
[box type=”bio”] What to Learn from this Article?[/box]
Learn a revolutionary proactive surgical treatment for avascular necrosis in sickle-cell patients.
Case Report | Volume 6 | Issue 5 | JOCR November-December 2016 | Page 62-64| Andrew M Steffensmeier, Karen Kirkham, John M Wiemann. DOI: 10.13107/jocr.2250-0685.634
Authors: Andrew M Steffensmeier[1], Karen Kirkham[2], John M Wiemann[1]
[1]Department of Orthopedic Surgery, Boonshoft School of Medicine, Wright State University, Dayton, Ohio, United States,
[2]Department of Internal Medicine, Boonshoft School of Medicine, Wright State University, Dayton, Ohio, United States.
Address of Correspondence
Dr. Andrew M Steffensmeier,
Department of Orthopedic Surgery, 240 East Drive, Dayton, Ohio – 45419, United States.
E-mail: Steffensmeier.2@wright.edu
Abstract
Introduction: Avascular necrosis (AVN) of the femoral or humeral heads in patients with sickle cell anemia is a common and painful condition. There is currently no gold standard treatment protocol for this condition. Typically, the pain is managed with narcotics and activity restriction until there has been collapse of the subchondral bone with a degree of arthrosis sufficient to warrant total joint arthroplasty. This method entails prolonged pain for the patient and decreases the ability to function occupationally and recreationally.
Case Report: A 51-year-old African-American woman with a history of sickle cell anemia presented for the evaluation of significant bilateral shoulder pain that was confirmed to be AVN via radiographs and magnetic resonance imaging of both her humeral heads without joint collapse. She tried and failed conservative management with physical therapy and optimization of sickle cell treatment with pain medications for years, so she desired surgical management. Arthroscopically assisted core decompression of her humeral heads with synthetic grafting was performed in an attempt at joint preservation.
Conclusion: This report demonstrates a technique of staged decompression of necrotic bone in the bilateral humeral heads with synthetic bone grafting to determine if this could function as a joint preservation strategy. This procedure was considered successful to alleviate the patients’ pain in both of her arms. The application of this procedure is significant because it could be used in various future medical joint preservation cases for a wide range of patients.
Keywords: Synthetic bone graft, sickle cell anemia, humeral head.
Introduction
Avascular necrosis (AVN) of the femoral and humeral heads is a frequent and debilitating finding in many patients with sickle cell anemia [1, 2, 3, 4]. The standard treatment is observation with symptomatic pain control until the arthrosis has progressed to the point requiring total joint arthroplasty [5, 6, 7, 8]. There is a lack of published research with regard to joint preservation strategies in this patient population with new data starting to be published on the outcomes of core decompression and arthroplasty on atraumatic osteonecrosis [6]. This case illustrates a patient with bilateral humeral head AVN in which staged decompression of the necrotic bone with synthetic bone grafting was performed as a joint preservation strategy. It is our goal to delay end-stage arthrosis and cartilaginous degeneration with early intervention.
