
[box type=”bio”] Learning Point of the Article: [/box]
Combining a correction approach, based on the Ponseti regimen with a hexapod fixator, together with a triple arthrodesis has presented an excellent management strategy for neglected clubfeet in an adult.
Case Report | Volume 9 | Issue 1 | JOCR January – February 2019 | Page 85-89 | Ziyaad Mayet, Annette-Christi Barnard, Franz Birkholtz. DOI: 10.13107/jocr.2250-0685.1322
Authors: Ziyaad Mayet[1],[2], Annette-Christi Barnard[3], Franz Birkholtz[3],[4]
[1]Department of Orthopaedics, Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa,
[2]Department of Orthopaedics, University of the Witwatersrand, Johannesburg, South Africa,
[3]Department of Orthopaedics, Walk-A-Mile Centre for Advanced Orthopaedics, Centurion 0046, Pretoria, South Africa,
[4]Department of Orthopaedics, University of Pretoria, Pretoria 0002, South Africa.
Address of Correspondence:
Dr. Franz Birkholtz,
Department of Orthopaedics, University of Pretoria, Pretoria 0002, South Africa.
E-mail: franz.birkholtz@walkamile.co.za
Abstract
Introduction: Management of neglected clubfoot presents a challenging problem. Treatments traditionally involve extensive posteromedial soft tissue releases, bony procedures, and the Ilizarov technique of differential distraction.
Case Report: We present a case of bilateral neglected clubfoot in a 34-year-old female. Management involved the novel combination of the gradual distraction of prepared triple arthrodesis surfaces and the Ponseti regimen which was achieved using the three-dimensional corrective power of hexapod-type circular fixators. Both feet were corrected to achieve plantigrade painless feet.
Conclusion: Combining the Ponseti regimen with a hexapod fixator has presented an excellent management strategy for neglected clubfeet in an adult. We further propose the use of a generic name, the Ponseti-hex technique, to cover for the use of all makes of hexapod external fixators.
Keywords: Adult neglected clubfoot, Ponseti regimen, Hexapod circular fixators, Ponseti-hex technique.
Introduction
Clubfoot has traditionally been a difficult condition to treat. Numerous operative and non-operative techniques have been used over the years [1]. The Ponseti regimen has arguably revolutionized the treatment of clubfoot and can be described as the gold standard [2]. It is based on serial manipulations and casting and aims to reverse the deformity using an understanding of the kinematics of the ankle and subtalar joints. The results of treatment in infancy with the Ponseti regimen have shown good results [2,3]. The Ponsetaylor technique is an alternative in successfully managing neglected or recurrent clubfeet. This technique utilizes a hexapod external fixator, specifically the Taylor Spatial Frame (Smith and Nephew, Memphis, USA) to achieve correctionby Ponseti’s principles [4]. Residual, recurrent, and neglected clubfoot is usually more challenging to treat. They present with rigid deformities, contracted posteromedial soft tissue structures, and tarsal bones with altered shapes from growth in deformed or abnormal positions, making treatment unpredictable [3]. Management ranges from conservative management to amputation, with treatments traditionally involving extensive posteromedial soft tissue releases, bony procedures, and the use of the Ilizarov technique with differential distraction [3,5, 6, 7, 8, 9, 10]. The use of the Ponsetaylor technique provides an attractive management option in the adult patient. We present a case of a 34-year-old female with neglected clubfoot where the combination of triple arthrodesis, distraction osteogenesis, and the three-dimensional corrective power of hexapod type circular fixators were used to achieve correction in both feet. The left foot was done with a Taylor Spatial Frame and the right was done with a TrueLok-Hex (Orthofix, Verona, Italy). We,therefore, also proposethe use of a generic name, the Ponseti-Hex technique, to cover for the use of all makes of hexapod external fixators.
