
[box type=”bio”] Learning Points for this Article: [/box]
The multiplanar external fixation can be used as a definitive treatment alternative in pediatric open defective supracondylar humerus fracture.
Case Report | Volume 7 | Issue 5 | JOCR Sep-Oct 2017 | Page 84-88 | Mehmet Demirel, Onur Tunali, Ismail Turkmen, Yavuz Saglam. DOI: 10.13107/jocr.2250-0685.908
Authors: Mehmet Demirel [1], Onur Tunali [2], Ismail Turkmen [3], Yavuz Saglam [4]
[1] Department of Orthopedic and Traumatology, Istanbul University, Istanbul Faculty of Medicine, Millet cad, Vatan bulvarı, Fatih, Çapa, Istanbul – 34100, Turkey
[2] Department of Orthopedic and Traumatology, Maslak Acibadem Hospital, Atakoy 4. Kisim, TO 211, Daire: 10, Bakirkoy, Istanbul, Turkey
[3] Department of Orthopedic and Traumatology, Umraniye Training and Research Hospital, Elmalıkent, Adem Yavuz Cd. No:1, 34766 Ümraniye, Istanbul, Turkey
[4] Department of Orthopedic and Traumatology, Biruni University Hospital, Beşyol, Eski Londra Asfaltı No:10, 34295 Küçükçekmece, Istanbul, Turkey.
Address of Correspondence
Dr. Mehmet Demirel,
Department of Orthopedic and Traumatology Istanbul University,
Istanbul Faculty of Medicine, Millet cad,
Vatan bulvarı, Fatih, Çapa, Istanbul – 34100, Turkey.
E-mail: dr88.mehmet.demirel@gmail.com
Abstract
Introduction: Although supracondylar fractures of the humerus are common in children, open fractures of are extremely rare injuries. Gustilo-Anderson Type-III fractures in the upper extremity are primarily associated with considerable bone loss resulting from high energy trauma. In this study, a case of open pediatric supracondylar humerus fracture treated by a joint and defect spanning multiplanar tubular external fixation is presented.
Case Report: A boy aged 3 years suffered from a Gustilo-Anderson Type-IIIA supracondylar humerus fractures. There was no neurovascular compromise. Intravenous antibiotic regimen was introduced. A joint and defect spanning multiplanar tubular external fixation was employed within 4 h of the accident. After the operation, the patient was closely followed in the inpatients unit. The external fixator was removed in the 6th week of follow-up, and range of motion exercises was started. With the exception of limited flexion of the elbow in 12th month of follow-up, supination and pronation were full. At the 48th month follow-up, 120° of elbow flexion, full extension, and full forearm rotation were observed. Physical examination showed 15° change in carrying angle to cubitus varus; radiologic examination showed a slight varus angulation of the distal humerus, a decreased Baumann’s angle. The Mayo elbow performance score was 100 points.
Conclusion: When taking into account the high remodeling capacity, healing potential, and greater resistance to joint stiffness in fractures of children, joint and external fixators appear as a viable definitive treatment in such cases.
Keywords: Open pediatric fracture, supracondylar humerus, bone loss, external fixator.
Introduction
Open fractures of the upper extremity are rare injuries in childhood and are generally seen in the distal humerus and forearm. Concomitant bone loss and soft tissue injuries are normally unexpected injuries because the majority of these fractures result from low energy trauma. However, Gustilo-Anderson Type-III fractures of the arm are primarily associated with considerable bone loss and soft tissue injuries due to high energy trauma [1]. Even though supracondylar fractures of the humerus are common in children, open supracondylar fractures are extremely rare, accounting for 1% of all supracondylar fractures [2]. In this article, with excellent functional and radiograph outcomes, a unique patient who underwent osteosynthesis with joint and defect spanning multiplanar tubular external fixation on account of an open supracondylar humerus fracture with bone loss is presented. The purpose of this case report is to give an opinion regarding the management of open supracondylar humerus fractures with bone loss in pediatric populations.
