
[box type=”bio”] What to Learn from this Article?[/box]
In benign bone tumors, conventional radiography forms the main stay in diagnosis. If not used judiciously, higher imaging like MRI or PET may erroneously lead to diagnosis of malignant neoplasm, thereby by leading to wrong and aggressive management.
Case Report | Volume 6 | Issue 1 | JOCR Jan-Mar 2016 | Page 79-81 | Gulia Ashish, Juvekar Shashikant, Puri Ajay, Desai Subhash DOI: 10.13107/jocr.2250-0685.385
Authors: Gulia Ashish[1], Juvekar Shashikant[2], Puri Ajay[1], Desai Subhash[2]
[1]Department of Orthopedic Oncology, Tata Memorial Hospital, Mumbai, Maharashtra. India.
[2]Department of Radiodiagnosis, Tata Memorial Hospital, Mumbai, Maharashtra. India.
Address of Correspondence
Prof. Subhash Desai,
Department Of Radiodiagnosis, Tata Memorial Hospital, Dr E. Borges Marg, Parel, Mumbai, Maharashtra. India 400012. Email : xraydesai@gmail.com
Abstract
Introduction: Melorheostosis is a benign bone dysplasia affecting predominantly the appendicular skeleton and adjoining soft tissues. The diagnosis can be established on plain radiographs alone and advanced imaging modalities can be avoided. We hereby report a rare case of melorheostosis affecting the foot with a review of the role of various imaging modalities in diagnosis of this rare bone dysplasia.
Case Report: We present the case of a 29 years old man who was diagnosed with melorheostosis affecting his left foot. The patient presented to the outpatient department of our tertiary care referral hospital with complains of pain in the left ankle and foot with imaging and evaluation done at a primary center.The radiograph revealed an irregular, longitudinal extraosseous hyperostosis along the body of the calcaneum and the metacarpals which was consistent with the classical radiological description of melorheostosis. The CT, MRI and bone scan findings corroborated our primary diagnosis.
Conclusion: The purpose of this case report is to review the features of this rare disorder affecting the foot, on multiple imaging modalities and emphasizing the role of conventional radiology in its diagnosis.
Keywords: Melorheostosis, Osteosclerosis, Bone dysplasia, Osteochondrodysplasias.
Introduction
Melorheostosis is a benign bone dysplasia affecting predominantly the appendicular skeleton and adjoining soft tissues. Melorheostosis is derived from Greek: melos = limb, rhein = to flow, ostos =bone. It is diagnosed as incidental radiographic finding in a patient who usually presents as chronic limb pain, swelling and rarely limitation of joint movement. It occurs sporadically and shows typical segmental distribution which has led to the understanding that it is a non-hereditary condition which most probably represents mixed sclerosing dysplasia with disturbance of endochondral and intramembranous ossification [1]. It commonly affects the lower extremity more than the upper [2]. It has been characteristically described as a “flowing hyperostosis” resembling dripping candle wax as an incidental radiograph finding” [2]. The diagnosis can be established on plain radiographs alone and advanced imaging modalities can be avoided. Histology shows nonspecific findings and can lead to erroneous diagnosis [3]. Treatment is mainly symptomatic and conservative.We hereby report a rare case of melorrheostosis affecting the foot with a review of the role of various imaging modalities in the diagnosis of this rare bone dysplasia.
