
[box type=”bio”] Learning Point of the Article: [/box]
Early diagnosis is the key to ensure a good functional outcome in the treatment of isolated Regan-Morrey type III ulnar coronoid process fracture.
Case Report | Volume 8 | Issue 6 | JOCR November – December 2018 | Page 65-67 | Ren Yi Kow, ZaharulAzri Mustapha Zakaria, Ed Simor Khan MorJapar Khan, ChooiLeng Low. DOI: 10.13107/jocr.2250-0685.1262
Authors: Ren Yi Kow[1],[3], ZaharulAzri Mustapha Zakaria[2], Ed Simor Khan MorJapar Khan[3], ChooiLeng Low[4]
[1]Department of Orthopaedic Surgery, Hospital Tengku Ampuan Afzan, Kuantan, Malaysia.
[2]Department of Orthopaedic Surgery, Hospital Kemaman, Terengganu, Malaysia.
[3]Department of Orthopaedic Surgery, International Islamic University Malaysia, Malaysia.
[4]Department of Radiology, Hospital Tengku Ampuan Afzan, Kuantan, Malaysia.
Address of Correspondence:
Dr. Kow Ren Yi,
Hospital Tengku Ampuan Afzan, 25100 Kuantan, Pahang, Malaysia.
E-mail: renyi_kow@hotmail.com
Abstract
Introduction: Fracture of the ulnar coronoid process is uncommon. It is commonly associated with posterior dislocation of the elbow, but it may also present as an isolated fracture. In general, all ulnar coronoid process fractures with elbow joint instability and large fracture fragments are fixed surgically. We report two cases of the rare isolated Regan-Morrey type III ulnar coronoid process fractures and their outcomes.
Case Report: Case Report 1: Mrs P, a 27-year-old right-hand dominant female, was involved in a motor vehicle accident (MVA) and sustained an isolated Regan-Morrey type III ulnar coronoid process fracture. In view of the large coronoid process fragment causing elbow joint instability, she underwent an open reduction and internal fixation when the elbow swelling had subsided. An anterior approach was used to identify the fracture fragment and it was fixed with two half-threaded cancellous lag screws with washers to achieve an anatomical reduction. Postoperatively, she recovered with excellent outcome based on the Mayo elbow performance score (MEPS).
Case Report 2: Mr M, a 23-year-old right-hand dominant gentleman, was involved in a MVA and sustained an isolated Regan-Morrey type III ulnar coronoid process fracture. During examination under general anesthesia, passive range of the movement of his right elbow was noted to be <90°due to the impaction of the fracture fragment. An open reduction through an anterior approach was performed and Kirschner wires were inserted to fix the coronoid process fracture. Kirschner wires were opted for the ease of post-operative removal as the patient was not keen to have a retained implant after recovery. He recovered with good outcome based on the MEPS.
Conclusion: Isolated fracture of the ulnar coronoid process is rare. Open reduction and internal fixation is mandatory for patients with coronoid process fracture and unstable elbow joint to achieve good functional outcomes.
Keywords: Coronoid fracture, ulna, Regan-Morrey, surgery, fracture.
Introduction
Fracture of the ulnar coronoid process is rare [1]. It is commonly associated with posterior dislocation of the elbow, but it may also present with isolated fracture of the ulnar coronoid process [1]. Up to 15% of the patients with posterior dislocation of the elbow have concurrent fractures of the ulnar coronoid process [2]. The stability of the elbow joint is maintained by a combination of the bony component, integrity of ligaments, capsule, and muscles surrounding it [1]. Anatomical studies reveal that ulnohumeral articulation is the primary constraint of the elbow joint [1]. The elbow joint is further stabilized by the medial and lateral collateral ligaments, ulnohumeral capsule, and the brachialis muscle [1]. Besides acting as an insertion point for the medial collateral ligament, the ulnar coronoid process, together with the radial head, also functions as an anterior buttress to prevent posterior subluxation and dislocation [1]. Cadaveric studies also show that a loss of 50% or more of the height of the ulnar coronoid process destabilizes the elbow joint posteriorly [1]. There are two classification systems for ulnar coronoid process fracture, namely the Regan and Morrey classification system and the O’Driscoll classification system [2]. In 1989, Regan and Morrey classified ulnar coronoid process fractures into three types based on the height of the coronoid process involved on lateral plain radiograph [2]. Type I fractures involve the tip of the coronoid process, type II fractures involve <50% of the height of the coronoid process, and type III fractures involve more than 50% of the height of the coronoid process [2]. In 2003, O’Driscoll divided ulnar coronoid process fractures based on the anatomical location and the number of coronoid process fragments, with a focus on identifying anteromedial fractures [2]. At present, there is no consensus on the mode of treatment for isolated ulnar coronoid process fracture, but generally, all ulnar coronoid process fractures with elbow joint instability and large fracture fragments are fixed surgically. We report two cases of the rare isolated Regan-Morrey type III ulnar coronoid process fractures and their outcomes.
