
[box type=”bio”] What to Learn from this Article?[/box]
Mangled upper limb injuries behave differently from lower limb injuries.
Case Report | Volume 7 | Issue 1 | JOCR January – February 2017 | Page 3-8 | R Siva Kumar, Prahalad Kumar Singhi, M Chidambaram. DOI: 10.13107/jocr.2250-0685.662
Authors: R Siva Kumar[1], Prahalad Kumar Singhi[1], M Chidambaram[1]
[1]Department of Orthopaedics, Preethi Hospitals Pvt. Ltd., Madurai, Tamil Nadu, India.
Address of Correspondence
Dr. R Siva Kumar,
Department of Orthopaedics, Preethi Hospitals Pvt. Ltd., 120 Feet Road, Ganesh Nagar, Near Mattuthavani Bus Stand, Madurai – 625 007, Tamil Nadu, India.
E-mail: profsivakumarspine@gmail.com
Abstract
Introduction: Mangled upper limb injuries are at surge because of industrialization, modernization, and severe motor vehicle accidents. The utility of various scoring systems are meant for decision making in mangled lower limb injuries, and the same have been extrapolated for mangled upper limb injuries to make a decision of salvage or amputation for the lack of separate scoring system.
Materials and Methods: We applied mangled extremity severity score (MESS) and mangled extremity syndrome index (MESI) scoring systems to 10 cases of mangled upper limb injuries during the period of November 2010 to September 2012 presented at our tertiary trauma care center. Average MESS score was 7.7 and MESI score was 18.1. Above elbow, amputation was needed in three patients, and salvage procedure was done in rest of the seven patients. All the patients were subjected to salvage procedure initially unless life threatening because of mangled limb injury. MESS scores over 7, MESI score over 20 is accepted for amputation in lower limbs, but could not be justified in our study for MESS whereas MESI was more reliable. Functional outcome was assessed using visual analog scale score and short form-36 (SF-36) score for all patients, which was satisfactory, elderly and diabetic patients were relatively less satisfied.
Conclusions: (a) Upper limb and lower limb mangled injuries cannot be considered same because of their anatomy. The upper limb has more rich vascularity and efficient collaterals, small muscle mass, so ischemia time is relatively more. Therefore, the different scoring systems are needed for both. (b) In our case series, MESI scoring was more reliable then MESS score, but this needs a large prospective study to validate it. (c) Salvage should be prime realistic aim influenced by several factors. Prosthesis for upper limb is very expensive and not well tolerated, so even a woody limb is well accepted in our patients.
Keywords: Mangled upper limb injury, salvage or amputation, scoring system.
Introduction
Mangled injury is a descriptive term which explains severity of the limb injury affecting severely at least 3 of 5 major components such as skin, soft tissue, bones, nerve and artery, usually caused by high velocity injuries [1] like motor vehicle accidents (MVAs), blast injury and crush injury (work spot injury). Mangled injury to lower limb is more common than of upper limb, and also most scoring systems have been described for the same. The decision to amputate or salvage is difficult, even for an experienced surgeon [2, 3, 4], and there is no valid scoring system to guide for upper limb injuries. With the evolution in the medical field like advanced bony, soft tissue reconstructive procedures, skeletal stabilization and microvascular procedure salvaging mangled limbs are possible [1, 4]. It also depends on multiple factors, available resources, and socioeconomic status. However, a valid scoring system is the need of hour.
Materials and Methods
Aims and objectives
To apply lower limb mangled injury scoring systems such as mangled extremity severity score (MESS) and mangled extremity syndrome index (MESI) for upper limb mangled extremity in decision-making of salvage or amputation assess the usefulness of these scoring systems and express our experience.
Inclusion criteria
All the patients with severe injury to at least 3 of the 5 components (skin, soft tissue, bone, artery, and nerve) of the upper limb.
Exclusion criteria
Critically injured patient with associated severe injuries (life threatening) with mangled upper limb injuries was excluded from the study.
