
[box type=”bio”] What to Learn from this Article?[/box]
Early Management and rehabilitation of mutilated hand injuries due to sugar cane machine.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 50-52 | Avijit Mahajan, Ravinder Kumar Khajuria. DOI: 10.13107/jocr.2250-0685.502
Authors: Avijit Mahajan[1], Ravinder Kumar Khajuria[2]
[1]Department of Orthopaedics, Maulana Azad Medical College, New Delhi, India.
[2]Department of Orthopaedics, Sri Guru Ram Rai Institute of Medical and Health Science, Dehradun, Uttarakhand, India – 248001.
Address of Correspondence
Dr. Avijit Mahajan, Senior Resident, Department of Orthopaedics, Maulana Azad Medical College, New Delhi, India.
E-mail: avijit_rahul@yahoo.co.in
Abstract
Introduction: Volumes have been written and practiced in relation to the crush injuries involving hands, over the decades. Mutilated hand and its treatment demands a thorough knowledge of rehabilitative techniques, and an in depth knowledge about the anatomy of hand, in order to achieve successful outcomes in its treatment.
Case Presentation: We present three cases of mutilated hand due to being crushed in a sugarcane machine. All three patients were males, with the age of 14yrs, 30yrs and 34yrs respectively.
Conclusion: Mutilated hand injuries must be treated aggressively and efficiently which is essential to achieve good functional results. Any delay in effective management may lead to stiffness and very poor functional results.
Key Words: Mutilated Hand, Sugar Cane Machine, Workers.
Introduction
Reid defined mutilated hand as the one that “has suffered a severe injury involving loss of substance and has been left lacking in prehension” [1]. These complex injuries with composite soft tissue loss and functional compromise require re-establishment of bony and soft tissue continuity, not only because of the significant loss of soft tissue cover which causes exposure of the deeper structures of hand, but also due to the fact that without such interventions a mutilated hand would remain functionless. The sugarcane machines commonly used in our country have two rollers with irregular surfaces, opposed to each other that are turned either by a handle or an electric motor [ Fig. 1: Motorized sugarcane machine].The sugarcane is kept in-between the two rollers and is churned amongst the rollers. These mutilating hand injuries due to sugarcane machines often occur, when the person is cleaning the machine and this machine is suddenly turned on unknowingly, thus churning the hand in-between its mechanical rollers. The same injury can also occur, if the cloth being used for cleaning the machine gets entrapped amongst the rollers when machine is turned on, therefore, subsequently dragging the hand along with it. The hand gets caught by a force and pulled at a low velocity in-between the rollers of the machine [2]. The irregular surfaces of the roller help the machine onto a firm grip on the hand, in turn pulling the finger tips between the rollers followed by the hand, thus, creating multiple burst lacerations over the fingers. The high energy force leads to fractures, opening of joint capsule, and severe soft tissue injuries.
Case Presentation
We report three cases with crush injury of hand while using sugarcane machine, which presented to us within a period of six months, i.e. March 2015 to August 2015.
Case 1: 14-year-old child, who presented to us within two hours of injury involving his left hand, which he sustained while cleaning the sugarcane machine.
[Fig. 2: a) Pre-operative image of the injured hand b) Post-operative image of the injured hand after skin grafting]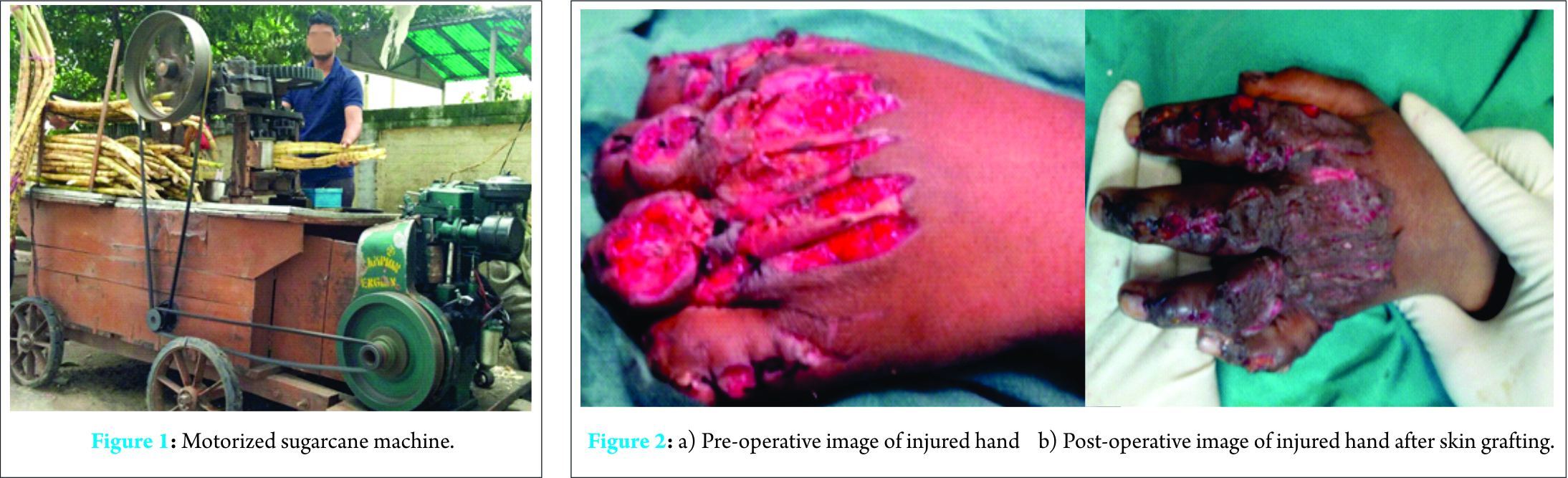
Case 2: 30-year-old man, who presented to us within 1 hour of injury involving his left hand, which he sustained while grinding the sugarcane pulp in the machine.
