
[box type=”bio”] Learning Point for this Article: [/box]
The treatment of traumatic bone loss is difficult and under certain circumstances, in a disadvantaged environment, it may be necessary to reintegrate a bone fragment expelled on the ground with very satisfactory results.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 30-32| Mamoudou Sawadogo, H Kafando, S Ouedraogo, S Tinto, M Tall. DOI: 10.13107/jocr.2250-0685.1036
Authors: Mamoudou Sawadogo[1], H Kafando[2], S Ouedraogo[1], S Tinto[2], M Tall[2]
[1]Department of Surgery, Regional University Hospital, Ouahigouya, Burkina Faso.
[2]Department of Orthopedics-Traumatology,Hospital Center University Yalgado Ouédraogo, Ouagadougou, Burkina Faso.
Address of Correspondence:
Dr. Mamoudou Sawadogo,
BP 36 CHR Ouahigouya, Burkina Faso.
E-mail: smamoudou@hotmail.com
Abstract
Introduction: Bone defect is a difficult problem in orthopedics. The treatment conventionally relies on techniques such as induced membrane, grafts, and elongations. The reintegration of an externalized osseous fragment involves significant infectious risks but is essential in certain situations.
Case Report: We report the case of a 10 cm traumatic bone loss of the right distal femur in a 35-year-old woman. Treatment consisted of paring, reintegration and stabilization by the external fixative. The 5-year follow-up was satisfactory with good consolidation and good function of the limb.
Conclusion: The reintegration of a bone fragment of limb expelled onto the soil is rare. We tried it because the response time was very short, but also and especially because the fragment was expelled on very hot bitumen. These two elements limited the risk of infection and favored the osseointegration of the fragment. We have not found a similar case reported in the literature allowing comparisons and recommendations.
Keywords: Traumatic, bone, loss, reconstruction.
Introduction
The reconstruction of diaphyseal bone segments remains a major challenge in the conservation of limbs regardless of the etiology of bone defect. This problem is still poorly solved by classical techniques, and amputation of the limb is still relevant.The most common methods are vascularized bone transfer (fibula), the segmental transfer method according to Ilizarov, and the sequential method of the induced membrane according to Masquelet. Bone autograft is not recommended when the loss of substance exceeds 4–5 cm. Beyond 6 cm, autologous bone grafts undergo a phenomenon of resorption even in a well vascularized muscular environment [1, 2]. We report a 10 cm traumatic bone loss of the right distal femur which we treated by trimming, reintegration, and stabilization by anexternal fixator.
Case Report
Mrs. M.S., aged 35, was in the back of a motorcycle driven by her husband when they were hit by a motor vehicle. She dropped on the tar with theopen trauma of the right thigh, expelling a bone fragment about 10 cm long on the pavement. The exact mechanism could not be specified. The patient was taken to the university hospital within 1h, with the expelled bone fragment packed in a plastic bag. On admission, the fragment was recovered and stored in physiological saline (Fig. 1). Clinical examination had a clear consciousness with Glasgow score = 15/15 and shock with blood pressure = 90/50 mm Hg and pulse rate = 110 pulses/min. The hemoglobin level was 8 g/dl. It was, therefore, a picture of polytrauma. The cutaneous opening, Type II of Gustilo-Anderson, was hemorrhagic and located at the anterolateral side of the thigh above the knee. The patient immediately received a transfusion of two globular pellets, tetanus prevention and 2 g of ceftriaxone. The radiograph of the femur had objectified a metaphyso-diaphyseal bone defect associated with an intercondylar split (Fig. 2).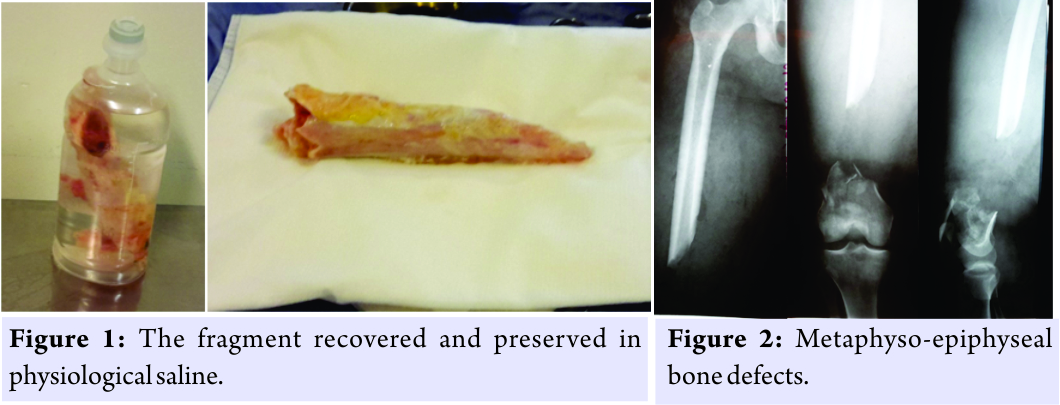 At about the 3rd h after her trauma, the patient was admitted to the operating room. The fragment was treated with physiological saline, then with 10 volumes hydrogen peroxide, and rinsed again with saline. After wound trimming, the fragment was reintegrated and reduced. The assembly was stabilized by an external Hoffmann II fixator (Fig. 3 and 4).
