 10.1016/j.otsr.2009.03.020.
3. Suzuki T, Smith WR, Stahel PF, Morgan SJ, Baron AJ, Hak DJ. Technical problems and complications in the removal of the less invasive stabilization system. J Orthop Trauma. 2010;24:369–373. doi: 10.1097/BOT.0b013e3181c29bf5.
4. Cole PA, Zlowodzki M, Kregor PJ. Treatment of proximal tibia fractures using the less invasive stabilization system: surgical experience and early clinical results in 77 fractures. J Orthop Trauma. 2004;18:528–535. doi: 10.1097/00005131-200409000-00008.
5. Georgiadis GM, Gove NK, Smith AD, Rodway IP. Removal of the less invasive stabilization system. J Orthop Trauma. 2004;18:562–564. doi: 10.1097/00005131-200409000-00014.
6. Hamilton P, Doig S, Williamson O. Technical difficulty of metal removal after LISS plating. Injury. 2004;35:626–628. doi: 10.1016/S0020-1383(03)00097-4.
7. Bae JH, Oh JK, Oh CW, Hur CR. Technical difficulties of removal of locking screw after locking compression plating. Arch Orthop Trauma Surg. 2009;129:91–95. doi: 10.1007/s00402-008-0769-5.
8. Sanderson PL, Ryan W, Turner PG. Complications of metalwork removal. Injury.1992;23:29–30. doi: 10.1016/0020-1383(92)90121-8.
9. Jago ER, Hindley CJ. The removal of metalwork in children. Injury. 1998;29:439–441. doi: 10.1016/S0020-1383(98)00080-1.
10. Takakuwa M, Funakoshi M, Ishizaki K, Aono T, Hamaguchi H. Fracture on removal of the ACE tibial nail. J Bone Joint Surg Br. 1997;79:444–445. doi: 10.1302/0301-620X.79B3.6980
11. Hak DJ, McElvany M. Removal of broken hardware. J Am Acad Orthop Surg.2008;16:113–120.
12. Bhutta MA, Dunkow PD, Lovell ME. A simple technique for removal of screws with damaged heads.Ann R Coll Surg Engl. 2003;85:207.
13. Busam ML, Esther RJ, Obremskey WT: Hardware removal: indications and expectations. J Am Acad Orthop Surg 2006, 14:113-120
14. Hanson B, van der Werken C, Stengel D: Surgeons’ beliefs and perceptions about removal of orthopaedic implants. BMC Musculoskelet Disord 2008, 9:73
Minkowitz RB, Bhadsavle S, Walsh M, Egol KA: Removal of painful orthopaedic implants after fracture union.
| How to Cite This Article: Singh H, Sharma R, Gupta S, Singh N, Singh S. Easy and Inexpensive Technique for Removal of Round Headed, Jammed Locking Screws in Distal Tibial Interlocking Plate. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 35-37. Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-302-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