We prospectively studied 10 cases presented to our trauma center from November 2010 to September 2012 with severe mangled upper extremity injury. Advanced trauma life support protocol was followed on receiving the patient in the emergency room and once patient was hemodynamically stabilized. MESS and MESI scores were applied initially in emergency room and later in operation theater. Arterial continuity was assessed by palpating the pulse or capillary reperfusion (capillary refill), in doubtful cases arterial Doppler or magnetic resonance (MR) angiogram was done. X-rays were taken to assess fractures and bony injuries, and appropriate investigations such as computed tomography scan and magnetic resonance imaging was done to assess associated injuries of head, chest, spine, and abdomen. A standard treatment protocol was followed, initial skeletal stabilization and wound debridement was done unless contraindicated (life threatening). Later on repetitive debrima, reconstructive procedures or delayed amputations were done depending on the survivability of limb and general condition of the patient. Our study had eight male and two female patients, seven had right and other three left side mangled upper limb injuries and all were right-handed dominant patients. MVA was mode of injury in seven, two had work spot injury, and one was a cracker blast injury. Average age of the patient was 35.8 years (minimum was 6 years and maximum 58 year). Average hospital stay was 36 days; maximum was 85 days in a patient. MESS score was above 7 in all patients, i.e., average MESS score 7.7 and average MESI score was 18.1. All patients presented to us within 6-18 h of injury except one patient who presented after 24 h. All patients had primary treatment, first aid taken elsewhere and later presented to us. Associated injuries were present in five patients such as chest injury, head injury, and lower limb injury were appropriately managed.
Primary wound debridement and skeletal stabilization was done in all patients except one where primary amputation was done (as patient was brought in septic shock) however following multiple procedures, salvage was achieved in seven patients (Fig. 1, 2, 3, 4a and b). Delayed amputation was later needed in two patients (Fig. 5a, b, 6 and 7).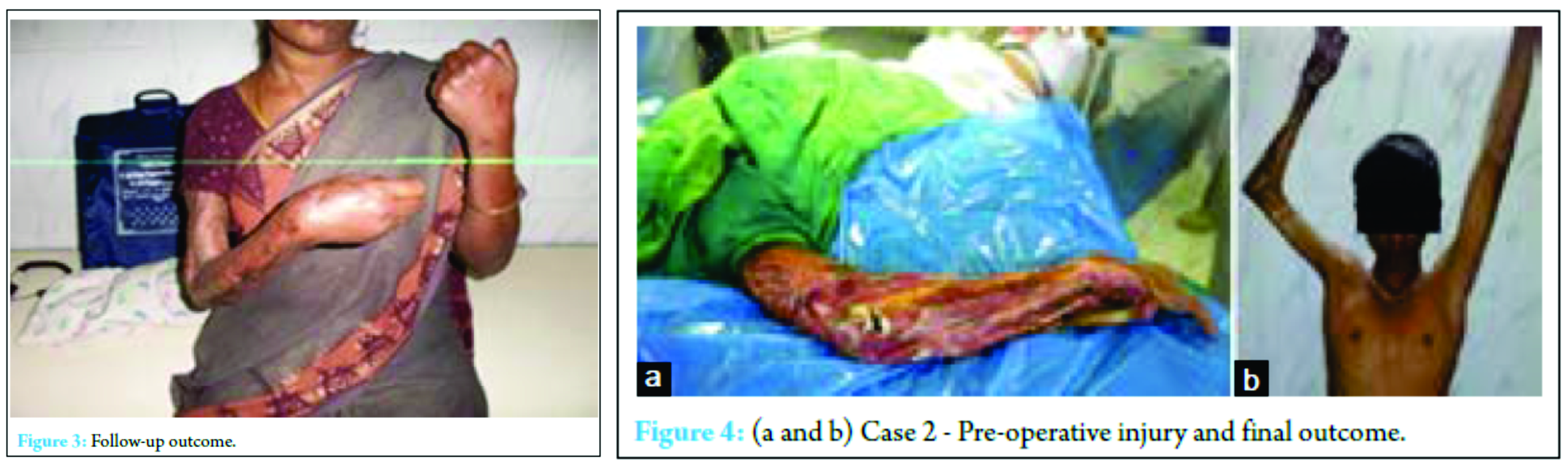
Reasons for delayed amputation – In three cases where amputation was done, MESS score was 8, 9, 9 and MESI score was 22, 21, and 20, respectively.  Initial debridement and skeletal fixation were done in two patients, and primary amputation was done in one case that was diabetic and in toxic state. Of the other two cases, one patient developed crush syndrome and was later taken for above elbow (AE) amputation on the third post-operative day. The third case was a blast injury that presented to us after 24 h had extensive muscle necrosis of arm and forearm with infection and associated with Grade III B compound fracture both bone leg with prolonged shock, initial debridement done, but as he was moving into septicemia, AE amputation was done on fifth post-operative day.