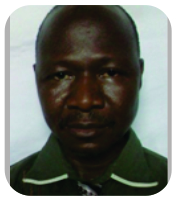
At about the 3rd h after her trauma, the patient was admitted to the operating room. The fragment was treated with physiological saline, then with 10 volumes hydrogen peroxide, and rinsed again with saline. After wound trimming, the fragment was reintegrated and reduced. The assembly was stabilized by an external Hoffmann II fixator (Fig. 3 and 4).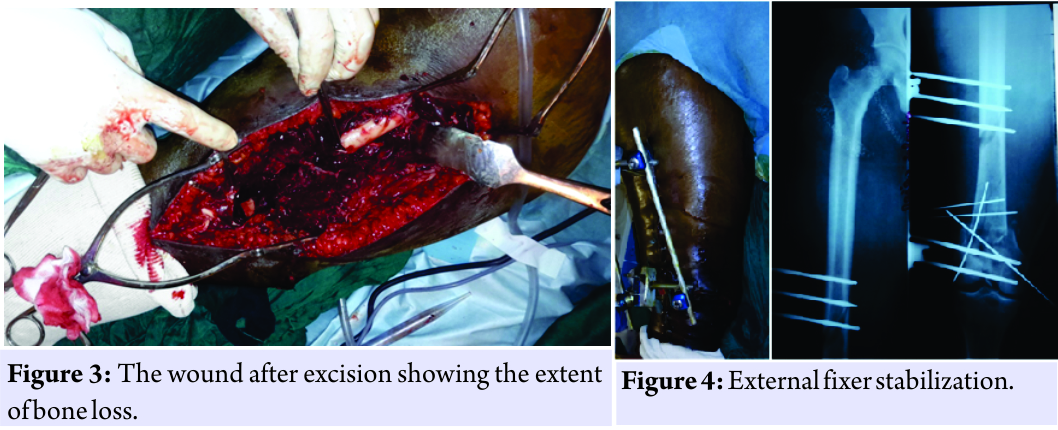 The surgical follow-ups were marked by superficial suppuration during the 2nd week. The pyoculture isolated a golden Staphylococcus, effectively treated with a triple combination of ceftriaxone, gentamycin, and metronidazole. Skin healing was obtained at the 3rd week. The physiotherapy was undertaken from the 4th week. Clinical and radiological consolidation was effective in the 7th, but the external fixation was only removed at the 9th post-operative month. At the 5-year follow-up, walking is normal, without limping. However, there are episodic and moderate mechanical gonalgia, a moderate stiffness of the knee with flexion limited to 100°. The result is considered satisfactory (Fig. 5 and 6).