Case Report
A 34-year-old female presented with bilateral neglected clubfoot. She presented with pain and callosities on the lateral border of the feet and was unable to fit the left foot into regular shoes (Fig. 1). All toes had flexion and adduction deformities at the metatarsophalangeal joint level,and the toe deformities were not fixed. The rigid equinocavovarus deformity on the left was visibly worse with fore foot adduction and pronation (Fig. 2),resulting in weight bearing only on the dorsolateral surface of the foot. Of note was the presence of a flat-top talus on the leftfoot (Fig. 3), indicative of abnormal growth of the talus. The presence of the flat-top talus resulted in restricted movement of the ankle and an equinus deformity that could only be fully corrected with an osteotomy. The severity of the left foot deformity and rigidity resulted in pre-operative AOFAS scores of8 for the hindfoot and 0 for the midfoot. The left foot was operated on first,followed by the right. The Ponsetaylor technique was used to correct the left foot using a Taylor Spatial Frame (Fig. 4). 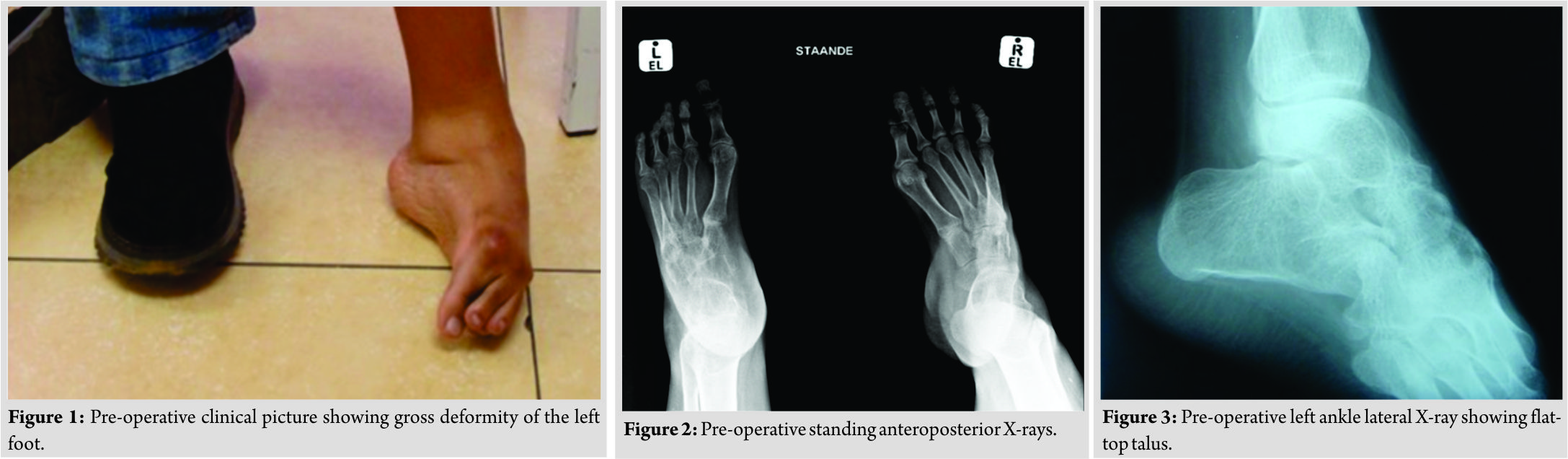 The right foot was treated in a similar fashion using a TrueLok-Hex Frame(Orthofix Verona, Italy) (Fig. 4). The procedures were combined with triple arthrodesis,and reduction and union were achieved using distraction osteogenesis. Both feet followed the same sequence. A plantar fascia release was performed to get some correction of the cavus to facilitate fixation in the frame.The Hoke procedure was performed to lengthen the Achilles tendon with percutaneous step cuts, allowing for its excursion during the correction process. The subtalar and calcaneocuboid joints were prepared for arthrodesis through a lateral approach. The medial approach was used for the talonavicular joint. The external fixator was applied with a full ring on the tibia and the foot. A laterally placed olive wire was placed in the talus to act as a fulcrum for correction. This was initially attached to the tibial frame, allowing correction to occur primarily through the subtalar joint. After a lag period of 7 days, gradual correction was started. Programming for the correction involved correction of the varus and internal rotation. After correction of these components, the talar wire was attached to the foot ring and equinus was corrected through the ankle joint by running a second adjustment programme. The frame was left in situ until consolidation of the arthrodesis had taken place. Intramedullary K-wires were inserted into the toes and kept throughout the duration of the correction to protect the metatarsophalangeal joints and prevent clawing of the toes. Time in frame for the left foot was 4 months and 4.1 months for the right. The arthrodesis was united at the time of frame removal for both feet,and no further casts or orthotics were needed.Pin track complications were minimal,and no antibiotics or exchanges were needed. The only complication was a posterior talar subluxation on the right during the equinus correction phase, which was corrected with a residual program. The patient was followed up 12 months after the Ponseti-Hex procedures and reported no chronic pain. Both feet were corrected to achieve plantigrade painless feet. On the right, a residual equinus deformity of 20° remained(Fig. 5)shows a united triple arthrodesis on the left and right. On the right, there is residual posterior subluxation of the ankle, and this is thought to be responsible for the residual equinus. This represents one of the risks of the technique, and we emphasize vigilance during the equinus correction phase to avoid posterior subluxation. Fig. 6 and 7 show the correction achieved clinically.