Initial debridement and skeletal fixation were done in two patients, and primary amputation was done in one case that was diabetic and in toxic state. Of the other two cases, one patient developed crush syndrome and was later taken for above elbow (AE) amputation on the third post-operative day. The third case was a blast injury that presented to us after 24 h had extensive muscle necrosis of arm and forearm with infection and associated with Grade III B compound fracture both bone leg with prolonged shock, initial debridement done, but as he was moving into septicemia, AE amputation was done on fifth post-operative day.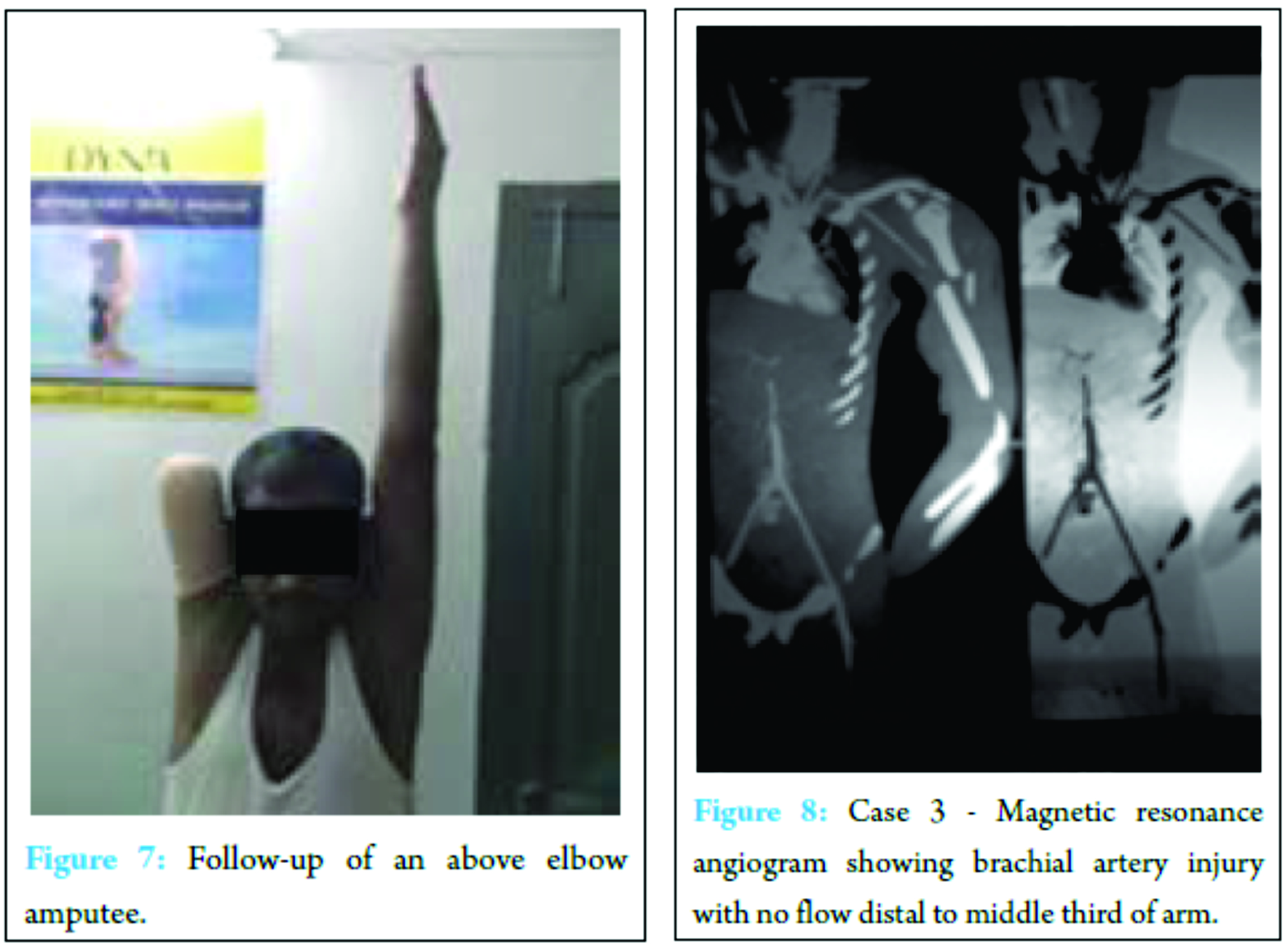