Case Report
Case Report 1
Mrs P, a 27-year-old right-hand dominant female, was involved in a motorvehicle accident (MVA) while riding a motorcycle. She had a fall and landed on her right side with an outstretched right hand. Post-trauma, she complained of pain and swelling at her right elbow with limited the right elbow range of movement due to the pain and swelling. She had no other associated injuries. Plain radiographs of her right elbow showed an isolated Regan-Morrey type III ulnar coronoid process fracture (Fig. 1a). In view of the large coronoid process fragment causing elbow joint instability, she underwent an open reduction and internal fixation when the elbow swelling had subsided. An anterior approach as described by Han et al. was used to identify the fracture fragment [3]. Under tourniquet control, a “lazy S” skin incision was made 2cm proximal to the elbow flexion crease, 1cm lateral to the biceps, and curves across the flexor crease horizontally and distally toward the ulnar border of the forearm, approximately 2cm distal to the flexor crease. The lateral antebrachial cutaneous nerve was identified and retracted laterally away from the surgical field. On incision of the bicipital aponeurosis, the median nerve and brachial artery were identified and retracted medially. The brachialis muscle was then incised and retracted to expose the coronoid fracture fragment. The fracture was fixed with two half-threaded cancellous lag screws with washers (3.5 mm and 2.7 mm, respectively) to achieve an anatomical reduction (Fig. 1b). 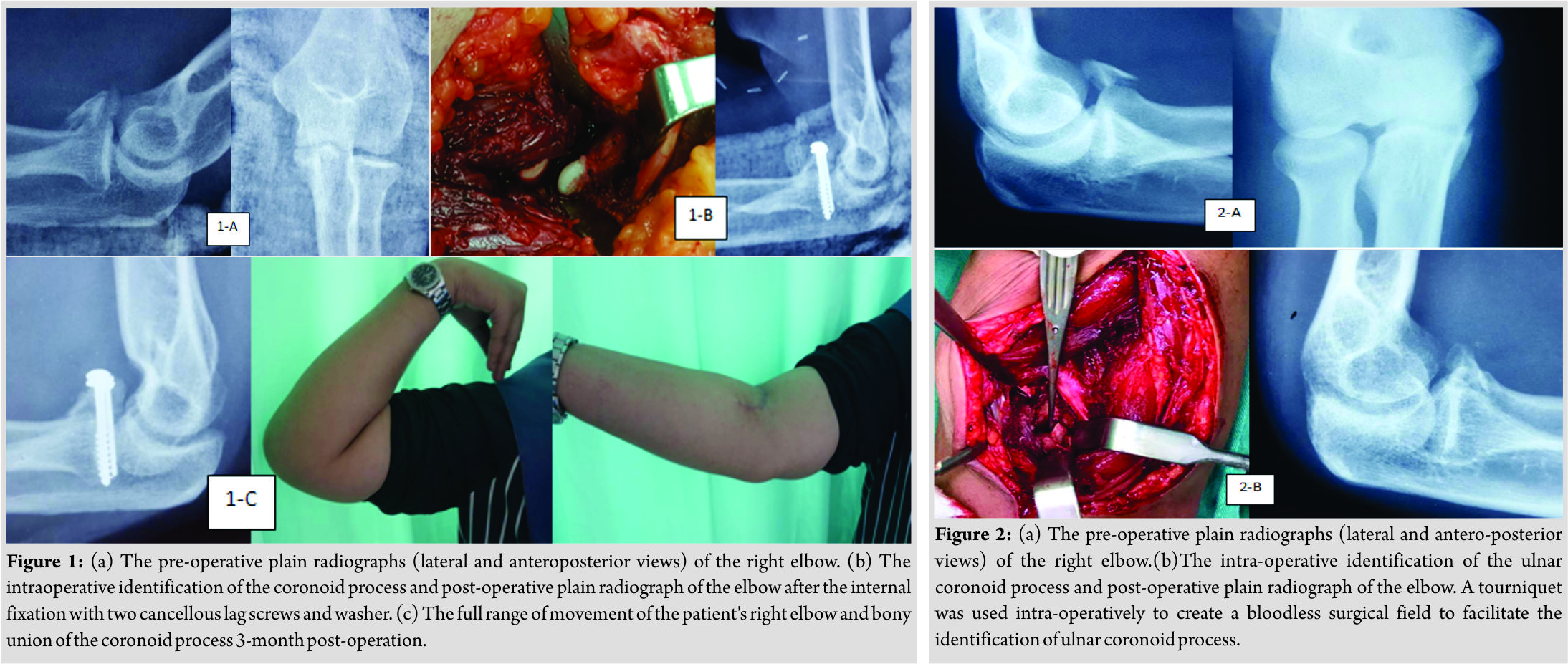 Postoperatively, her right elbow was protected with an above elbow posterior slab for 2 weeks, and then, she was started on gradual active range of movement exercises without any complication. Bony union was achieved at 3-month post-operation with excellent outcome based on the Mayo elbow performance score (MEPS).
Postoperatively, her right elbow was protected with an above elbow posterior slab for 2 weeks, and then, she was started on gradual active range of movement exercises without any complication. Bony union was achieved at 3-month post-operation with excellent outcome based on the Mayo elbow performance score (MEPS).
Case Report 2