The right foot was treated in a similar fashion using a TrueLok-Hex Frame(Orthofix Verona, Italy) (Fig. 4). The procedures were combined with triple arthrodesis,and reduction and union were achieved using distraction osteogenesis. Both feet followed the same sequence. A plantar fascia release was performed to get some correction of the cavus to facilitate fixation in the frame.The Hoke procedure was performed to lengthen the Achilles tendon with percutaneous step cuts, allowing for its excursion during the correction process. The subtalar and calcaneocuboid joints were prepared for arthrodesis through a lateral approach. The medial approach was used for the talonavicular joint. The external fixator was applied with a full ring on the tibia and the foot. A laterally placed olive wire was placed in the talus to act as a fulcrum for correction. This was initially attached to the tibial frame, allowing correction to occur primarily through the subtalar joint. After a lag period of 7 days, gradual correction was started. Programming for the correction involved correction of the varus and internal rotation. After correction of these components, the talar wire was attached to the foot ring and equinus was corrected through the ankle joint by running a second adjustment programme. The frame was left in situ until consolidation of the arthrodesis had taken place. Intramedullary K-wires were inserted into the toes and kept throughout the duration of the correction to protect the metatarsophalangeal joints and prevent clawing of the toes. Time in frame for the left foot was 4 months and 4.1 months for the right. The arthrodesis was united at the time of frame removal for both feet,and no further casts or orthotics were needed.Pin track complications were minimal,and no antibiotics or exchanges were needed. The only complication was a posterior talar subluxation on the right during the equinus correction phase, which was corrected with a residual program. The patient was followed up 12 months after the Ponseti-Hex procedures and reported no chronic pain. Both feet were corrected to achieve plantigrade painless feet. On the right, a residual equinus deformity of 20° remained(Fig. 5)shows a united triple arthrodesis on the left and right. On the right, there is residual posterior subluxation of the ankle, and this is thought to be responsible for the residual equinus. This represents one of the risks of the technique, and we emphasize vigilance during the equinus correction phase to avoid posterior subluxation. Fig. 6 and 7 show the correction achieved clinically.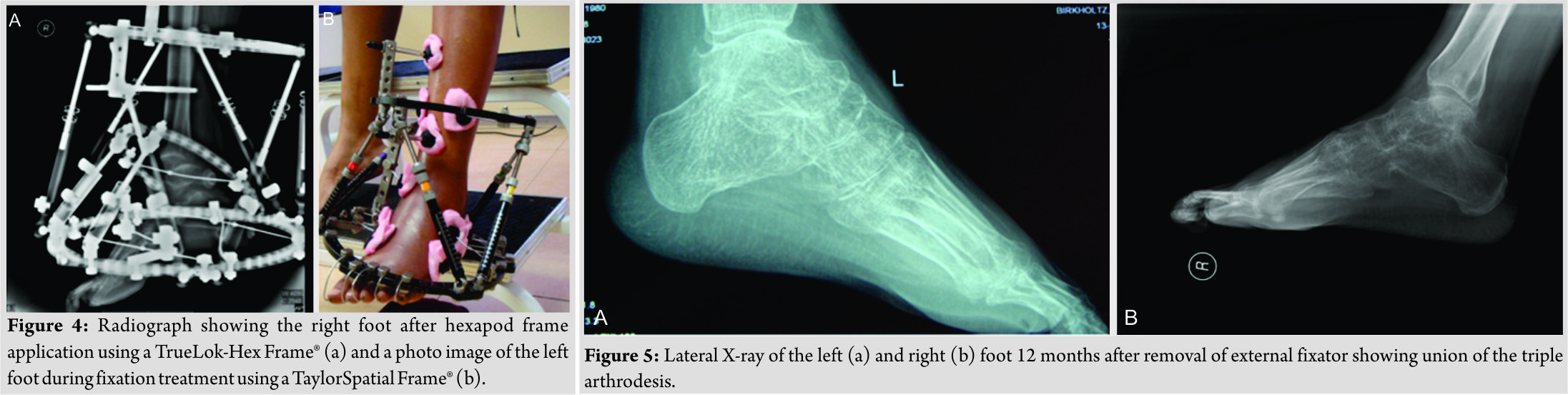 The patient was satisfied with the result and scored both feet at 0 on a visual analog score. The score was set between 0 and 10, with 0 being extremely happy and 10 being extremely unhappy. Her post-operative AOFAS score after 12 months of follow-up was 51 for the midfoot and 55 for the hindfoot on the left, representing a vast improvement from the pre-operative scores. The patient’s walking distance improved from 50m to approximately 600m, with the use of crutches. She could also walk without crutches for short distance indoors. Her ankle range of motion on the right was 10°–10°–30° on the right, with the foot unable to reach neutral. On the left, it was 20°–0°–10°. The midfoot and forefoot joints showed functional ranges of motion. The Laaveg and Ponseti functional score was 72 on the left, which is rated as fair [3]. Finally, gait analysis showed results consistent with that of stiff feet, with the patient having no real heel strike or toe off. The general gait pattern, along with the use of crutches, compensated for this. Although further surgery can correct residual equinus, the patient elected not to have additional surgery performed as she was comfortable with her functional outcome and appearance.