The rest of seven cases also had MESS score of 7 and over and MESI score of under 20, where thorough wound debridement and skeletal stabilization was done. Later multiple debridement, soft tissue and bony reconstructive procedures were done to achieve the salvage of the limb.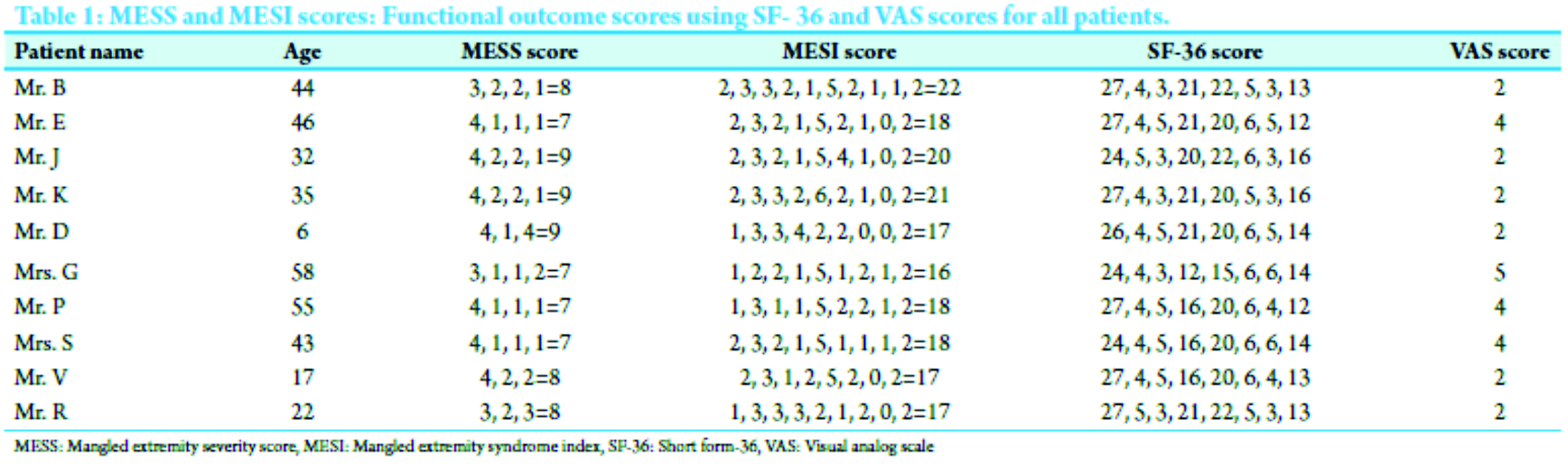
Two patients had complete occlusion of brachial artery with no collateral flow confirmed using MR angiogram. In first case (Fig. 8) brachial artery repair using vein graft, debridement and humeral shortening at fracture site with conservative management of the avulsion injury of brachial plexus was done. Limb was salvaged with good vascularity and the fracture united well but wrist drop persist. The second case was a 6-year-old boy