
[box type=”bio”] Learning Point of the Article: [/box]
Any mechanical stress, especially compression, applied on the extensor pollicis longus tendon can result in ischemia and rupture. We describe a unique mechanism of this condition.
Case Report | Volume 8 | Issue 5 | JOCR September – October 2018 | Page 89-91| Dimitrios Kitridis, Georgia Bei, Konstantinos Dogramatzis, Panagiotis Givissis. DOI: 10.13107/jocr.2250-0685.1228
Authors: Dimitrios Kitridis[1], Georgia Bei[2], Konstantinos Dogramatzis[3], Panagiotis Givissis[4]
[1]Department of Orthopaedics, 424 General Military Hospital, Thessaloniki, Greece,
[2]Department of Civil Engineering, Aristotle University of Thessaloniki, Thessaloniki, Greece,
[3]Department of Orthopaedics, 401 General Military Hospital, Athens, Greece,
[4]Department of Orthopaedics, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Address of Correspondence:
Dr. Dimitrios Kitridis,
Department of Orthopaedics, 424 General Military Hospital, Thessaloniki, Greece.
E-mail: dkitridis@gmail.com
Abstract
Introduction: Traumatic and atraumatic rupture of the extensor pollicis longus (EPL) tendon has been described as a result of mechanical or biological stresses. Common mechanisms include fractures of the distal radius, rheumatoid arthritis, local injection of steroids, and repetitive motion activities at the wrist.
Case Report: We report a case involving the spontaneous rupture of the EPL tendon in a relative of a deceased person who carried her coffin in a wrong way with no other predisposing factors. A three-dimensional simulation model was created in an attempt to illustrate the forces applied at his wrist.
Conclusion: Our case indicates that carriage of a coffin should be done by four undertakers, ideally of the same height, on their shoulders. Furthermore, a high level of suspicion is needed when tenderness over Lister’s tubercle after any type of trauma is encountered.
Keywords: Extensor pollicis longus, tendon rupture, spontaneous, tendon transfer.
Introduction
Spontaneous ruptures of the extensor pollicis longus (EPL) tendon have been reported most commonly after inflammatory conditions of the wrist, such as rheumatoid arthritis, or after undisplaced, or minimally displaced fractures of the distal radius [1, 2, 3, 4, 5]. Ruptures associated with sports activities or other daily repetitive movements have been also described [6, 7, 8, 9]. We report a rare case of non-traumatic spontaneous rupture of the EPL in a healthy male adult who was carrying his aunt’s coffin in a wrong way, with his palm, instead of the shoulder. A three-dimensional mathematical model was created in an effort to study the transmission of the forces to the four undertakers of the coffin.
Case Report
A 41-years-old right-handed man with height 1.82 m, presented in our outpatient clinic complaining for sudden loss of active extension of his right thumb. He experienced an extravagating pain and a popping sound at the dorsoradial aspect of his wrist. 4 days earlier, he was engaged as one of the four coffin carriers during the funeral of a relative. He was the second tallest of the carriers, and due to their different standing level, they could not carry the coffin on their shoulders, but it rested on their palms for over 200 m to normalize the different heights. As a result, our patient had to keep his wrist overloaded in full extension. He experienced pain in the dorsal aspect of his wrist from the first 50 m, but kept on until the end. Physical examination revealed tenderness over the third dorsal wrist compartment with the inability of his right thumb interphalangeal joint extension and weakness of the first metacarpophalangeal joint extension. Radiographs of the hand and wrist showed no bony abnormalities, and the clinical diagnosis of EPL tendon rupture was made.
