
[box type=”bio”] Learning Point of the Article: [/box]
For a chronic Monteggia fracture-dislocation, use the center of rotational angulation to determine the location of the ulnar osteotomy whether or not the fracture is intra-articular.
Case Report | Volume 8 | Issue 6 | JOCR November – December 2018 | Page 27-30 | Samuel L Posey, Heather A Cole, Schuyler Halverson, Chris Stutz, Jonathan G Schoenecker. DOI: 10.13107/jocr.2250-0685.1242
Authors: Samuel L Posey[1], Heather A Cole[1], Schuyler Halverson[1], Chris Stutz[2], Jonathan G Schoenecker[1]
[1]Department of Orthopaedics and Rehabilitation, Vanderbilt University Medical Center, Nashville, TN, USA.
[2]Divisions of Hand and Pediatric Orthopaedic Surgery, Texas Scottish Rite Hospital for Children, Dallas, TX, USA.
Address of Correspondence:
Dr. Jonathan G Schoenecker,
4202 Doctors’ Office Tower, 2200 Children’s Way, Nashville, TN 37232-9565, USA.
E-mail: jon.schoenecker@vumc.org
Abstract
Introduction: Elbow fractures are the most common pediatric fracture to require operative fixation and can be associated with significant morbidities such as vascular injury, neurologic injury, and loss of function. Specifically, the chronic Monteggia fracture-dislocation causes devastating losses in range of motion. Presenting as a proximal to midshaft ulna fracture and radiocapitellar joint disruption, the acute injury can be successfully managed with closed reduction, serial casting, and close follow-up. The chronic complications of this injury, however, usually occur from an unrecognized radial head dislocation. Here, we present the first known case of a chronic Monteggia fracture-dislocation in the setting of an intra-articular ulnar fracture. Using the center of rotational angulation (CORA) from injury mechanism and radiographs, an intra-articular osteotomy was performed to correct ulnar length and improve this child’s range of motion.
Case Report: A 3-year-old Hispanic male was first seen in the emergency department for elbow pain following a fall from a sofa. He was incorrectly diagnosed with an isolated intra-articular ulna fracture. 5 weeks after the initially missed Monteggia fracture-dislocation, he presented to clinic with 90° flexion, 40° extension, and a 20° pronation/supination arc. An opening-wedge osteotomy was performed at the intra-articular CORA to restore ulnar length and allow for reduction of the radial head. The magnitude of the ulnar opening-wedge osteotomy was trialed until the radiocapitellar joint maintained reduction throughout pronosupination.
Conclusion: 7 months after the surgery, the patient displayed functional improvements with 115° flexion, 15° extension, and a 75° pronation/supination arc. On physical examination, he had no neuropathic symptoms, with intact median, radial, and ulnar nerves. Using the CORA from the perceived injury mechanism and radiographs, an intra-articular osteotomy was performed to correct ulnar length, reduce the radial head, and thereby improve this child’s range of motion.
Keywords: Monteggia fracture, pediatrics, center of rotational angulation.
Introduction
Although awareness of the Monteggia fracture-dislocation presentation has increased among pediatric orthopedists [1, 2], this upper extremity injury still poses a diagnostic and subsequent therapeutic challenge to modern orthopedic surgeons. In 1943, Sir Watson-Jones stated “…no fracture presents so many problems; no injury is beset with greater difficulty; no treatment characterized by more general failure.”[3] The Monteggia fracture-dislocation pattern is classically described as a proximal third ulnar fracture and radial head dislocation. Normally, the longitudinal axis of the radius should bisect the ossification center of the capitellum in all radiologic views [4]. Focusing on the easily identified ulna fracture distracts a physician from the sometimes subtle radiocapitellar disruption in the under calcified elbow joint of a child. The ulna of such a missed presentation heals, but the dislocated radial head calcifies and can subsequently cause arthritis, pain, and loss of range of motion. Here, we present an unrecognized Monteggia fracture-dislocation in the setting of an intra-articular ulnar fracture; more significantly, we show how knowledge of the center of rotational angulation (CORA) permitted the success of an intra-articular osteotomy to restore ulnar length and improve a functional outcome.