Case Report
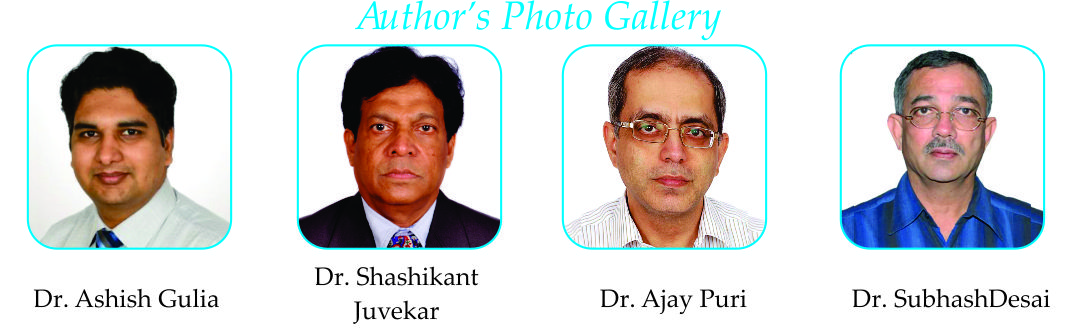
A 29 yrs old male presented to the outpatient department of our hospital with complains of pain in the left ankle and foot for the past 6 months. On local examination, there was tenderness on the dorsal and medial aspect of the left foot. The routine blood investigations were within normal limits. A radiograph of the foot was ordered which revealed irregular, longitudinal extraosseous hyperostosis appearing along the body of the calcaneum and predominantly the 3rd and 4th metatarsals which was consistent with the classical radiological description of melorheostosis- “periosteal hyperostosis along the cortex of long bones, resembling the dripping or flowing of candle wax” (Fig. 1.Classical appearances of melorheostosis affecting the left foot: Anteroposterior and lateral radiograph demonstrates dense cortical and extra-cortical bone formation along the lateral aspect of the calcaneum and the 3rd and 4th metatarsal.-“the dripping candle wax appearance”). The patient had been referred to our tertiary care centre from a primary health centre where he was already investigated with bone scan, computed tomography and MRI. 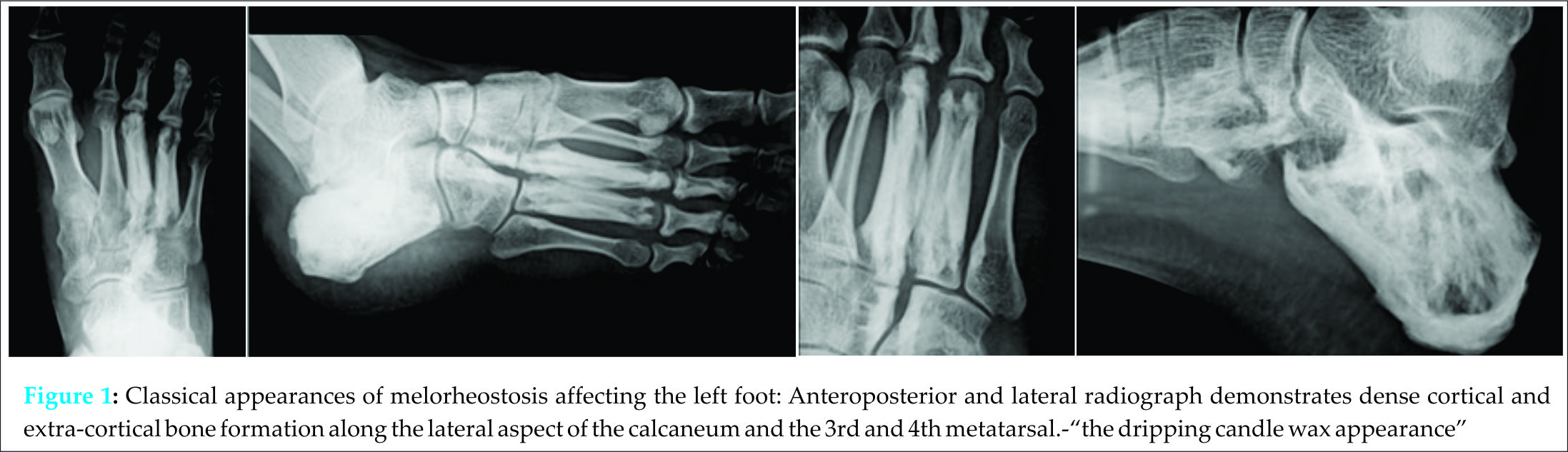 Computed tomography revealed cortical hyperostosis of the calcaneum and metatarsals with hyperdense exuberant sclerotic lesions along the medial aspect of the calcaneum (Fig. 2. Computed tomography shows cortical hyperostosis of the calcaneum and metatarsals with hyperdense exuberant sclerotic lesions along the medial aspect of the calcaneum encroaching into the medullary space characteristic of melorheostosis). On magnetic resonance imaging, these lesions appeared hypointense with thickened cortices on all imaging sequences confirming the sclerotic and hyperostotic nature of the tissue (Fig. 3: Axial coronal and sagittal images showing thickened cortices which were hypointense all imaging sequences confirming the sclerotic and hyperostotic nature of the tissue, associated narrowing of the marrow canal was noted. No other marrow or joint abnormality was seen). The patient was treated with a course of analgesics and he responded well with decrease in the intensity of the pain.