The surgical follow-ups were marked by superficial suppuration during the 2nd week. The pyoculture isolated a golden Staphylococcus, effectively treated with a triple combination of ceftriaxone, gentamycin, and metronidazole. Skin healing was obtained at the 3rd week. The physiotherapy was undertaken from the 4th week. Clinical and radiological consolidation was effective in the 7th, but the external fixation was only removed at the 9th post-operative month. At the 5-year follow-up, walking is normal, without limping. However, there are episodic and moderate mechanical gonalgia, a moderate stiffness of the knee with flexion limited to 100°. The result is considered satisfactory (Fig. 5 and 6).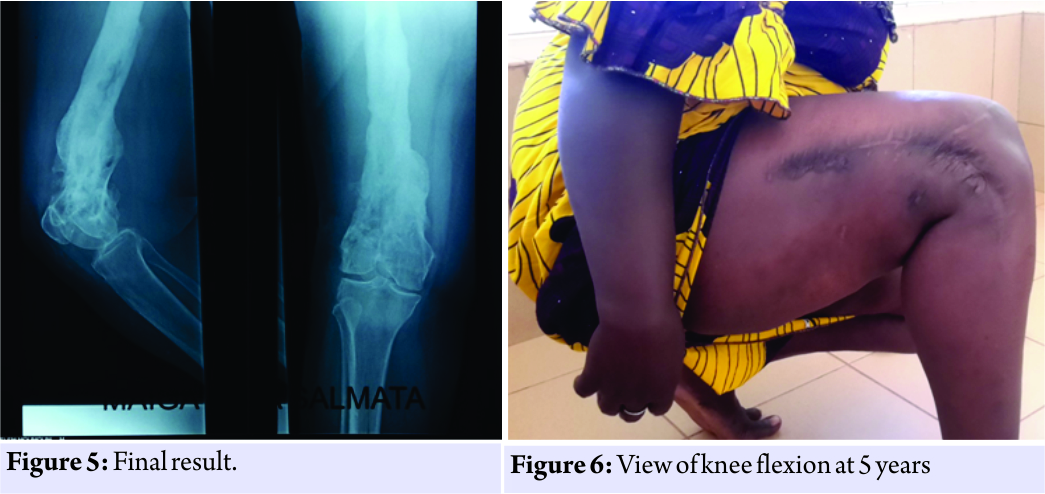
Discussion
The reconstruction of bone loss is one of the major difficulties encountered in reconstructive orthopedic surgery. Autologous bone grafting from the iliac crest remains the reference treatment [3]. However, the amount of autologous bone available may be insufficient,and the morbidity at the sampling site is not negligible. The reference techniques for large losses of substance are vascularized bone transfer [1, 4], bone mobilization according to the so-called “elevator” technique [5, 6, 7, 8, 9], and the induced membrane [1, 10]. These are techniques that require technical mastery, an adequate technical platform and which are sequential, requiring several re-interventions. Failures are not uncommon. Our observation took place in a semi-urban zone of a resource-limited country. The technical plateau is minimal,and care funding is provided directly by patients, who are often deprived. These facts limit the possibilities for reinterventions. Our attitude “reintegration of a bone fragment expelled on the road,” even if it appeared bold compared to the classic rules, could be justified by several considerations:
• Early intervention: we intervened within 3 hours of the trauma;
• The bone fragment was expelled onto the bitumen where the temperature was close to 50°.These two factors have undoubtedly contributed to limiting the infectious risk. The suppuration that we observed during the second post-operative week was probably related to the local conditions of asepsis and the opening of the focus when we know that open fractures are burdened in 10–30% of infectious complications [11].
• Moreover, the reintegration of the fragment that is similar to a bone autograft was done very early. The fragment was certainly still alive, which helped its rapid osseointegration. Most authors are convinced of the necessity of an early transplant, although paradoxically it is delayed [3]. At the 28th week the consolidation was acquired even if, as a precautionary measure, we delayed the removal of the fixer at 32 weeks. The delays reported in the literature are often much longer with conventional techniques [5, 6, 10, 9].
Conclusion
In all, it was a bold attitude that was beneficial, avoiding the patient multiple interventions in a precarious environment and with the result more than random. We have not found a similar case in the literature allowing comparisons or recommendations.
Clinical Message
Bone reconstruction can sometimes be a real challenge when substance loss is important, especially in disadvantaged areas. The reintegration of a lost bone fragment is not described in the literature but maybe a saving solution under certain conditions.