Case Report
A 3-year-old male was seen in the emergency department with left elbow pain following a fall from a sofa. No prior injuries or significant medical history were noted. On physical examination, the skin was intact with soft and compressible compartments. The patient was neurovascularly intact with normal sensation and strength of the median, radial, and ulnar nerves and associated musculature. Plain radiographs at the time were read as a “minimally displaced olecranon fracture” (Fig. 1a and b). While the lateral view shows an intact radiocapitellar line, the AP view shows that the radius is medial to the capitellum. This radial head dislocation was not recognized at the time. The patient was placed in a bivalve long arm cast and scheduled to follow-up in clinic in 1 week; however, he missed the original follow-up appointment. 5 weeks after the initial injury, the patient followed up in clinic. By that time, the physical examination showed limited range of motion with arm flexion to 90°, extension to 40°, and a 20° pronation/supination arc. Repeat radiographs demonstrated an intra-articular olecranon fracture with a radial head dislocation and disruption of the proximal radioulnar joint (Fig. 1c and d). 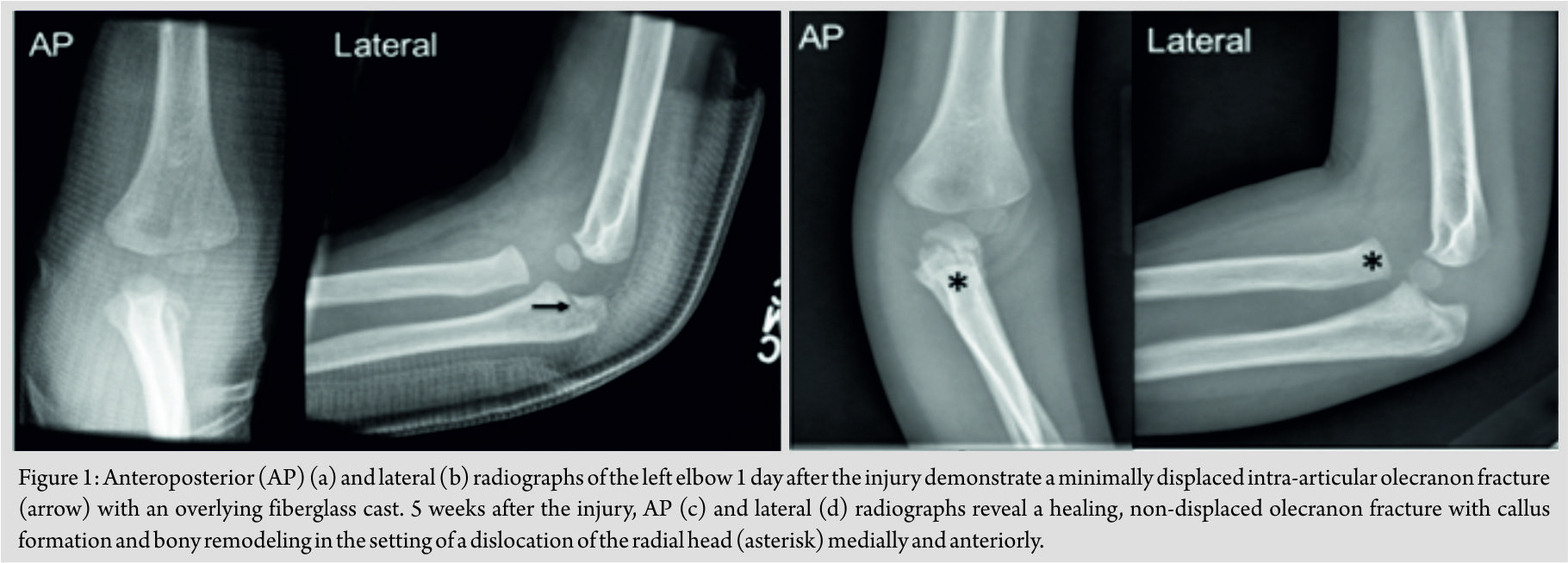 The original diagnosis did not identify the radial head dislocation. Due to the lack of follow-up, the patient remained incorrectly treated for 5 weeks in a long arm cast before recognizing the original radiographs as a Monteggia fracture-dislocation. Treatment of a chronic Monteggia fracture-dislocation with pain and functional disability requires operative fixation [5]. To correct the angular deformation of the malunited ulna, the CORA must be recognized as the intersection of the proximal and distal ulnar anatomical axes. Thereafter, an opening-wedge ulnar osteotomy is performed at the CORA to restore ulnar length and allow for reduction of the radial head [6]. The unique CORA of this injury mechanism was used to plan the intra-articular ulnar osteotomy as opposed to the classically described diaphyseal ulnar osteotomy (Fig. 2a, b, c, d, e, f, g, h).