Case Report
A boy aged 3 years was referred to our emergency room after falling from a height of 3 m. He was conscious with slight tachycardia (140 per min). A physical examination revealed a 4 cm skin injury on the posteromedial side of his right elbow. The neurovascular examination was normal with intact radial and ulnar pulses. Antero-posterior and lateral plain radiographs displayed a supracondylar humerus fracture with segmental bone loss. In light of above findings, the initial diagnosis was considered as a Gustilo-Anderson Type-IIIA supracondylar humerus fracture. An intravenous antibiotic regimen was introduced with cefazolin 500 mg 4 times daily for 7 days, gentamicin 40 mg twice daily for 3 days, and metronidazole 200 mg twice daily for 3 days. No additional cranial, chest and abdominal injury were evaluated. The patient was immediately taken to the operating theater, which was within 4 h of the injury. Under general anesthesia, the patient was put to sleep in the supine position without fastening a tourniquet. First, radical debridement was enforced, and a 3 cm × 4 cm segment of avascular and grossly contaminated bone was noted and removed (Fig. 1a, b).
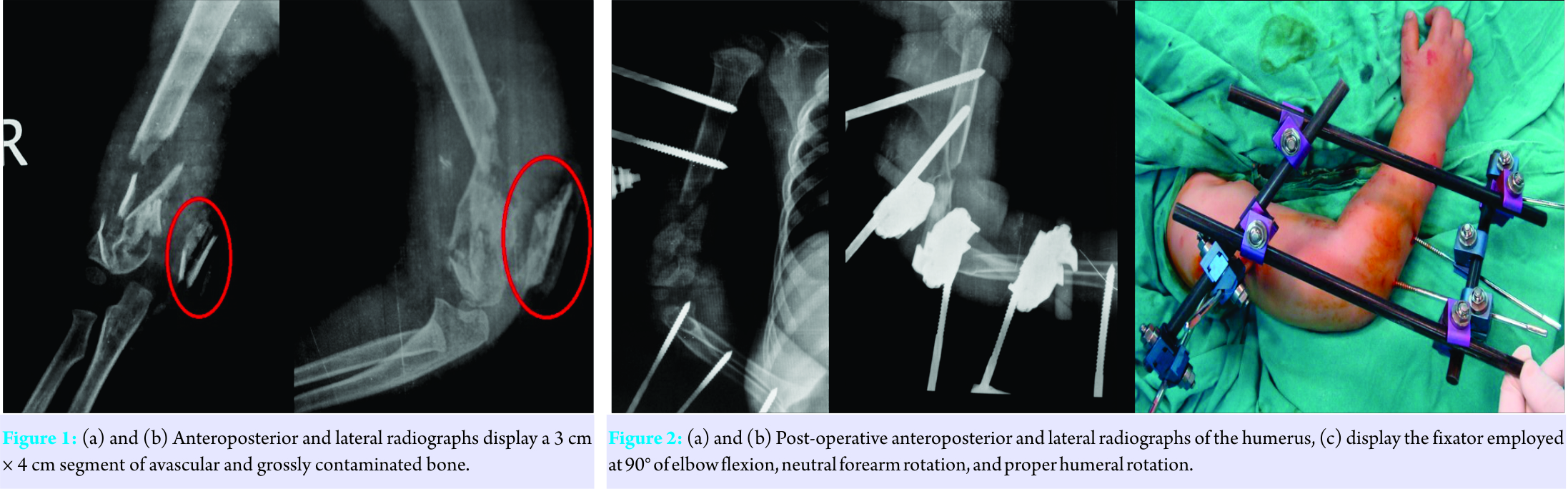
Acceptable thick periosteal coverage was achieved after the debridement of contaminated tissues including the segmental bone. After the repair of the remaining periosteum, the lack of sufficient bone mass in the distal humerus was observed. A defect spanning multiplanar tubular external fixator that bridged the elbow was considered as a suitable choice of treatment to restore the original length of the humerus. After making this decision, a fixator was employed at 90° of elbow flexion, neutral forearm rotation, and proper humeral rotation, to ensure the length and alignment of the humerus (Fig. 2a-c).