Case Report
A 51-year-old African-American woman with a history of sickle cell anemia presented for the evaluation of significant bilateral shoulder pain that was interfering with her activities of daily living and requiring narcotic medication for pain control. The pain and disability had been increasing progressively over several years and was recalcitrant to physical therapy. Radiographs and magnetic resonance imaging (MRI) confirmed AVN of her humeral heads without joint collapse (Fig. 1).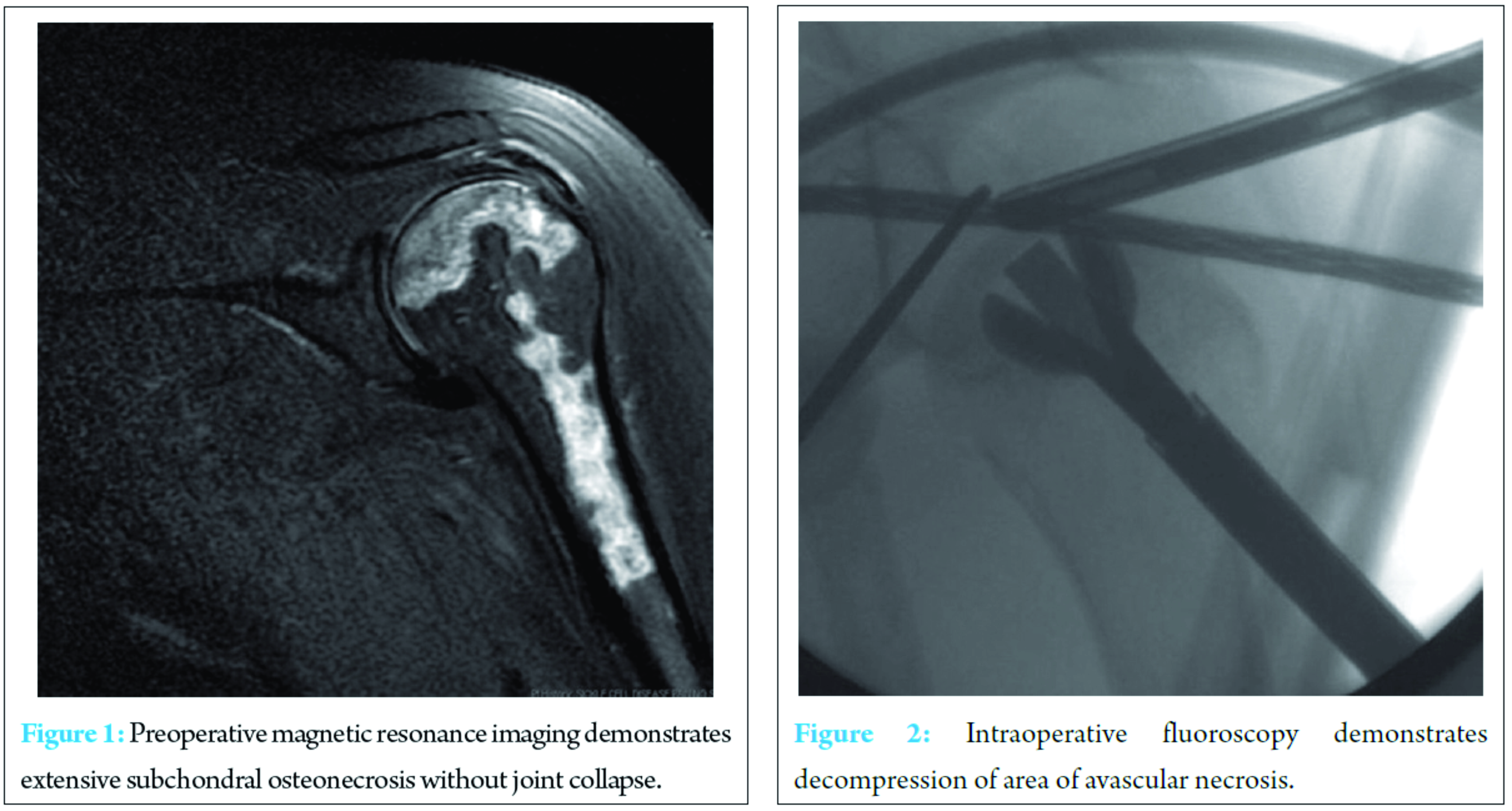
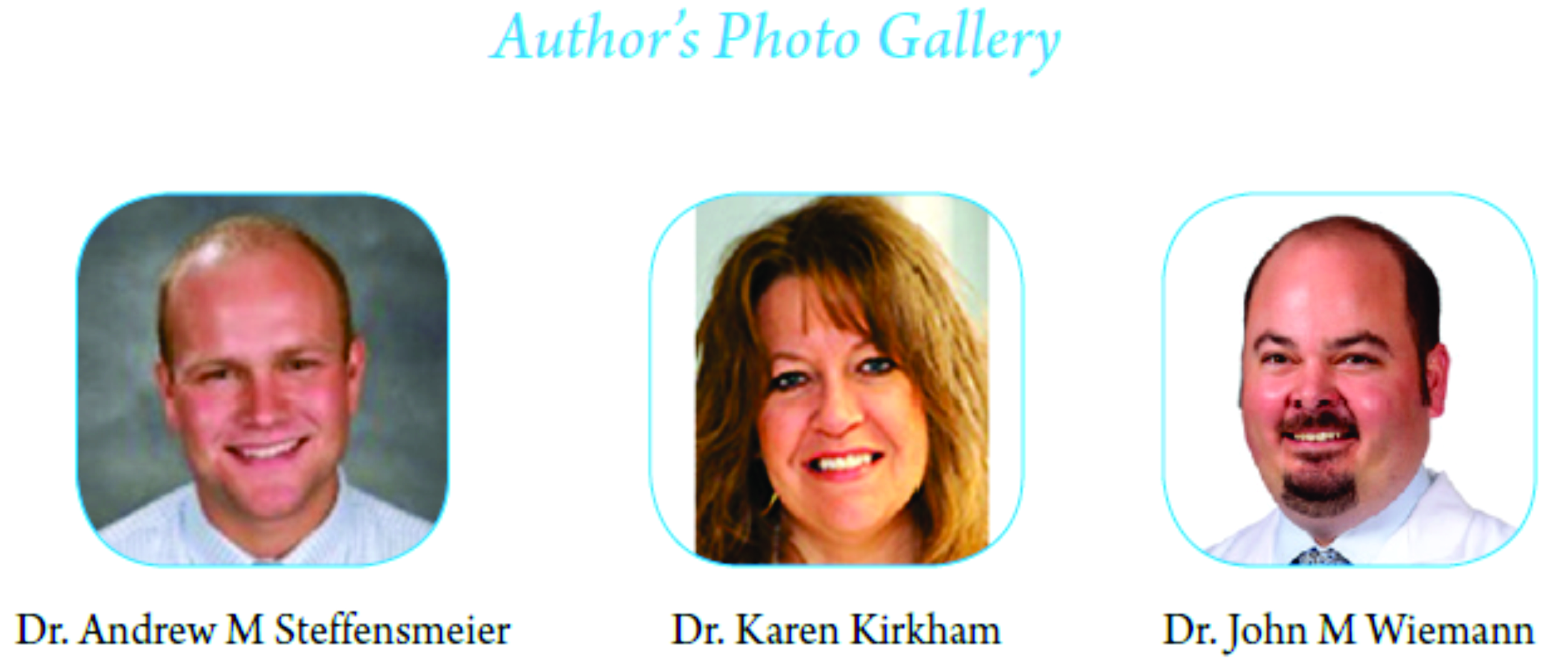
Staged surgery was then performed approximately 4-month apart using the identical technique on both shoulders. Our standard perioperative protocol for sickle cell patients was utilized. This consists of admission the evening before surgery to the internal medicine service with acquisition of routine blood work, intravenous hydration, and preoperative blood transfusion as indicated based on hemoglobin level [9]. Surgery was performed in the beach chair position with the