The original diagnosis did not identify the radial head dislocation. Due to the lack of follow-up, the patient remained incorrectly treated for 5 weeks in a long arm cast before recognizing the original radiographs as a Monteggia fracture-dislocation. Treatment of a chronic Monteggia fracture-dislocation with pain and functional disability requires operative fixation [5]. To correct the angular deformation of the malunited ulna, the CORA must be recognized as the intersection of the proximal and distal ulnar anatomical axes. Thereafter, an opening-wedge ulnar osteotomy is performed at the CORA to restore ulnar length and allow for reduction of the radial head [6]. The unique CORA of this injury mechanism was used to plan the intra-articular ulnar osteotomy as opposed to the classically described diaphyseal ulnar osteotomy (Fig. 2a, b, c, d, e, f, g, h).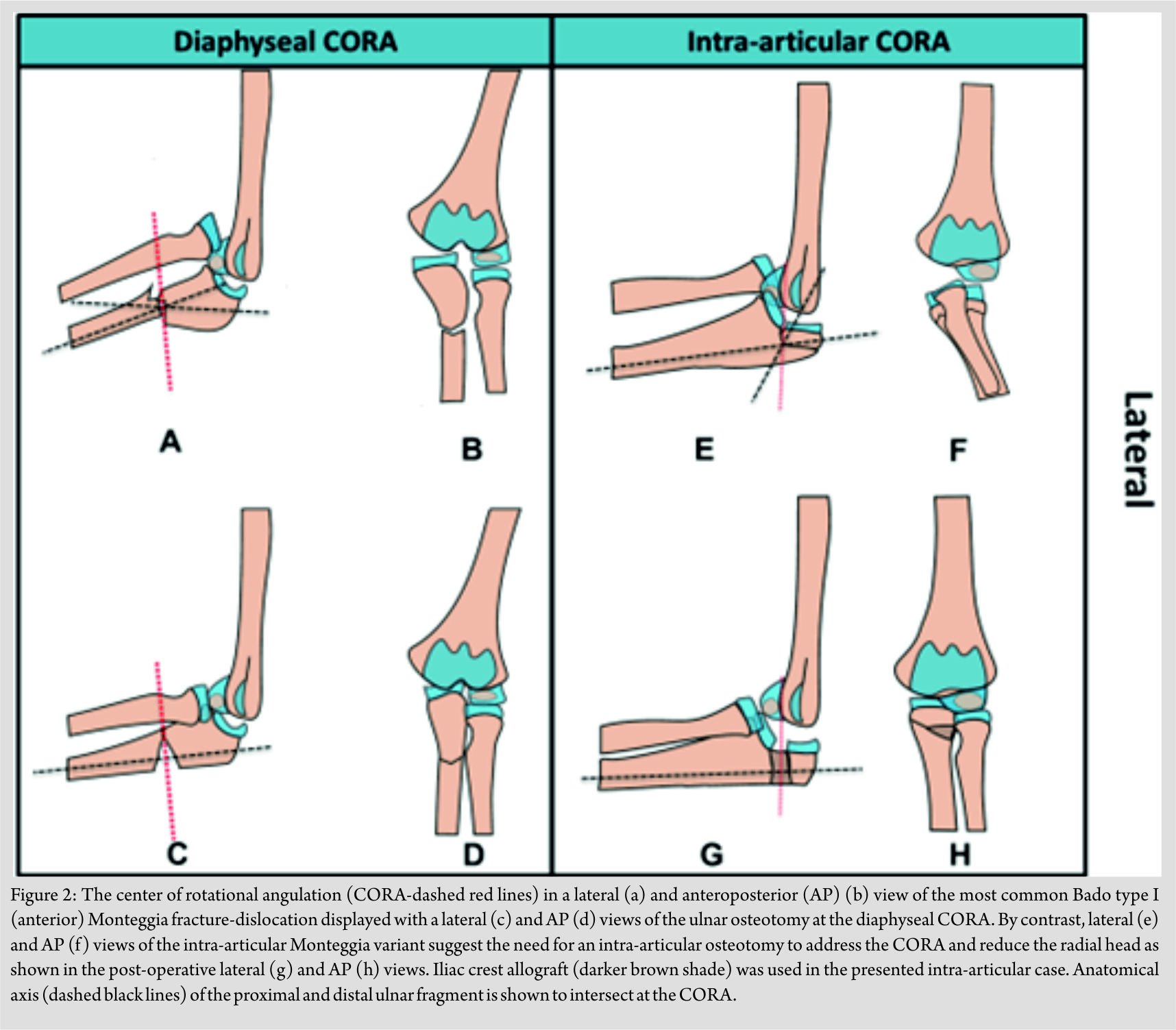 A posterolateral incision was made to allow visualization of the ulnar malunion and development of the Kocher interval (ECU-anconeus) to evaluate the radiocapitellar joint. A separate incision in the anterior antecubital fossa allowed identification and protection of the radial nerve in the brachialis-brachioradialis interval. To perform the ulnar osteotomy, K-wires were first used to localize and develop the plane of the malunion. The posterior corticotomy was performed with sequential drilling, and an osteotome was used to complete and distract the osteotomy (Fig. 3a, b, c, d, e).