[Fig. 3: a) Pre-operative image of the injured hand b) Pre-Op X-rays of injured hand c)Post-operative image of the injured hand d) Image After Skin Grafting d) Image At 6 weeks follow-up f) Image at 6 months follow-up]
Case 3: 34 years old man, who presented within 3 hours of injury to the right hand, sustained while grinding the sugarcane pulp.
[Fig. 2: a) Pre-operative image of Injured hand b) Post-operative image of the injured hand c) Image at 4 weeks follow-up]
The two of the three patients sustained injuries to the non-dominant hand. The injury characteristically involved four fingers of the hand. . The thumb being shorter than all the fingers is rarely involved in the cascade of the injury.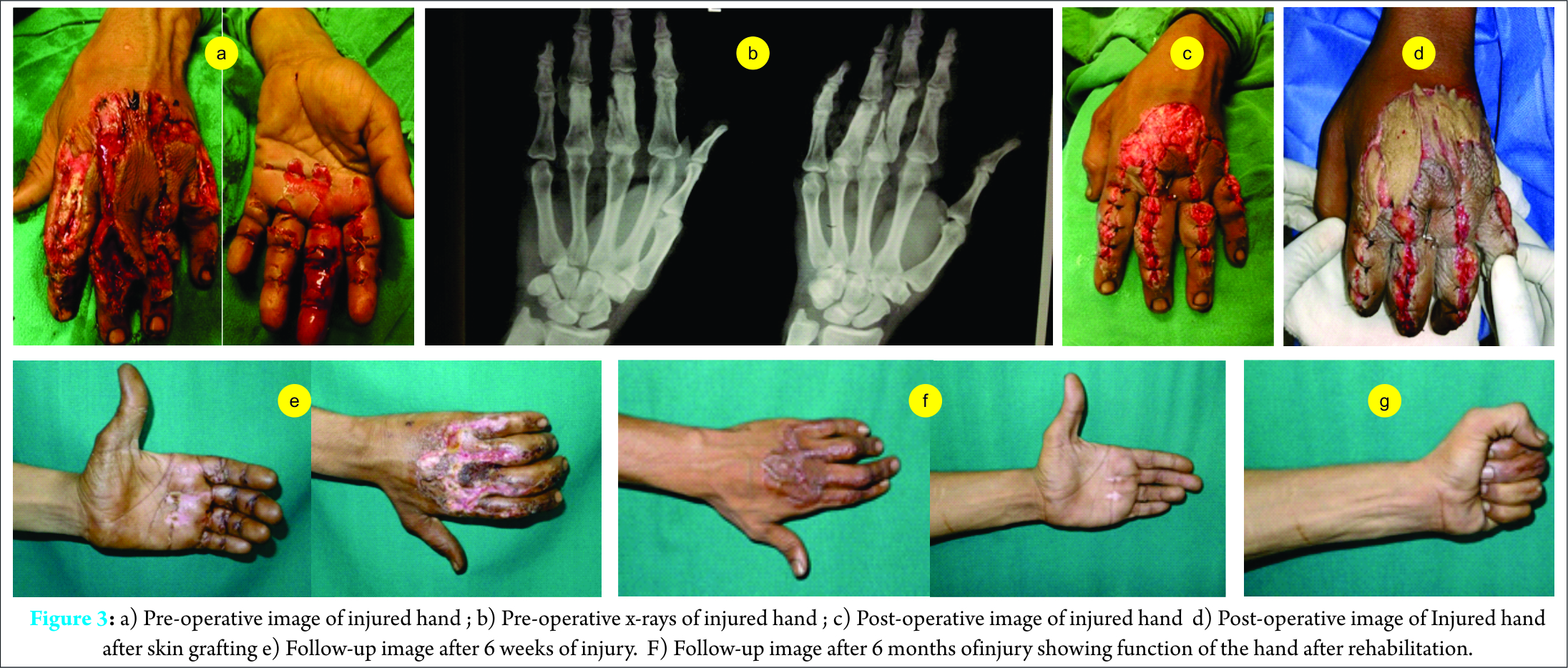
All injured fingers had macerations along the margins of the skin, possibly due to the roller blades being wet at the time of injury. There were longitudinal lacerations over the fingers, both on the dorsal and volar sides, with the nail complex involved sparingly. The lacerations, however, were more extensive on the dorsal side. The extensor expansion had vertical slits running along its length till the metacarpo-phalangeal joints. The proximal interphalangeal joints were exposed with the avulsion of the central slips and loss of continuity of the covering capsules, whereas, the flexor tendons were in continuity with loss of the flexor tendon sheath in the region of the volar skin laceration. The digital nerves and vessels were not damaged, in any of the cases. The bone continuity was lost only amongst two of the three patients.