c-arm coming in perpendicular to the patient. Diagnostic arthroscopy was performed to evaluate for intra-articular pathology and confirm that there was no significant chondromalacia, which would negate the benefits of the joint preservation procedure. In this case, arthroscopy revealed small partial thickness articular sided supraspinatus tears that were debrided but no visible chondral damage was present. Upon probing, the cartilage was quite soft over the areas of AVN noted on MRI. Under fluoroscopic guidance, a guide wire was directed into the center of the region of AVN, which was done via a small deltoid splitting approach laterally. The arthroscopic probe was placed in the center of the most depressible cartilage region on the head and utilized fluoroscopically to guide pin placement. Once the guide wire was in the center of the defect, an expandable reamer was utilized and the necrotic bone was removed (Fig. 2). 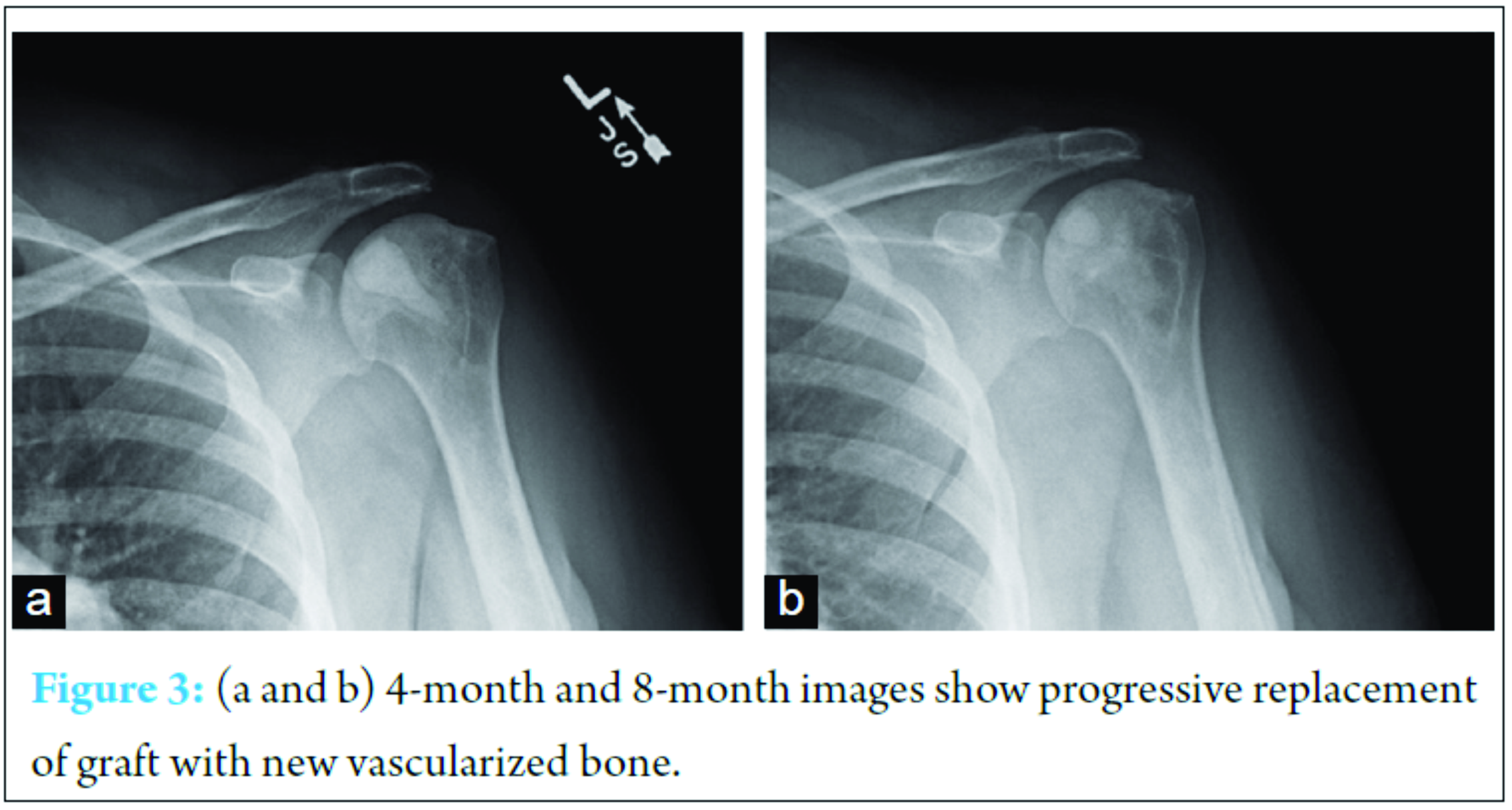 The arthroscope is critical in this stage to allow complete extraction of necrotic subchondral bone while ensuring no penetration of the cartilage. After full decompression was performed, synthetic bone graft (PRO-DENSE, Wright Medical) was injected under fluoroscopy and direct visualization. Given the immediate structural integrity of the graft, maximal removal of necrotic segments was attempted. Care was taken under fluoroscopic guidance not to penetrate the articular surface and no cartilaginous defects were encountered. For both procedures, the standard sickle cell protocol was followed with overnight admission for intravenous hydration followed by discharge with 2 weeks of deep venous thrombosis (DVT) chemoprophylaxis. She was allowed activity as tolerated and physical therapy initiated 2 weeks after each surgery. At 8-month follow-up from the index procedure, she is asymptomatic with a full range of motion on the first shoulder and some mild residual stiffness in the second shoulder (4-month follow-up). Radiographs demonstrate incorporation of the bone graft without evidence of joint collapse or further AVN (Fig. 3).