A posterolateral incision was made to allow visualization of the ulnar malunion and development of the Kocher interval (ECU-anconeus) to evaluate the radiocapitellar joint. A separate incision in the anterior antecubital fossa allowed identification and protection of the radial nerve in the brachialis-brachioradialis interval. To perform the ulnar osteotomy, K-wires were first used to localize and develop the plane of the malunion. The posterior corticotomy was performed with sequential drilling, and an osteotome was used to complete and distract the osteotomy (Fig. 3a, b, c, d, e).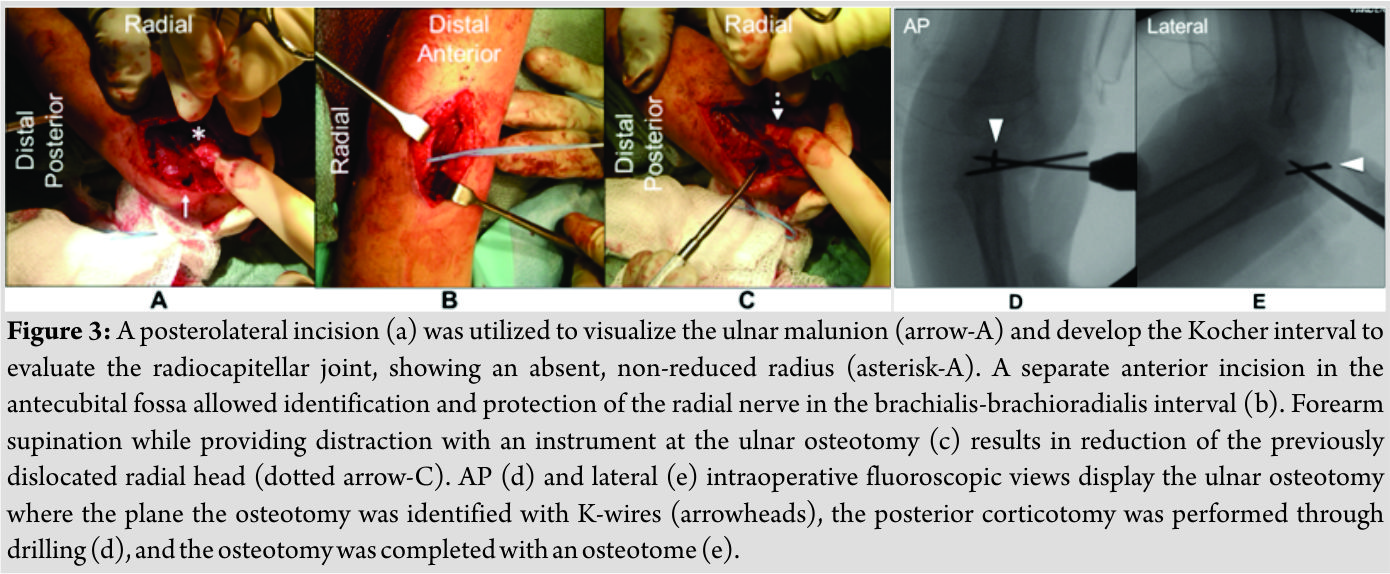 The magnitude of the ulnar opening-wedge osteotomy was trialed until the radiocapitellar joint maintained reduction throughout pronosupination. The radiocapitellar joint was pinned to hold reduction while the ulnar opening-wedge osteotomy was completed with tricortical iliac crest allograft. At the end of the case, the annular ligament was repaired (Fig. 4a, b, c, d, e, f).