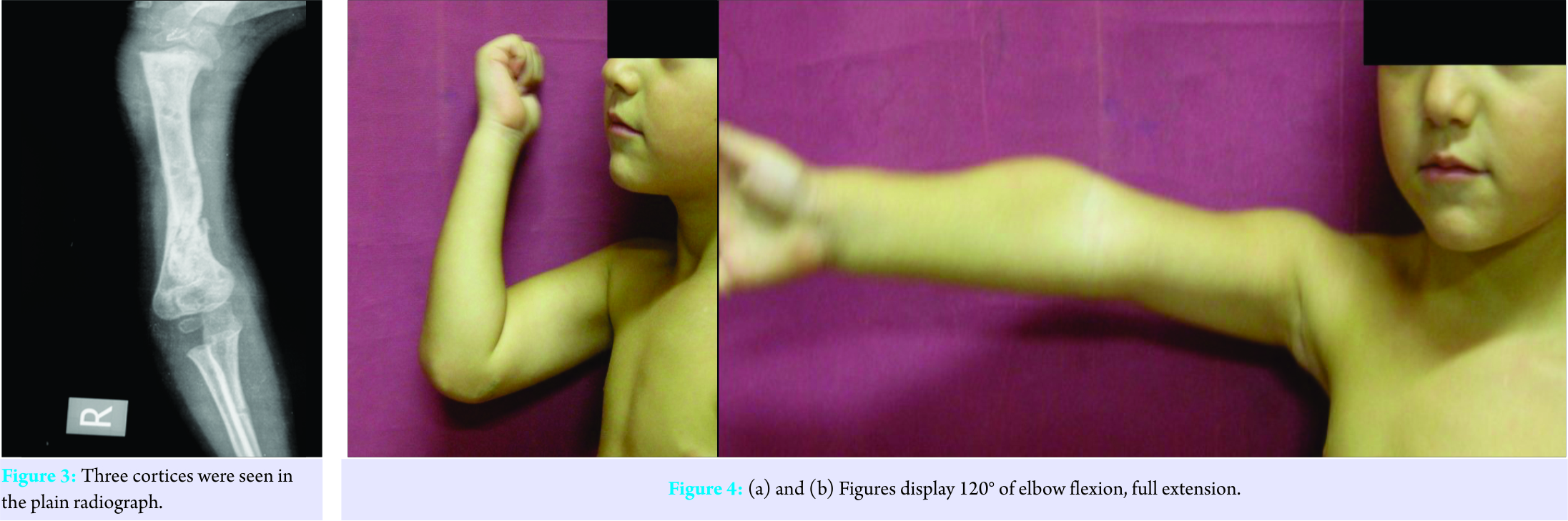
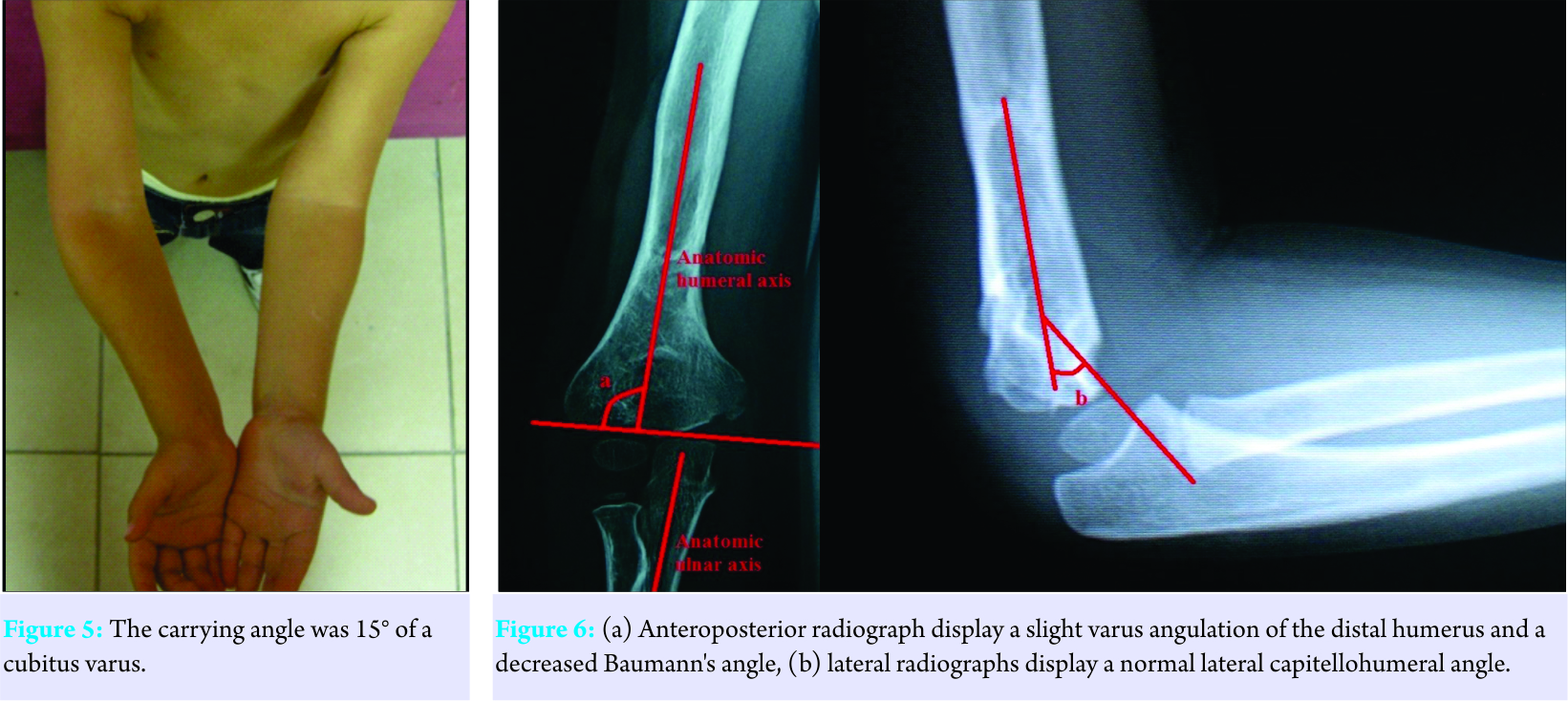
The patient was closely monitored in the inpatients unit in terms of vascular compromise and compartment syndrome. Gentamicin and metronidazole were stopped on the 3rd day of the follow-up period, and the patient was discharged. Intravenous cefazolin 500 mg 4 times daily was continued until the 7th post-operative day. A standard dressing was applied, and sutures were extracted 2 weeks after the operation. No sign of infection was noted during follow-up. To check healing of the bone defect, post-operative serial elbow radiographs were taken at the 1st, 2nd, 4th, and 6th week follow-ups. The external fixator was removed in the 6th week of follow-up after three cortices were seen in the plain radiograph (Fig. 3). Gentle elbow range of motion exercises were started as soon as the fixator was removed. With the exception of limited flexion of the elbow at the 12th month follow-up, supination and pronation were full. At 48th month follow-up, 120° of elbow flexion, full extension, and full forearm rotation were observed (Fig. 4a and b). A physical examination showed that carrying angle was 15° of a cubitus varus (Fig. 5); radiologic examination showed a slight varus angulation of the distal humerus, a decreased Baumann’s angle, and a normal lateral capitellohumeral angle, when compared with the healthy side (Fig. 6). In addition to the above findings, pain intensity, motion, stability, and function parameters of the elbow were assessed as being excellent with 100 points using the Mayo elbow performance score.