These injuries were managed with debridement under anesthesia. On receiving the patients, wounds were washed and covered with sterile dressings, with broad spectrum antibiotics being started. Within the operation room, the principles of wound care were followed with an attempt at restoring the bony stability and soft tissue coverage to allow early mobilization of the fingers. Wound debridement and lavage with 6 liters of normal saline was carried out under regional block. The vertical midline slits in the extensor expansion were stitched using interrupted 4-0 nylon sutures. The skin was approximated over tendons to provide them with a biological coverage using sutures i.e. nylon 3-0. The fractures, sustained by case II were fixed using K-wires, whereas, mini fixators were used in case III. Two of these patients required split thickness skin grafting over the dorsum of hand, which was undertaken after the three days of sustaining the injury. The hand was immobilized in using a dorsal plaster slab for pain relief, and the patients were allowed to flex their fingers within the slab. Limb elevation was maintained post-operatively to decrease soft tissue edema. The patients were administered analgesics to reduce the pain and promote active flexion of fingers. The slab was removed in the second week and the K- wires in case 2 were removed after confirming union at three weeks. The patient is assessed for the post-traumatic stiffness, which is clinically apparent in inter-phalyngeal, meta-phalyngeal and wrist joints. The patient undergoes rehabilitation under the supervision of a physiotherapist, where he practices passive, active-assisted and active stretching of the involved joint. The aim is to restore the function to normal or near normal dexterity. The patients were assessed using mini dash score at the end of 6 months. The score was 0 in two patients and 1 patient (case 3) was lost to follow-up.
Discussion
The mutilating injuries of hand have a seasonal incidence; being more common during the spring and summer months, during which the harvest of sugarcane is reaped throughout India. The crushing of hand leads to an “explosive damage“ [3]. Nail complex is usually injured and the fingers (usually the index to little finger) have multiple lacerations of the dorsal and palmar aspect. These lacerations are typically oriented along the long axis of the finger. The extensor expansion has a typical pattern of injury. The expansion is longitudinally split along its entire length, up to the meta-carpophalangeal joint. The central slip is usually avulsed from the base of middle phalynx, exposing the PIPJ to the exterior leaving its capsule torn. The flexor tendons are found in continuity with extensive damage to the flexor tendon sheath in the region of the volar laceration. The digital nerves and vessels usually escape injury, likely due to the longitudinal nature of lacerations [4]. The sugarcane injury is different from press injuries. The rollers of the sugarcane machine have gaps between them, thus leaving some space unlike the press injuries where the entire finger is crushed, including the bones. In the patients managed by us, the bony injuries were less severe compared to the soft tissue injuries which may be due to the explanation offered above. Early Debridement and removal of sugarcane fibers along with intravenous antibiotics should be undertaken and if the tissue are mutilated beyond salvage, amputation with reconstruction of the hand should be undertaken [5].
Conclusion
These injuries are likely to develop significant stiffness and loss of function due to the following reasons a) injury to both the flexor tendon sheath and extensor tendons leading to stiffness on both sides of the fingers b) extensive lacerations with thin skin bridge and loss of skin over some areas c) high risk of infection due contamination by vegetable material d) chance of developing Boutennier’s deformity due to injury to the central slip e) fractures, even when less severe, may cause delay in mobilization.
Clinical Message
The sugar cane machine injury, even though timely intervened, seemingly leaves a partially deformed hand, but the function of the hand returns to near normal after physiotherapy and intervention, primarily by an orthopaedic surgeon.
References
1. Cho BC, Lee JH, Byun JS, Baik BS : Clinical applications of delayed arterialized venous flaps. Ann Plast Surg. 39:145, 1997.
2. GKrishnamoorthy R, Karthikeyan : Degloving injuries of hand. Indian J Plast Surg. 227-236, May-Aug 44(2), 2011.
3. Nemethi CE :Crushing Injury Of Hand-Prevention Of Ischaemic Contractures. Calif Med.207-212,90(3),Mar,1959.
4. Nemethi CE :Crushing Injury Of Hand-Prevention Of Ischaemic Contractures. Calif Med.207-212,90(3),Mar,1959.
5. Ahmad SR : Sugarcane extraction machine injuries of hand. BMC Proceedings, A104,9(Suppl 3),2015
| How to Cite This Article: Avijit Mahajan, Ravinder Kumar Khajuria. Mutilated Hand due to Sugarcane Machine – Challenge to an Orthopaedician (Case series of three patients). Journal of Orthopaedic Case Reports 2016 July-Aug;6(3):50-52. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-502-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