The magnitude of the ulnar opening-wedge osteotomy was trialed until the radiocapitellar joint maintained reduction throughout pronosupination. The radiocapitellar joint was pinned to hold reduction while the ulnar opening-wedge osteotomy was completed with tricortical iliac crest allograft. At the end of the case, the annular ligament was repaired (Fig. 4a, b, c, d, e, f).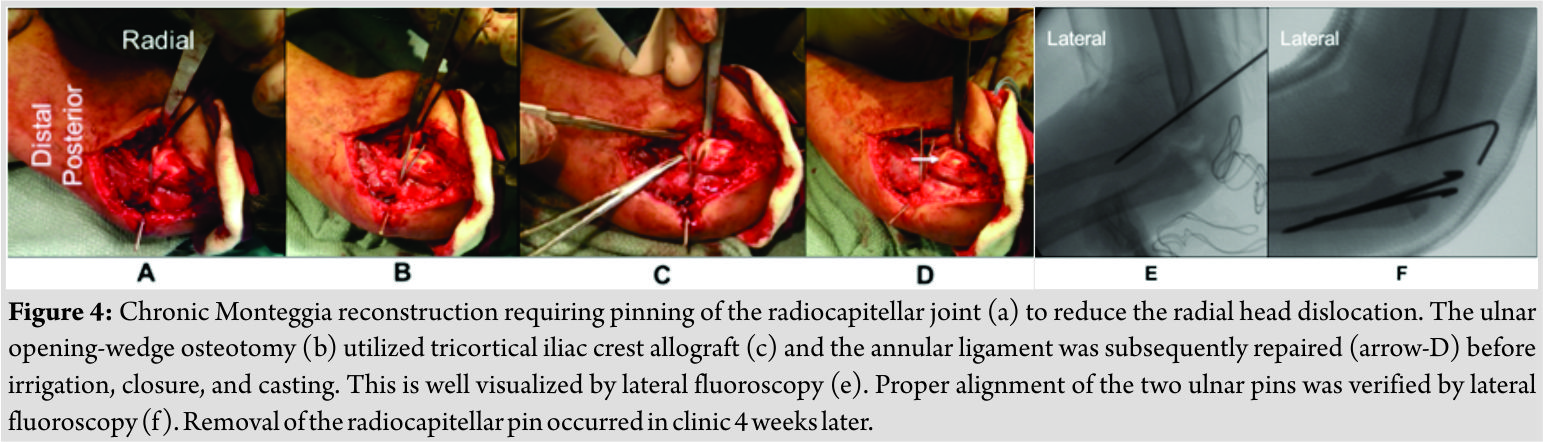 A subtle amount of instability remained in the joint after the osteotomy; therefore, the radiocapitellar pin was left in place and ultimately removed 4 weeks later in clinic. 7 months after surgery, the patient displayed functional improvements with arm flexion to 115°, extension to 15°, and a 75° pronation/supination arc (Fig. 5a, b, c). On physical examination, he had no neuropathic symptoms, with intact median, radial, and ulnar nerve function. Radiographs confirmed incorporation of the olecranon bone graft (Fig. 5d and e).