Computed tomography revealed cortical hyperostosis of the calcaneum and metatarsals with hyperdense exuberant sclerotic lesions along the medial aspect of the calcaneum (Fig. 2. Computed tomography shows cortical hyperostosis of the calcaneum and metatarsals with hyperdense exuberant sclerotic lesions along the medial aspect of the calcaneum encroaching into the medullary space characteristic of melorheostosis). On magnetic resonance imaging, these lesions appeared hypointense with thickened cortices on all imaging sequences confirming the sclerotic and hyperostotic nature of the tissue (Fig. 3: Axial coronal and sagittal images showing thickened cortices which were hypointense all imaging sequences confirming the sclerotic and hyperostotic nature of the tissue, associated narrowing of the marrow canal was noted. No other marrow or joint abnormality was seen). The patient was treated with a course of analgesics and he responded well with decrease in the intensity of the pain.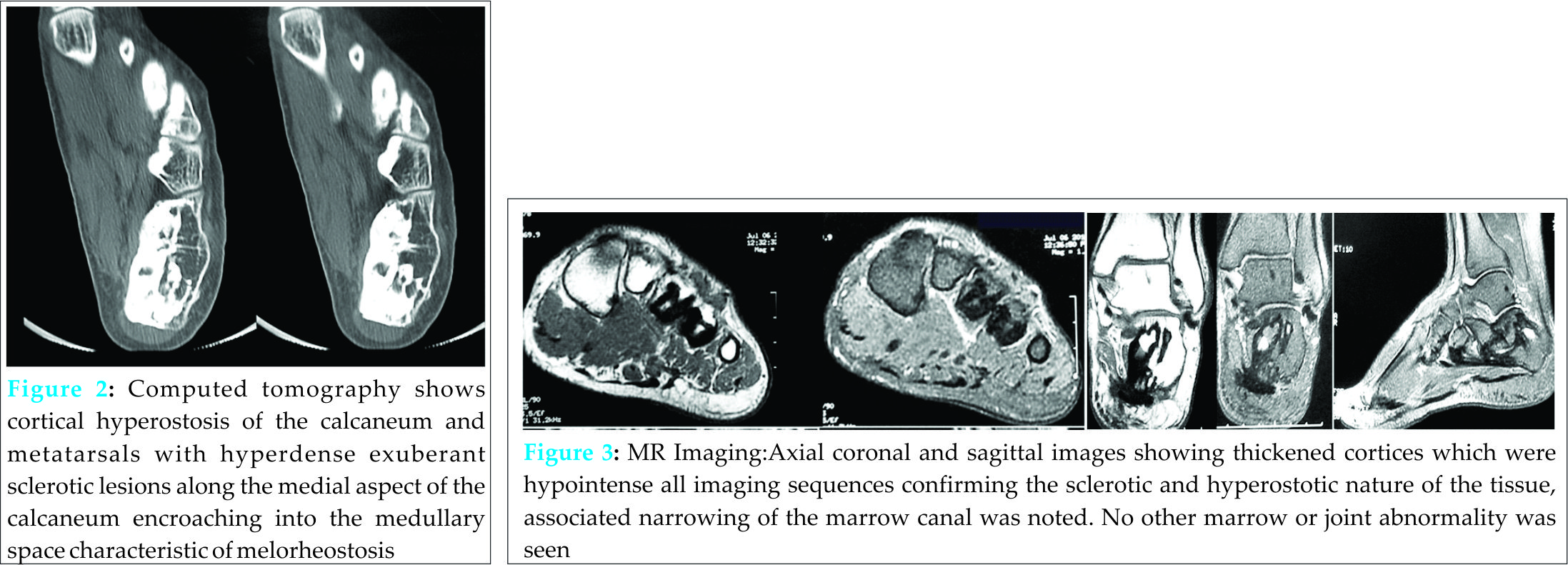
Discussion
Melorrheostosisis a rare benign, sclerosing mesodermal dysplasia that affects the skeleton and adjacent soft tissues, with an incidence of 0.9 cases per million affecting both sexes equally [4]. It was first described by Leri and Joanny in 1922 who described it as “’hyperostose en coulée’ i.e. flowing hyperostosis resembling candle wax [5]. Although a benign condition, the osseous changes can cause significant morbidity [6]. Various theories have been put forward to explain the aetiology of the disorder. The most accepted theory is the classic theory of Murray and McCredie which linked melorheostosis with thescleretomes and proposed that it might be the result of a segmental sensory lesion due to specific infection, insult, or injury to a segment or segments of the neural crest during embryogenesis [7]. Recently, Hellemens et al have demonstrated that a loss-of-function mutation in LEMD3 (on chromosome 12q) is associated with osteopoikilosis, BOS, and melorheostosis [8]. It predominantly affects the appendicular skeleton particularly the long bones of the upper and lower extremities, the lower limb being affected more commonly [2, 9]. There is a predilection for the diaphyseal and the epiphyseal regions of the long bones [10]. A review of literature revealed that very few cases affecting the foot have been reported so far.