The arthroscope is critical in this stage to allow complete extraction of necrotic subchondral bone while ensuring no penetration of the cartilage. After full decompression was performed, synthetic bone graft (PRO-DENSE, Wright Medical) was injected under fluoroscopy and direct visualization. Given the immediate structural integrity of the graft, maximal removal of necrotic segments was attempted. Care was taken under fluoroscopic guidance not to penetrate the articular surface and no cartilaginous defects were encountered. For both procedures, the standard sickle cell protocol was followed with overnight admission for intravenous hydration followed by discharge with 2 weeks of deep venous thrombosis (DVT) chemoprophylaxis. She was allowed activity as tolerated and physical therapy initiated 2 weeks after each surgery. At 8-month follow-up from the index procedure, she is asymptomatic with a full range of motion on the first shoulder and some mild residual stiffness in the second shoulder (4-month follow-up). Radiographs demonstrate incorporation of the bone graft without evidence of joint collapse or further AVN (Fig. 3).
Discussion
There are no published articles on surgical shoulder joint preservation in sickle cell anemia to the authors knowledge. In this report, we show a potential method to mitigate this process and prevent or delay the need for total joint arthroplasty with early intervention. Synthetic grafting with an injectable calcium sulfate and calcium phosphate composition (PRO-DENSE) has been shown to be effective in allowing relatively rapid bone regrowth in the setting of femoral head AVN [10, 11]. Removal of necrotic bone back to healthy vascularized bone with interposition of a structurally strong osteoconductive substrate allows for gradual revascularization and re-ossification of the region. While decompression and grafting will not change the underlying sickle cell disease process, it is our hope to provide improved the quality of life for these patients. Further study is required to demonstrate the long-term efficacy of joint preservation strategies in the humeral heads of sickle cell patients with humeral head AVN before evidence of cartilaginous damage. In terms of indications and contraindications or inclusion and exclusion criteria, we do not feel that joint preservation strategies would be effective after the onset of subchondral collapse, rather in the setting of MRI-confirmed symptomatic AVN with intact cartilage. The risk profile of any surgical intervention in the setting of sickle cell anemia must also be considered, with appropriate care taken to prevent acute sickle crisis, DVT, and pulmonary embolism. Therefore, coordination with an established sickle cell program is critical to ensure appropriate pre-hydration, transfusion, and anticoagulation protocols are followed to prevent perioperative medical complications. There is no known increased risk in this patient population to using the bone graft material, so the main consideration for contraindications are related to the surgical risk of a sickle cell patient and how well his or her disease is being managed.
Conclusion
AVN is a common problem for patients with sickle cell disease and this report demonstrates a technique of staged decompression of necrotic bone in the bilateral humeral heads with synthetic bone grafting to determine if this could function as a joint preservation strategy. This procedure was considered successful to alleviate the patients’ pain in both of her arms (bilateral humeral heads). The application of this procedure is significant because it could be used in various future medical joint preservation cases for a wide range of patients.
Clinical message
Joint degeneration and long-term pain are common outcomes of sickle cell anemia and other disease processes. While decompression and grafting will not change the underlying disease process, it is our hope to provide improved the quality of life for these patients using this procedure. Our goal is to apply this joint preservation technique to more sickle cell patients and patients with other diseases causing joint pain and degeneration to improve not only the quality of joint function, but also the quality of life.