for who repeated debridement was done, as artery was irreparable, but had capillary refill, so vacuum-assisted closure was applied twice to improve vascularity and soft tissue bed for skin coverage.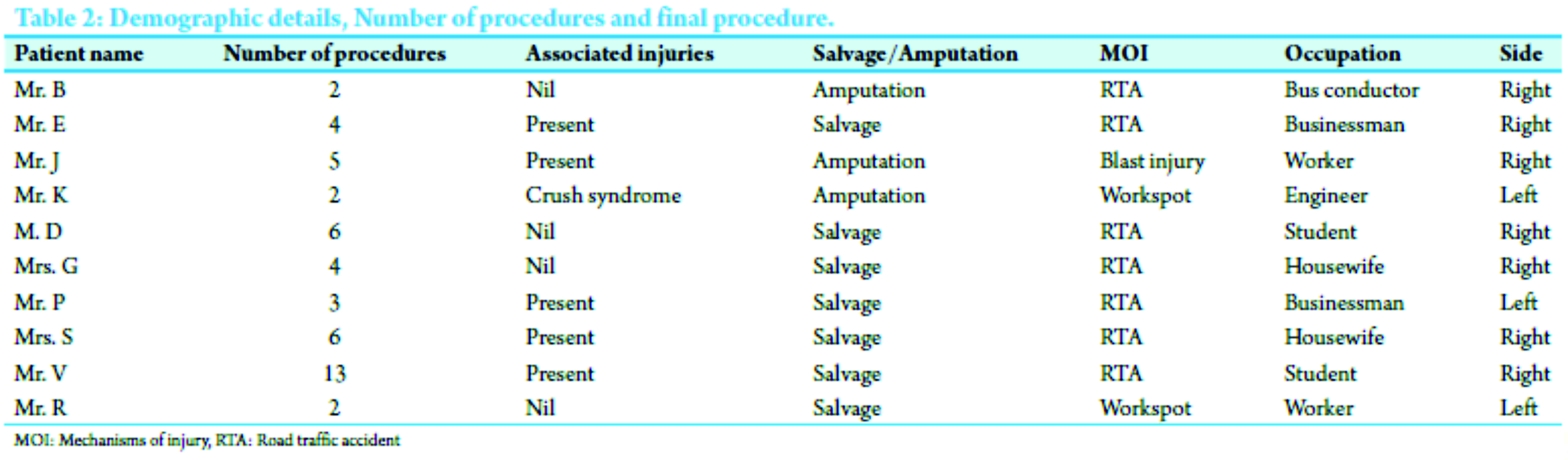
Multiple procedures were done in all patients, average number of 4.4 procedures, and maximum of 13 procedures in a case that also had associated lower limb injury.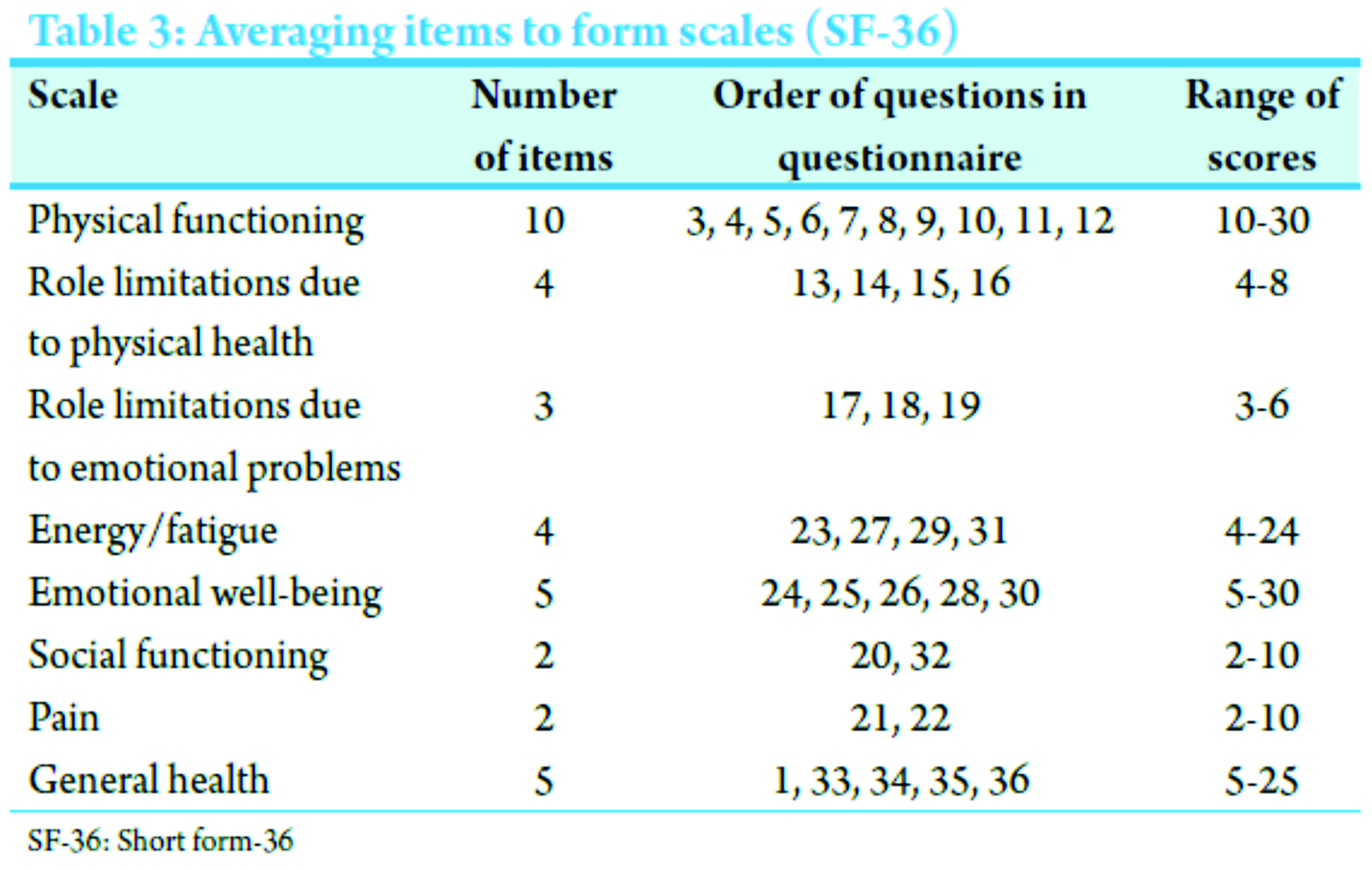
Results
MESS score ranged from 7 to 9 and MESI score from 16 to 22 (Table 1 and 2). Amputation was done in three cases, primarily in one and delayed in two cases that developed crush syndrome and toxicity as a life-saving procedure. In rest of the seven cases, successful limb salvage was obtained, arterial repair was done in one case, ulnar nerve repair in two cases. Initial skeletal stability and later soft tissue reconstructive procedures were done in all cases, satisfactory bony union and soft tissue coverage obtained in due course with a reasonable functional limb which enables to do certain activities of daily living. The final functional outcome in all 10 patients was satisfactory assessed using short form-36 (SF-36) questionnaire and visual analog scale (VAS) score for pain done at the end of 1 year follow-up (scoring done in Table 3). Pain on VAS score was more in elderly diabetic patients who were salvaged and also the SF-36 was relatively less satisfactory.