Discussion
As compared with adults, children have greater remodeling ability and healing potential, in addition to showing more resistance to joint stiffness. Periosteum continuity and the ligamentotaxis effect may provide rapid and quality bone development for the healing of the defective zone. To achieve new bone formation in a short period of time, use of external fixators in defective humeral fractures with periosteal continuity may be an effective surgical method in pediatric patients [3]. In line with these considerations, fast bone formation was observed 6 weeks after the operation in our patient through use of an external fixator. Likewise, in our opinion, the repair of the remaining periosteum played a crucial role in the formation of new bone. Stabilization is necessary in open fractures; however, rigid fixation is not always significant in younger children compared with older children and adults. Unless there is considerable bone loss, bone grafts are seldom necessary in young children because the periosteum has a clear ability to regenerate bone [4]. In our case, no bone graft was employed in defective area of the humerus; we relied on the high regeneration capacity of young age and the repair of the remaining periosteum. Regarding the treatment modalities of open pediatric fractures, a variety of fixation techniques have been described to date. For example, intramedullary fixation with rigid or elastic titanium nails, percutaneous Kirschner wires (K-wires) or plate and screw fixation techniques, external fixation with or without bone grafting may be employed taking into account the anatomic area and features of the fracture [4]. Besides these, treatment regimens of open forearm fractures mostly comprise cast immobilization only, intramedullary stabilization, percutaneous K-wire, or plate and screw fixation techniques [1, 5, 6]. As noted above, there are many techniques in the management of these fractures. However, the decision as to which technique is appropriate represents a challenge to surgeons treating pediatric open fractures [4]. External fixation has been employed as a traditional treatment method in open fractures of the femur, tibia, and pelvis in pediatric patients. The use of external fixators remains controversial, and numerous clinical studies have addressed the advantages and disadvantages of this technique [4, 7, 8, 9, 10, 11]. External fixation is an accepted treatment method for open unstable tibia fractures with severe comminution or considerable bone loss. However, complications such as high rates of pin-track infection, marked scars, soft tissue contracture, delayed union, refracture, and limb length inequality make external fixation less attractive in the management of stable tibia fractures [9, 11]. In additıon, external fixation is considered an option when flexible intramedullary nailing is not suitable due to fracture location, and characteristic or soft tissue conditions in open femoral fractures in children [8, 12]. When taking into account, the presence of considerable bone loss and soft tissue injury in addition to an increased risk of infection for the Type-III open fracture, we preferred to use joint and defect spanning multiplanar tubular external fixation in our patient. In the literature, a limited number of studies have been published to date regarding open supracondylar humerus fractures in pediatric populations. In a study by Haasbeek and Cole [1], 12 children who had a supracondylar humerus fracture were described; nine patients’ injuries were classified as Gustilo Type-I, two patients had Type-II fractures. All supracondylar humerus fractures were managed with closed reduction and percutaneous K-wire fixation. Union was achieved in all children, and there were no complications such as infection, non-union, delayed union, malunion, growth arrest, refracture, or neurovascular compromise. The final outcomes of the humeral fractures after at least a 3-year follow-up period, which covered carrying angle and range of motion of the elbow, showed excellent results in four patients, good results in seven patients, and fair results in two patients [1]. In another study, Pirone et al. [13] found only four patients with open supracondylar humerus fracture among 230 children with supracondylar fractures of the humerus. The definitive treatment of the four patients was open reduction and internal fixation (ORIF). However, the functional outcomes of ORIF in open fractures were not highlighted in this study [13]. In a recent study, Lewine et al. [2] compared open and closed supracondylar humerus fractures in 96 children, 30 with open fractures and 56 with closed fractures, all of which were Gartland Type-III. All patients were treated using open or closed reduction and pin fixation. With a slightly increased infection rate in the open fracture group, the clinical and radiographic outcomes of children were found similar in both groups considering post-operative loss of reduction, malunion, and neurovascular compromise [2]. However, no open supracondylar humerus fracture was treated using an external fixator. Furthermore, Slongo et al. defined a new technique called lateral external fixation for managing displaced supracondylar humerus fractures. The researchers used a small lateral external fixator in 31 pediatric patients; three patients had open supracondylar humerus fractures, one had a Gustilo Type-I, and two had a Gustilo Type-II fractures. In both closed and open supracondylar humerus fractures, normal range of motion was observed as well as excellent cosmetic results at the elbow. The authors stated that the main indications for this technique were irreducible fractures following use of the traditional closed techniques, oblique fractures that did not seem stabilized with classic methods, comminuted fractures, and open fractures of the humerus. According to this study, this technique may be considered as an alternative method to traditional percutaneous K-wire fixation, which provides to protect against secondary displacement and risk of malunion in cubitus varus [14]. It may be seen that external fixation is a useful treatment modality in the management of open supracondylar humerus fracture with bone loss. However, to the best of our knowledge, there are no case reports and a limited number of clinical studies in the literature addressing the management of open supracondylar humerus fractures [1, 2]. Furthermore, the existing studies are generally about either closed or open Gartland Type-III fractures without bone loss. We might make the argument that the present study provides additional evidence with respect to the treatment of open upper extremity fractures in the pediatric population because, to the best of our knowledge, this is the first case report regarding the use of a multiplanar external fixator, whether in a supracondylar humerus fracture or open fracture of the upper extremity with considerable bone loss. There are a variety of treatment methods with respect to the management of open fractures in pediatric population in the literature; however, research associated with the treatment of open fractures of the upper extremity, especially Gustilo-Anderson Type-III injuries, is quite limited. Accordingly, further studies addressing this challenging issue are required.