References
1. David HG, Bridgman SA, Davies SC, Hine AL, Emery RJ. The shoulder in sickle-cell disease. J Bone Joint Surg Br 1993;75(4):538-545.
2. Hanker GJ, Amstutz HC. Osteonecrosis of the hip in the sickle-cell diseases. Treatment and complications. J Bone Joint Surg Am 1988;70(4):499-506.
3. Milner PF, Kraus AP, Sebes JI, Sleeper LA, Dukes KA, Embury SH, et al. Osteonecrosis of the humeral head in sickle cell disease. Clin Orthop Relat Res 1993;289:136-143.
4. Gruson KI, Kwon YW. Atraumatic osteonecrosis of the humeral head. Bull NYU Hosp Jt Dis 2009;67(1):6-14.
5. LaPorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS. Osteonecrosis of the humeral head treated by core decompression. Clin Orthop Relat Res 1998;355:254-260.
6. Kennon JC, Smith JP, Crosby LA. Core decompression and arthroplasty outcomes for atraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2016;25(9):1442-1448.
7. Mansat P, Huser L, Mansat M, Bellumore Y, Rongières M, Bonnevialle P. Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14(2):114-120.
8. Lau MW, Blinder MA, Williams K, Galatz LM. Shoulder arthroplasty in sickle cell patients with humeral head avascular necrosis. J Shoulder Elbow Surg 2007;16(2):129-134.
9. Buck J, Casbard A, Llewelyn C, Johnson T, Davies S, Williamson L. Preoperative transfusion in sickle cell disease: A survey of practice in England. Eur J Haematol 2005;75(1):14-21.
10. Evaniew N, Tan V, Parasu N, Jurriaans E, Finlay K, Deheshi B, et al. Use of a calcium sulfate-calcium phosphate synthetic bone graft composite in the surgical management of primary bone tumors. Orthopedics 2013;36(2):e216-e222.
11. Kumar CY, K B N, Menon J, Patro DK, B H B. Calcium sulfate as bone graft substitute in the treatment of osseous bone defects, a prospective study. J Clin Diagn Res 2013;7(12):2926-2928.
| How to Cite This Article: Steffensmeier AM, Kirkham K, Wiemann JM. Core Decompression with Synthetic Grafting as a Joint Preservation Strategy in Humeral Avascular Necrosis Due to Sickle Cell Anemia: A Case Report. Journal of Orthopaedic Case Reports 2016 Nov-Dec;6(5):62.64. Available from: https://www.jocr.co.in/wp/2016/11/10/2250-0685-634-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2023 Osteonecrosis of the Humeral Head Following Arthroscopic Repair of Rotator Cuff Tears: A Case Report
December 10, 2023 Osteonecrosis of the Humeral Head Following Arthroscopic Repair of Rotator Cuff Tears: A Case Report June 7, 2021 Single-Stage Bilateral Stemless Shoulder Hemiarthroplasty using a Subscapularis-Sparing Approach for Bilateral Dysbaric Osteonecrosis of the Humeral Head in a Diver: A Case Report
June 7, 2021 Single-Stage Bilateral Stemless Shoulder Hemiarthroplasty using a Subscapularis-Sparing Approach for Bilateral Dysbaric Osteonecrosis of the Humeral Head in a Diver: A Case Report January 2, 2016 Melorheostosis of the Foot: A Case Report of A rare entity with a Review of Multimodality Imaging Emphasizing the Importance of Conventional Radiography in Diagnosis
January 2, 2016 Melorheostosis of the Foot: A Case Report of A rare entity with a Review of Multimodality Imaging Emphasizing the Importance of Conventional Radiography in Diagnosis July 10, 2024 Surgical Tips: Managing the Orthopedic Traction Table on Gritti-Stokes Amputated Patients
July 10, 2024 Surgical Tips: Managing the Orthopedic Traction Table on Gritti-Stokes Amputated Patients