References
1. Masquelet AC, de Gauzy JS, Bauer T, Fabre A, Fitoussi F, Hannouche D, et al. Reconstruction of traumatic diaphyseal bone loss. Rev Chir Orthop Repar Appar Mot 2012;98:94-103.
2. Pallaro J, Angelliaume A, Dunet B, Lavoinne N, Tournier C, Fabre T. Reconstruction of femoral femoral bone loss by monoplane external fixation with bone transport. Rev Chir Orthop Repar Appar Mot 2015;101:379-84.
3. Garbuio P, Tropet Y. Type III leg open fractures with bone loss: Interest of bone grafting in contemporary urgency of internal fixation of skeleton and cover. Maîtrise Orthop 1999;87:6-8.
4. Tu YK, Yen CY, Yeh WL, Wang IC, Wang KC, Ueng WN, et al. Reconstruction of posttraumatic long bone defect with free vascularized bone graft: Good outcome in 48 patients with 6 years’ follow-up. Acta Orthop Scand 2001;72:359-64.
5. Rigal S, Merloz P, Le Nen D, Mathevon H, Masquelet AC. Bone mobilization technique in traumatic bone loss. Rev Chir Orthop Repar Appar Mot 2012;98:88-93.
6. Trigui M, Ayadi K, Ellouze Z, Gdoura F, Zribi M, Keskes H. Treatment of limb bone loss by segmental bone transport. Rev Chir Orthop Repar Appar Mot 2008;94:628-34.
7. Bégué T, Masquelet AC. Osteosynthesis of reconstructions after loss of segmental or cavitary bone substance. Comparative study of plates, external fixators and nailing. Rev Chir Orthop Repar Appar Mot 2011;97:S292.
8. Zappaterra T, Ghislandi X, Adam A, Huard S, Gindraux F, Gallinet D, et al. Reconstruction of bone loss of the upper limb by the induced membrane technique, prospective study of nine cases. Chir Main 2011;30:255-63.
9. Marais LC, Ferreira N. Bone transport through an induced membrane in the management of tibial bone defects resulting from chronic osteomyelitis. Strategies Trauma Limb Reconstr 2015;10:27-33.
10. Masquelet AC. The concept of membrane induced for the reconstruction of the losses of substance of long bones. E-Mem Acad Chir 2008;7:34-8.
11. Kitoko RA, W’Ifongo FW, Georis P, Gillet-Congo-Kinshasa P. Incidence of postoperative infections of osteosynthesis-treated fractures of the tibial leg and tibialis in the Democratic Republic of Congo. Med Afr Noire 2012;5912:573-81.
 |
 |
 |
 |
 |
| Dr. Mamoudou Sawadogo | Dr. Hamado Kafando | Dr. Ouedraogo Salam | Dr. Sayouba Tinto | Dr. Mohamed Tall |
| How to Cite This Article: Sawadogo M, Kafando H, Ouedraogo S, Tinto S, Tall M. Reconstruction of a Traumatic Bone Defect from Distal Femur. Journal of Orthopaedic Case Reports 2018. Mar- Apr; 8(2):30-32 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Comprehensive Arthroscopic Management of Multi-ligament Knee Injury: A Case Report
May 1, 2025 Comprehensive Arthroscopic Management of Multi-ligament Knee Injury: A Case Report March 1, 2025 Rehabilitation in Arthroscopic Anterior Cruciate Ligament Reconstruction
March 1, 2025 Rehabilitation in Arthroscopic Anterior Cruciate Ligament Reconstruction February 1, 2025 Novel Use of Tricortical Iliac Crest Bone Allograft to Reconstruct the Lateral Tibia Plateau Articular Surface: A Case Series
February 1, 2025 Novel Use of Tricortical Iliac Crest Bone Allograft to Reconstruct the Lateral Tibia Plateau Articular Surface: A Case Series February 1, 2025 Limb Salvage and Reconstruction of a Complex Upper Extremity Injury: A Case Report
February 1, 2025 Limb Salvage and Reconstruction of a Complex Upper Extremity Injury: A Case Report