Mr M, a 23-year-old right-hand dominant gentleman, was involved in an MVA in which he fell and landed on his right side with his outstretched right hand. He had limited range of motion of his right elbow due to the severe pain and swelling. Plain radiographs of his right elbow showed an isolated Regan-Morrey type III ulnar coronoid process fracture (Fig. 2a). When the soft tissue swelling had reduced, he underwent an examination of his right elbow under general anesthesia. Intraoperatively, the passive range of movement of the right elbow was <90° due to the impaction of the fracture fragment. An open reduction through an anterior approach was performed and Kirschner wires were inserted to fix the coronoid process fracture (Fig. 2b). Kirschner wires were opted for the ease of post-operative removal as the patient was not keen to have a retained implant after recovery. Postoperatively, the Kirschner wires were removed after 3 weeks and his right elbow was protected with an above elbow posterior slab for 6 weeks before he started on gradual active range of movement exercises without any complication. Bony union was achieved postoperatively with good outcome based on the MEPS (Table 1).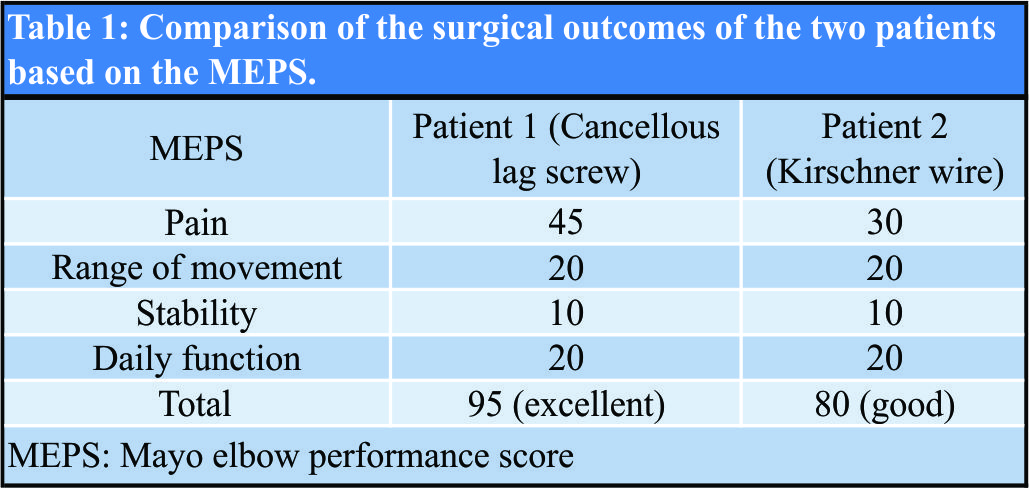
Discussion
Isolated fracture of the coronoid process of the ulna is rare. In 1989, Regan and Morrey reported five cases of type III ulnar coronoid process fractures, in which only one case is an isolated type [4]. Treatment of the coronoid process fracture includes both conservative and surgical fixation. Butler et al. reported a good outcome in an isolated anterolateral fracture of the coronoid process of the ulna without ligamentous injury which was treated conservatively [5]. The indications for surgical fixation include type III fractures, unstable elbow joint, or any terrible triad pattern injury [1]. In the term of surgical fixation, most authors agree that an open reduction through an anterior approach is the best method [1, 2, 3, 4]. This approach provides an excellent exposure for fracture fragment identification in cases of isolated coronoid process fractures [3]. Nevertheless, care should be taken to avoid injury to the lateral antebrachial cutaneous nerve after skin incision as well as the brachial artery and median nerve after incision of the bicipitalaponeurosis [3]. On identification of the coronoid process, it can be fixed with a variety of implants. Cancellous lag screw, miniplate, Kirchner wire, and suture can be