Discussion
Mangled upper limb injuries are less common as compared to lower limb and also most of the scoring systems are meant for lower limb injuries. The utility of various scoring systems are infallible and not useful. These are two extreme points of view, which are not true. In doubtful situations, they provide additional guidelines in the management of the problems, which enables to make a decision of salvage or amputation [1]. The most widely used scoring systems are MESS [2], MESI [3], predictive salvage index [4], and the nerve injury, ischemia, soft tissue injury, skeletal injury, shock, and age of patient (needs imminent salvage so abandon) score, Hannover fracture scale-97, Ganga hospital score (GHS) [1]. Most of them have been meant for mangled lower limb injuries [1, 6]. However, MESS and MESI have been used for upper limb injuries in few literatures [2, 3]. In MESS and MESI scoring systems for mangled lower limb extremity a cutoff score of 7 and 20, respectively, is generally considered for amputation. The scoring systems have been described to enable the treating surgeon to take a decision. Several criteria like tertiary center with multispecialty, and microsurgical team, injury pattern, pre-existing co-morbidities influence the outcome [1]. Amputation will be unpleasant, not easily acceptable by the patient and relatives, at the same time prolonged attempts to salvage the limb with unsuccessful results may prove to be disastrous in terms of patient life and money [1]. Furthermore, these systems fail to consider factors related to patient’s quality of life, pain, occupation, age, wishes social support system, family status, financial resources, training, and expertise of treating surgical team [1]. Although these considerations are more subjective, undoubtedly they are very important. Enthusiastic decision to salvage the limb based on microsurgical techniques and expertise alone may not be wise; it will be costlier and sometimes lethal affair [6, 7]. Hansen characterized this approach as triumphs over reason [8]. Tornetta and Olson [9] reported that heroic attempt to salvage a limb may render the patient depressed, divorced, unemployed and significantly disabled. Patient and family have to be realized that both salvage and early amputation by no means can reassure that the patient will return to normal pain-free extremity [10]. Bondurant et al. [11] compared primary versus delayed amputation and reported increased risk of sepsis and infective complications in delayed amputation. The affordability of the treatment by the family members is an important deciding factor, as the salvage procedures end up with huge medical bills. The emotional aspects following primary as compared to delayed amputations and salvage procedures demonstrated that early amputation on the basis of appropriate criteria had improved function and limited the long-term complications [8, 11, 12]. MESS is the only one that derives from a study with a prospective validation trial. The authors used this system because of its simplicity and its ability to score at the time of the initial evaluation without direct observation in the operating room, though MESS was not designed to have 100% specificity and 100% positive predictive value in these injuries [14]. Weak point of this scoring system is its limited sensitivity and negative predictive value when compared to MESI for the upper extremities [14]. In our study, MESI was more accurate than MESS to predict amputation. However, Togawa et al. [15] challenged utility of MESS score stating muscle mass is small as compared to lower limb [16] so factors contributing to the development of crush syndrome are reduced; second upper limb has well-developed collateral circulation. There is no artery in upper limb like popliteal artery in the lower limb which produces ischemia primarily as a result of single major arterial injury, also the critical time allowed to reperfusion in the arm is 8-10 hrs [17, 18] which are 6 h limit for lower limb [2]. Hyperbaric oxygen therapy improves ischemia [19, 20]. These factors make the MESS scoring inappropriate for application to the upper limb and make it necessary to establish a suitable alternative scoring system [1, 21]. This was the reason we also utilized MESI score to enable us to take a decision. The lower extremity assessment project [13] was a prospective longitudinal study conducted at level 1 trauma center in United States for the treatment of high-energy trauma of lower extremities they concluded that the scores were quite useful in predicting limb salvage, but the opposite, i.e., decision to amputate was not true. All the scores in the series had low sensitivity and could not be accurate predictors of amputation. The acceptance of amputation, the social stigma and psychological impact of amputation are quite different in various societies and geographical regions of the globe [1]. Furthermore, the upper limb prosthesis is usually less well tolerated as compared to lower limb, so even a non-functional woody upper limb is also well accepted in our country.
Conclusions
Upper limb and lower limb mangled injuries cannot be considered same, because of their anatomy. Upper limb has more rich vascularity and efficient collaterals, small muscle mass, so ischemia time is relatively more. Therefore, different scoring systems are needed for both. In our case series, MESI scoring was more reliable then MESS scoring, but this needs a large prospective study to validate it. Salvage should be prime realistic aim influenced by several factors. Prosthesis for upper limb is very expensive and not well tolerated, so even a woody limb is well accepted in our patients.
Acknowledgments
Entire Department of Orthopaedics, Preethi Hospitals Pvt. Ltd.
Clinical Message
A mangled upper limb injury has to be individualized and needs a valid scoring system. Salvage should always be a priority. Even a woody non-functional limb is well accepted in our patients.
References
1. Shanmuganathan R. The utility of scores in the decision to salvage or amputation in severely injured limbs. Indian J Orthop 2008;42(4):368-376.