Surgical exploration of the third dorsal wrist compartment verified EPL rupture at the level of Lister’s tubercle. The tendon was degenerated, brownish and a large necrotic area of almost 5 cm was apparent (Fig. 1). We hypothesized that the necrosis of the tendon happened due to the severe and continued crushing between the styloid process of the third metacarpal and the Lister’s tubercle. This led to a subsequent swelling and narrowing of the space of the third dorsal compartment, under the dorsal carpal ligament, thrombosis of the vessels, and long-acting ischemia of the tendon, which in combination with the crushing injury led to necrosis and rupture of the tendon. The large necrotic area of the tendon rendered direct repair not possible and tendon transfer using the extensor indicis proprius (EIP) was decided. The EIP tendon was transferred to the distal healthy stump of EPL using Pulvertaft suture technique (Fig. 2). Postoperatively, the patient’s hand was immobilized in a short-arm cast with the wrist in slight extension and the thumb in abduction and extension for 4 weeks. Then, the cast was exchanged for a shorter thermoplastic splint, which immobilized the wrist, fingers, and thumb in extension but was removed for intermittent exercise. This was applied for a further 2 weeks. In the meantime, an experienced hand therapist commenced a re-education program, stressing the synergistic movements of flexion and extension. 2 months postoperatively, he was able to fully extend and flex the interphalangeal joint of the thumb. At the 2 years follow-up, he remained asymptomatic (Fig. 3).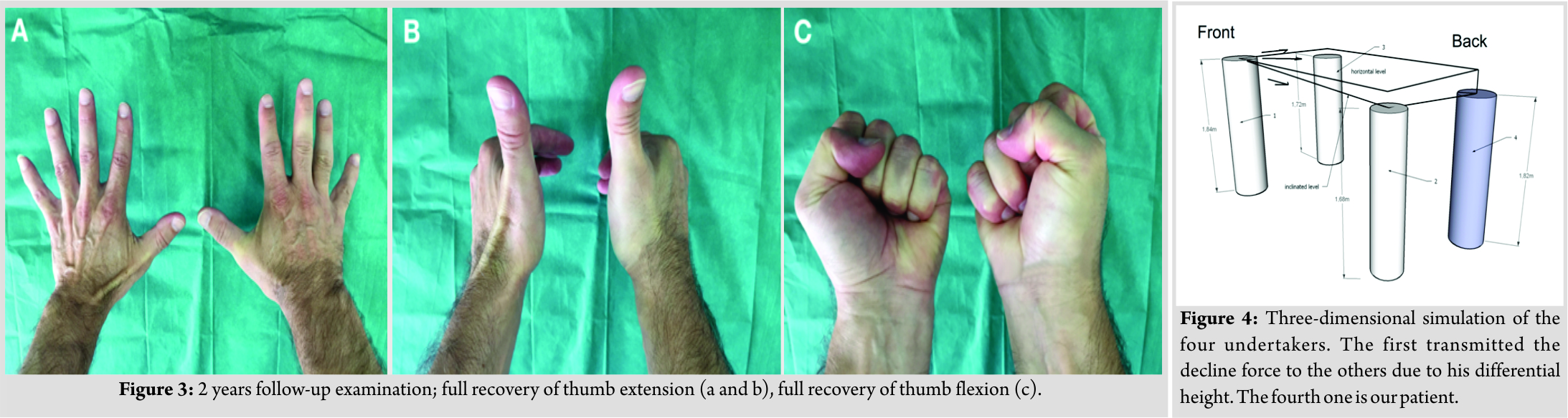
Discussion
Rheumatoid arthritis, steroid injections, gout, lupus, ischemic conditions, iatrogenic, and undisplaced or minimally displaced distal radial fractures have been known to cause spontaneous rupture of the EPL tendon [1, 2, 3, 4, 5]. Ruptures associated with sport or occupational activity, thus repeated abnormal movements of the wrist joint, without any other predisposing factor are limited [6, 7, 8, 9]. The pathogenesis of the spontaneous EPL tendon rupture seems to combine two major theories, a mechanical and a vascular one. According to the mechanical theory, the anatomical configuration of the EPL makes it vulnerable to disruption. Denman suggested that late EPL rupture after a Colles Fracture may be due to the crushing of the tendon between the styloid process of the third metacarpal and the dorsal tubercle of the radius, when the wrist is forced into extreme extension [10]. On the other hand, Björkman and Jörgsholm suggested that a rough bony edge after a distal radius fracture abrades the EPL tendon, which acts as a potential mechanical factor [1]. The vascular theory associates the increased pressure within the tendon sheath at Lister’s tubercle with ischemia and delayed rupture of the EPL tendon. Engkvist and Lundborg proved the peculiarity of EPL blood supply and its significance to delayed ruptures, usually within 8 weeks [11]. In a more recent microvascular study, Hirasawa et al. revealed that this tendon is subject to mechanical bending and attrition, has no mesotenon and has a poorly vascularized portion about 5 mm in length [12]. In our case, hyperextension and overloading of the wrist seem to have caused crushing of the tendon between the styloid process of the third metacarpal and the Lister’s tubercle. Subsequently, possible thrombosis of the vessels led to long-acting ischemia of the tendon and finally necrosis and rupture that was surprisingly 5 cm long. The large necrotic area of the tendon rendered direct repair not possible and tendon transfer using the EIP was used. The EIP has an appropriate direction and excursion, and the result was satisfactory. In an effort to understand the mechanism that led patient’s EPL to degeneration, necrosis, and finally to rupture we created a three-dimensional simulation model of the four undertakers (Fig. 4). Their numbers (1–4) and their heights are shown in (Fig. 4). Due to their different heights, the carriers could not carry the coffin on their shoulders as they should do. Instead, they have used their palms in a fully extended wrist to normalize the imbalance. The most possible scenario is that the two antidiagonal shorter undertakers (2 and 3) simply balance the load as horizontal fixed rollers while the tallest (1 and 4, also antidiagonal) receive all the stresses, as hinges. Transmission of a decline force from the tallest carrier (1) to our patient (4) means that he received the highest amount of strain. This strain is transmitted to the EPL tendon, which was trapped between Lister’s tubercle and the styloid process of the third metacarpal.