used to fix the fracture with good outcomes [1, 2,5]. After fixing the coronoid process, it is imperative to examine the elbow joint stability. In cases where there is elbow joint instability, the medial and lateral collateral ligaments and the capsule have to be repaired to achieve a stable elbow joint. Postoperatively, the affected elbow needs to be protected for 2–3 weeks. After that, gradual active range of movement exercises can be started. Nonsteroidal anti-inflammatory drugs such as indomethacin can be given to reduce the incidence of post-traumatic heterotopic ossification of the elbow.
Conclusion
Isolated fracture of the ulnar coronoid process is rare. Open reduction and internal fixation is mandatory for patients with coronoid process fracture and unstable elbow joint to achieve good functional outcomes.
Clinical Message
A high index of suspicion is needed to diagnose isolated coronoid fracture. A neglected isolated coronoid fracture may lead to poor functional outcome of the elbow. If indicated, open reduction and internal fixation is mandatory as soon as the soft tissue condition is favorable.
References
1. Samii A, Zellweger R. Fractures of the coronoid process of the ulna: Which ones to fix and which ones to leave alone: A review. Eur J Trauma EmergSurg 2008;34:113-9.
2. Lee SK, Kim HY, Kim KJ, Yang DS, Choy WS. Coronoid plate fixation of Type II and III coronoid process fractures: Outcome and prognostic factors. Eur J OrthopSurgTraumatol 2012;22:213-9.
3. Han SH, Yoon HK, Rhee SY, Lee JK. Anterior approach for fixation of isolated Type III coronoid process fracture. Eur J OrthopSurgTraumatol 2013;23:395-405.
4. Hanks GA, Kottmeier SA. Isolated fracture of the coronoid process of the ulna: A case report and review of the literature. J Orthop Trauma 1990;4:193-6.
5. Butler DP, Alsousou J, Keys R. Isolated anterolateral fracture of the coronoid process of the ulna: A case report. J Shoulder Elbow Surg 2011;20:e1-4.
 |
 |
 |
 |
| Dr. Ren Yi Kow | Dr. Zaharul Azri M Z | Dr. Zaharul Azri M Z | Dr. Ed Simor Khan MorJapar Khan |
| How to Cite This Article: Kow R Y, Zaharul Azri M Z, Mor Japar Khan E S K, Low C L. Isolated Regan-Morrey Type III Fracture of the Ulnar Coronoid Process: A Report of Two Cases. Journal of Orthopaedic Case Reports 2018 Nov-Dec; 8(6): 65-67. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