A subtle amount of instability remained in the joint after the osteotomy; therefore, the radiocapitellar pin was left in place and ultimately removed 4 weeks later in clinic. 7 months after surgery, the patient displayed functional improvements with arm flexion to 115°, extension to 15°, and a 75° pronation/supination arc (Fig. 5a, b, c). On physical examination, he had no neuropathic symptoms, with intact median, radial, and ulnar nerve function. Radiographs confirmed incorporation of the olecranon bone graft (Fig. 5d and e).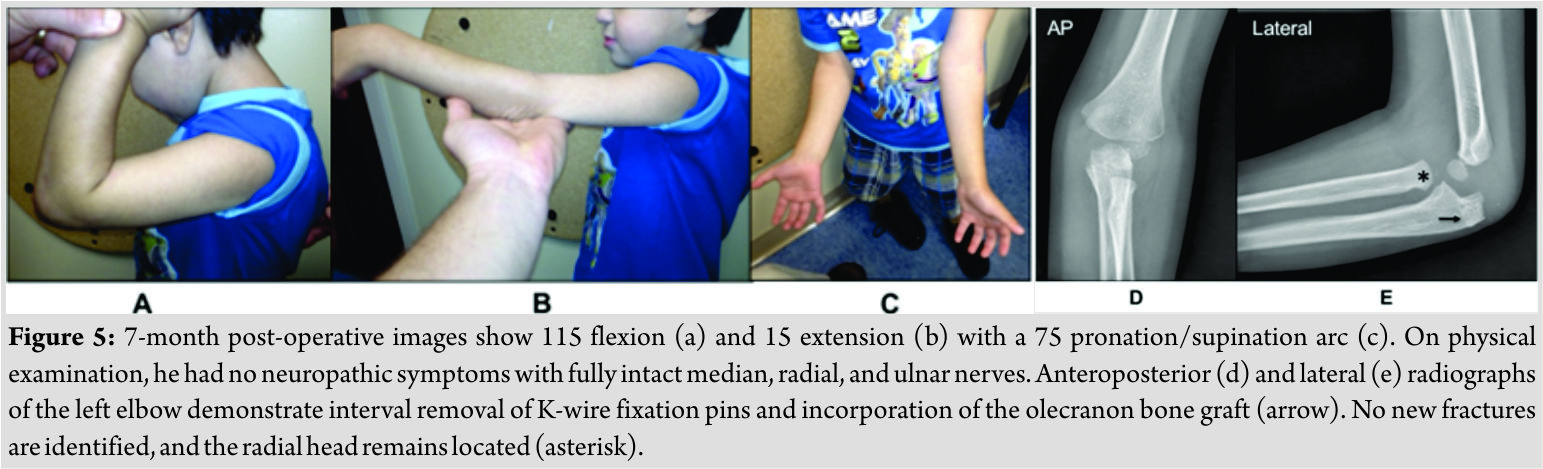 Most importantly, the radial head remained located and he regained most of his range of motion (Table 1).
Most importantly, the radial head remained located and he regained most of his range of motion (Table 1).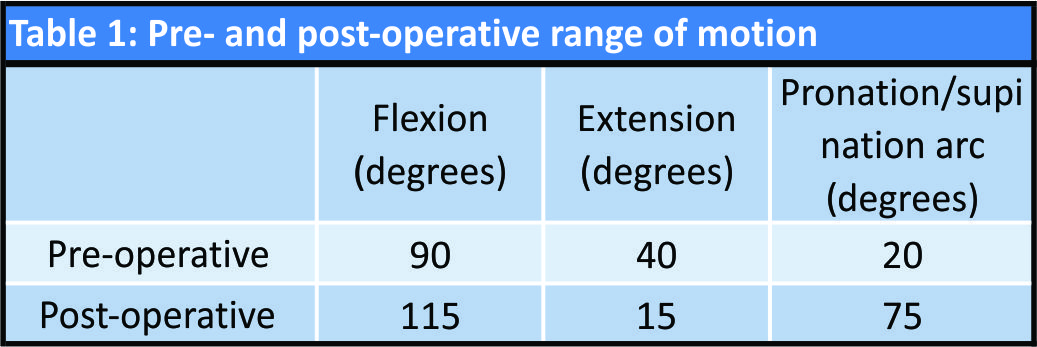
Discussion
Acute Monteggia fracture-dislocations can typically be treated by closed reduction and serial casting with close follow-up [2]. Although common in pediatrics, these are frequently missed injuries, thus they can present as a chronic injury requiring open reduction with an osteotomy to restore ulnar length and forearm rotation [7]. The missed Monteggia fracture-dislocation presented here not only emphasizes the need for clinical awareness of this injury mechanism, but also illustrates the novel use of an intra-articular osteotomy to correct anatomical alignment. To prevent the morbidity of loss of function and need for a more complex surgery, a physician’s suspicion for the Monteggia fracture-dislocation must heighten in the presence of an ulnar fracture; the subsequent transference of displacing forces through the stiff interosseous membrane toward the radial head necessitates a careful evaluation of elbow radiographs from multiple radiological views [8]. Simply, a pretzel cannot break in just one location, and an ulnar fracture in pediatrics requires careful evaluation of both the proximal and distal radioulnar joints in addition to other potential trajectories of the force vector. The mechanism of this injury is best explained by visualizing the CORA. In essence, the injury mechanism of most pediatric fractures displays an axis of rotation, which helps to explain the varus or valgus positioning of extremities and subsequent need for supination or pronation maneuvers to reduce such fractures [9]. While displacing forces can both fracture and cause a rotational malformation, the CORA is the point about which a deformity may be rotated to achieve correction. In the case of a proximal ulnar diaphysis fracture, the application of this knowledge correlates with the need for a diaphyseal ulnar osteotomy at the CORA to address the classically missed Monteggia fracture-dislocation [7]. The unique case presented here, however, suggested the use of an intra-articular ulnar osteotomy to address its CORA. In short, we propose that recognizing the location of the CORA aids in determining the location of the ulnar osteotomy. This study was limited by a loss in patient contact after the 7-month post-operative visit; nonetheless, a significant improvement in range of motion had been achieved at this point.