2. Johansen K, Daines M, Howey T, Helfet D, Hansen ST Jr. Objective criteria accurately predict amputation following lower extremity trauma. J Trauma 1990;30(5):568-572.
3. Gregory RT, Gould RJ, Peclet M, Wagner JS, Gilbert DA, Wheeler JR, et al. The mangled extremity syndrome (M.E.S.): a severity grading system for multisystem injury of the extremity. J Trauma 1985;25(1):1147-1150.
4. Howe HR Jr, Poole GV Jr, Hansen KJ, Clark T, Plonk GW, Koman LA, et al. Salvage of lower extremities following combined orthopedic and vascular trauma. A predictive salvage index. Am Surg 1987;53(4):205-208.
5. McNamara MG, Heckman JD, Corley FG. Severe open fractures of the lower extremity: a retrospective evaluation of the Mangled Extremity Severity Score (MESS). J Orthop Trauma 1994;8(2):81-87.
6. Dirschl DR, Dahners LE. The mangled extremity: When should it be amputated? J Am Acad Orthop Surg 1996;4(4):182-190.
7. Tomaino MM, Bowen CV. Unsatisfactory outcome after lower limb salvage: decision-making pitfalls. Am J Orthop (Belle Mead NJ) 1998;27(7):526-529.
8. Hansen ST Jr. The Type-IIIC tibial fracture. Salvage or amputation. J Bone Joint Surg Am 1987;69(6):799-800.
9. Tornetta P 3rd, Olson SA. Amputation versus limb salvage. Instr Course Lect 1997;46:511-518.
10. MacKenzie EJ, Bosse MJ, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Joint Surg Am 2005;87(8):1801-1809.
11. Bondurant FJ, Cotler HB, Buckle R, Miller-Crotchett P, Browner BD. The medical and economic impact of severely injured lower extremities. J Trauma 1988;28(8):1270-1273.
12. Hansen ST Jr. Overview of the severely traumatized lower limb. Reconstruction versus amputation. Clin Orthop Relat Res 1989;243:17-19.
13. Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. A prospective evaluation of the clinical utility of the lower-extremity injury-severity scores. J Bone Joint Surg Am 2001;83-A(1):3-14.
14. Durham RM, Mistry BM, Mazuski JE, Shapiro M, Jacobs D. Outcome and utility of scoring systems in the management of the mangled extremity. Am J Surg 1996;172(5):569-573.
15. Togawa S, Yamami N, Nakayama H, Mano Y, Ikegami K, Ozeki S. The validity of the mangled extremity severity score in the assessment of upper limb injuries. J Bone Joint Surg Br 2005;87(11):1516-1519.
16. Clarys JP, Marfell-Jones MJ. Soft tissue segmentation of the body and fractionation of the upper and lower limbs. Ergonomics 1994;37(1):217-229.
17. Wang SH, Young KF, Wei JN. Replantation of severed limbs – Clinical analysis of 91 cases. J Hand Surg Am 1981;6(4):311-318.
18. Wood MB, Cooney WP 3rd. Above elbow limb replantation: functional results. J Hand Surg Am 1986;11(5):682-687.
19. Myers RA. Hyperbaric oxygen therapy for trauma: crush injury, compartment syndrome, and other acute traumatic peripheral ischemias. Int Anesthesiol Clin 2000;38(1):139-151.
20. Bouachour G, Cronier P, Gouello JP, Toulemonde JL, Talha A, Alquier P. Hyperbaric oxygen therapy in the management of crush injuries: a randomized double-blind placebo-controlled clinical trial. J Trauma 1996;41(2):333-339.
21. Lin CH, Wei FC, Levin LS, Su JI, Yeh WL. The functional outcome of lower-extremity fractures with vascular injury. J Trauma 1997;43(3):480-485.
| How to Cite This Article: Kumar RS, Singhi PK, Chidambaram M. Are We Justified Doing Salvage or Amputation Procedure Based on Mangled Extremity Severity Score in Mangled Upper Extremity Injury. Journal of Orthopaedic Case Reports 2017 Jan-Feb;7(1): 3-8. Available from: https://www.jocr.co.in/wp/wp-content/uploads/5.-2250-0685.662.pdf |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