The classical radiographic appearance is that of flowing cortical hyperostosis along one side of the shaft of the long bone resembling ”melting wax flowing down the side of a candle” as described by Moore et al [11]. However, this classical textbook description is not seen in all cases. In one of the largest case series so far by Freyschmidt et al, describing 23 patients with the disorder, the various radiological presentations included: osteoma-type (7cases), myositis ossificans–type (1 case), osteopathiastriata–type (6 cases), classic (5 cases), and mixed type (4 cases) [2]. The common differential diagnoses of the radiographic appearance include chronic osteomyelitis, myositis ossificans, osteopetrosis, osteopoikilosis, osteopathiastriata and infantile cortical hyperostosis [3]. Bone scintigraphy demonstrates intense asymmetric cortical radionuclide uptake that may cross articulations to involve adjacent bones [11]. Owing to their hyperostotic nature, these lesions appear hyperdense on CT and hypointense on all MRI sequences. It can rarely be associated with soft tissue masses [12]. A study by Judkiewicz et al. described the appearance of these associated soft tissue masses as heterogeneous signal intensity on all MRI images due to a mixture of mineralized , non-mineralized fibrovascular tissue with variable collagen content and fat. Interestingly, these masses showed mild to moderate post contrast enhancement simulating aggressive neoplastic lesions. In one of the cases, the soft tissue findings were more conspicuous than the osseous changes of melorheostosis leading to an erroneous diagnosis of sarcoma [12].
Conclusion
Melorheostosis is a rare disorder and only a few cases affecting the foot have been described. Although it is a benign dysplasia, it can cause significant morbidity. As clinical radiologists, awareness of the various clinical and radiological presentations can significantly contribute to the appropriate management of these patients. Our case report describes one such uncommon case affecting the foot and highlighting the imaging features of this benign dysplasia on various imaging modalities. Although advanced imaging with CT and MRI complements the finding of convention radiography, if used as a primary imaging modality MRI can lead to overdiagnosis of this benign condition as an aggressive neoplastic lesion; reiterating the importance of conventional radiography in the diagnosis.
Clinical Message
In bone neoplasms, imaging by CT, MRI and PET scans are used primarily to determine its extent and spread; not for diagnosis, except as complementary to conventional radiography in few perplexing cases. If used for diagnosis without conventional plain radiography, erroneous diagnosis of malignant neoplasm would be made for benign bone lesions like melorheostosis, thereby leading to wrong and aggressive management. Thus, conventional radiography forms the main stay in diagnosis of bone neoplasms and awareness of the diverse manifestation of bone neoplasms will significantly contribute to appropriate management.
References
1. Greenspan A. Sclerosing bone dysplasias a target-site approach. Skeletal Radiol 1991;20:561–83.
2. Freyschmidt J. Melorheostosis: A review of 23 cases. EurRadiol 2001;11:474- 479.
3. Jain VK, Arya RK, Bharadwaj M, Kumar S. Melorheostosis: clinicopathological features, diagnosis, and management. Orthopedics 2009;32(7):512.
4. Taybi H, Lachman RS. Radiology of syndromes, metabolic disorders, and skeletal dysplasias. (4th ed.). Chicago 1996;Year Book: 843–4.
5. Leri A, Joanny J. Une affection non decrite des os. Hyperostose’encoulee’ surtoute la longeur d’un member ou ‘melorheostose’. Bull MemSoc Med Hop Paris 1922; 46:1141.
6. Suresh S, Muthukumar T, Saifuddin A. Classical and unusual imaging appearances of melorheostosis. ClinRadiol. 2010;65(8):593–600.
7. Murray RO, McCredie J. Melorheostosis and the sclerotomes: a radiological correlation. Skeletal Radiol 1979;4:57–71.
8. Hellemans J, Preobrazhenska O, Willaert A, et al. Loss-of-function mutations in LEMD3 result in osteopoikilosis, Buschke-Ollendorff syndrome and melorheostosis. Nat Genet 2004;36:1213–18.
9. Bansal A. The dripping candle wax sign. Radiology. 2008;246 (2): 638-40.
10. Khurana JS, Ehara S, Rosenberg AE, et al. Melorheostosis of ilium, femur, and adjacent soft tissues. Skeletal Radiol 1988;17:53.
11. Moore JJ, de Lorimier AA. Melorheostosisleri -review of literature and report of a case. AJR Am J Roentgenol 1933;29:161–71.
12. Judkiewicz AM, Murphey MD, Resnik CS, et al. Advanced imaging of melorheostosis with emphasis on MRI. Skeletal Radiol 2001;30:447–53.
| How to Cite This Article: Ashish G, Shashikant J, Ajay P, Subhash D. Melorheostosis of the Foot: A Case Report of A rare entity with a Review of Multimodality Imaging Emphasizing the Importance of Conventional Radiography in Diagnosis. Journal of Orthopaedic Case Reports 2016 Jan-Mar;6(1): 79-81. Available from: https://www.jocr.co.in/wp/2016/01/02/2250-0685-385-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