Conclusion
To the best of our knowledge, all reported pediatric cases of a chronic Monteggia fracture-dislocation injury involve an ulnar diaphyseal fracture and subsequent diaphyseal osteotomy to restore ulnar length and the longitudinal axis. By contrast, we present a unique intra-articular ulnar fracture variant of a missed Monteggia fracture-dislocation injury. More importantly, we use the CORA to explain the operative approach of an intra-articular osteotomy to improve the functional outcome.
Clinical Message
The Monteggia fracture-dislocation continues to beset the modern orthopedic surgeon, and this case study highlights the need for careful evaluation of the pediatric elbow from multiple radiologic views after an acute injury. If this injury pattern is missed and becomes a chronic malunion, however, we suggest using the CORA to determine the location of the ulnar osteotomy whether or not the fracture is intra-articular.
References
1. Saeed W, Waseem M. Fracture, Elbow. Stat Pearls; 2017. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28723005.
2. Leonidou A, Pagkalos J, Lepetsos P, Antonis K, Flieger I, Tsiridis E, et al. Pediatric monteggia fractures: A single-center study of the management of 40 patients. J Pediatr Orthop 2012;32:352-6.
3. Watson-Jones R. Fractures and Joint Injuries. 3th ed. Vol. 2 Baltimore, MD: Williams and Wilkins; 1943.
4. Peter MW, Bae DS. Pediatric Hand and Upper Limb Surgery: A Practical Guide. Lippincott: Williams and Wilkins; 2012.
5. Park H, Park KW, Park KB, Kim HW, Eom NK, Lee DH, et al. Impact of open reduction on surgical strategies for missed monteggia fracture in children. Yonsei Med J 2017;58:829-36.
6. Paley D, Herzenberg JE, Tetsworth K, McKie JB. Deformity Planning for Frontal and Sagittal Plane Corrective Osteotomies. Clinical Key. Available from: https://www.clinicalkey.com/#!/content/medline/2-s2.0-8028886. [Last accessed on 2017 Dec 22].
7. Goyal T, Arora SS, Banerjee S, Kandwal P. Neglected monteggia fracture dislocations in children: A systematic review. J Pediatr Orthop B 2015;24:191-9.
8. Anderson A, Werner FW, Tucci ER, Harley BJ. Role of the interosseous membrane and annular ligament in stabilizing the proximal radial head. J Shoulder Elbow Surg 2015;24:1926-33.
9. Fawdington R, Johnson B, Kiely N, Orthopaedics and Trauma. Vol. 28. UK: Elsevier Ltd; 2013. p. 33-40.
 |
 |
 |
 |
 |
| Dr. Samuel L Posey | Dr. Heather A Cole | Dr. Schuyler Halverson | Dr. Chris Stutz | Dr. Jonathan G Schoenecker |
| How to Cite This Article: Posey S L, Cole H A, Halverson S, Stutz C, Schoenecker J G. Intra-articular Monteggia Fracture: A Case Study of Using the Center of Rotational Angulation to Improve a Functional Outcome. Journal of Orthopaedic Case Reports 2018 Nov-Dec; 8(6): 27-30. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