Conclusion
The use of external fixators in humeral fractures with bone loss may be an effective surgical method in pediatric patients because children have a greater remodeling ability and healing potential than adults in a short period of time due to periosteum continuity. As a result, multiplanar external fixation may be regarded as a definitive procedure in open supracondylar humerus fractures with considerable bone loss. However, physicians may confront some complications during the treatment period such as pin-track infection, marked scarring, soft tissue contracture, delayed union, and refracture.
Clinical Message
The multiplanar external fixation may be regarded as a definitive procedure in open supracondylar humerus fractures with considerable bone loss. However, it should be kept in the mind that several complications can be confronted by orthopedic surgeons.
References
1. Haasbeek JF, Cole WG. Open fractures of the arm in children. Bone Joint J 1995;77:576-81.
2. Lewine E, Kim JM, Miller PE, Waters PM, Mahan ST, Snyder B, et al. Closed versus open supracondylar fractures of the humerus in children: A Comparison of clinical and radiographic presentation and results. J Pediatr Orthop 2016.
3. Wiley JJ. Fracture patterns in children. In: Current Concepts of Bone Fragility. Berlin: Springer-Verlag; 1986. p. 159.
4. Stewart DG Jr, Kay RM, Skaggs DL. Open fractures in children. Principles of evaluation and management. J Bone Joint Surg Am 2005;87:2784-98.
5. Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE. Complications and outcomes of open pediatric forearm fractures. J Pediatr Orthop 2004;24:1-6.
6. Greenbaum B, Zionts LE, Ebramzadeh E. Open fractures of the forearm in children. J Orthop Trauma 2001;15:111-8.
7. Ramseier LE, Bhaskar AR, Cole WG, Howard AW. Treatment of open femur fractures in children: Comparison between external fixator and intramedullary nailing. J Pediatr Orthop 2007;27:748-50.
8. Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised study. J Bone Joint Surg Br 1997;79:975-8.
9. Kubiak EN, Egol KA, Scher D, Wasserman B, Feldman D, Koval KJ, et al. Operative treatment of tibial fractures in children: Are elastic stable intramedullary nails an improvement over external fixation? J Bone Joint Surg Am 2005;87:1761-8.
10. Cullen MC, Roy DR, Crawford AH. Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-47.
11. Tolo VT. External skeletal fixation in children’s fractures. J Pediatr Orthop 1983;3:435-42.
12. Hutchins CM, Sponseller PD, Sturm P, Mosquero R. Open femur fractures in children: Treatment, complications, and results. J Pediatr Orthop 2000;20:183-8.
13. Pirone AM, Graham HK, Krajbich JI. Management of displaced extension-type supracondylar fractures of the humerus in children. J Bone Joint Surg Am 1988;70:641-50.
14. Slongo T, Schmid T, Wilkins K, Joeris A. Lateral external fixation – A new surgical technique for displaced unreducible supracondylar humeral fractures in children. J Bone Joint Surg Am 2008;90:1690-7.
| How to Cite This Article: . Demirel M, Tunali O, Turkmen I, Saglam Y. As a Definitive Choice of Treatment, Joint and Defect Spanning Multiplanar Tubular External Fixation in the Management of Pediatric Open Defective Supracondylar Humerus Fracture: A Case Report. A Case Report. Journal of Orthopaedic Case Reports 2017 Sep-Oct;7(5):84-88. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