Conclusion
Our case indicates that carriage of a coffin should be done by four undertakers, ideally of the same height, on their shoulders. Otherwise, tendon problems could arise. We also believe that a high level of suspicion is needed when tenderness over Lister’s tubercle after any type of trauma is encountered. A synovial tendon sheath release to preserve the tendon’s vascularity may be considered.
Clinical Message
Any mechanical stress, especially compression, applied on the EPL tendon can result in ischemia and rupture. We describe a unique mechanism of this condition.
References
1. Björkman A, Jörgsholm P. Rupture of the extensor pollicis longus tendon: A study of aetiological factors. Scand J Plast Reconstr Surg Hand Surg 2004;38:32-5.
2. Roth KM, Blazar PE, Earp BE, Han R, Leung A. Incidence of extensor pollicis longus tendon rupture after nondisplaced distal radius fractures. J Hand Surg Am 2012;37:942-7.
3. Kim CH. Spontaneous rupture of the extensor pollicis longus tendon. Arch Plast Surg 2012;39:680-2.
4. Naito K, Sugiyama Y, Dilokhuttakarn T, Kinoshita M, Goto K, Aritomi K, et al. A survey of extensor pollicis longus tendon injury at the time of distal radius fractures. Injury 2017;48:925-9.
5. Sato K, Murakami K, Mimata Y, Doita M. Incidence of tendon rupture following volar plate fixation of distal radius fractures: A survey of 2787 cases. J Orthop 2018;15:236-8.
6. Choi JC, Kim WS, Na HY, Lee YS, Song WS, Kim DH, et al. Spontaneous rupture of the extensor pollicis longus tendon in a tailor. Clin Orthop Surg 2011;3:167-9.
7. Fujita N, Doita M, Yoshikawa M, Fujioka H, Sha N, Yoshiya S, et al. Spontaneous rupture of the extensor pollicis longus tendon in a professional skier. Knee Surg Sports Traumatol Arthrosc 2005;13:489-91.
8. Lloyd TW, Tyler MP, Roberts AH. Spontaneous rupture of extensor pollicis longus tendon in a kick boxer. Br J Sports Med 1998;32:178-9.
9. Taş S, Balta S, Benlier E. Spontaneous rupture of the extensor pollicis longus tendon due to unusual etiology. Balkan Med J 2014;31:105-6.
10. Denman EE. Rupture of the extensor pollicis longus–a crush injury. Hand 1979;11:295-8.
11. Engkvist O, Lundborg G. Rupture of the extensor pollicis longus tendon after fracture of the lower end of the radius – A clinical and microangiographic study. Hand 1979;11:76-86.
12. Hirasawa Y, Katsumi Y, Akiyoshi T, Tamai K, Tokioka T. Clinical and microangiographic studies on rupture of the E.P.L. tendon after distal radial fractures. J Hand Surg Br 1990;15:51-7.
 |
 |
 |
 |
| Dr. Dimitrios Kitridis | Dr. Georgia Bei | Dr. Georgia Bei | Dr. Panagiotis Givissis |
| How to Cite This Article: Kitridis D, Bei G, Dogramatzis K, Givissis P. Death of an Extensor Pollicis Longus due to a Funeral. Journal of Orthopaedic Case Reports 2018 Sep-Oct; 8(5): 89-91. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