The patient was satisfied with the result and scored both feet at 0 on a visual analog score. The score was set between 0 and 10, with 0 being extremely happy and 10 being extremely unhappy. Her post-operative AOFAS score after 12 months of follow-up was 51 for the midfoot and 55 for the hindfoot on the left, representing a vast improvement from the pre-operative scores. The patient’s walking distance improved from 50m to approximately 600m, with the use of crutches. She could also walk without crutches for short distance indoors. Her ankle range of motion on the right was 10°–10°–30° on the right, with the foot unable to reach neutral. On the left, it was 20°–0°–10°. The midfoot and forefoot joints showed functional ranges of motion. The Laaveg and Ponseti functional score was 72 on the left, which is rated as fair [3]. Finally, gait analysis showed results consistent with that of stiff feet, with the patient having no real heel strike or toe off. The general gait pattern, along with the use of crutches, compensated for this. Although further surgery can correct residual equinus, the patient elected not to have additional surgery performed as she was comfortable with her functional outcome and appearance.
Discussion
Neglected clubfoot has been a problem of the developing world [11]. This has been attributed to a lack of education or the lack of or limited access to healthcare. Treatments have varied much in the past, including the use of corticosteroids, physical therapy,and supportive orthotics. A citation from 1932 suggested that a patient who received no treatment by 20 years will not benefit from correction and amputation should be offered [5, 6]. Sobel et al. stated that achievement of a pain-free, plantigrade foot in neglected adult clubfeet required surgery. They treated three patients with acute corrections. The surgical procedure consisted of extensive posterior plantar medial release with double arthrodesis involving calcaneal cuboid wedge resection and talonavicular fusion. This corrected the hind foot, provided minimal shortening, and restored a plantigrade position. Postoperatively, the patients were kept in a below-knee cast for 2 months. All three patients were reported to have cosmetically acceptable feet with good functional results [5]. Various treatment regimens have been proposed, with varying amounts of success, for residual or neglected clubfeet. One such regimen, popularized by Ilizarov, employed differential distraction of the deformity using a circular external fixator. Soft tissue structures medially and laterally are distracted differentially to achieve a plantigrade foot [1]. The original technique was criticized for not following normal biomechanics of the foot. This criticism was based on complications seen. These included physeal separation, planovalgus foot, tarsal subluxations, and joint contractures [3]. Grill and Frank were among the first to publish on the technique of differential distraction in 1987. Their study showed good results, with only minor complications in nine children with relapsed feet using an unconstrained Ilizarov external fixator [8,12]. Other studies have also shown promising results using this technique. Choi et al. were the first to use an unconstrained Ilizarov fixator combined with a laterally placed olive wire in the talus, toderotation ofthe talus. The hind foot, midfoot, and forefoot deformities were corrected simultaneously. Using this technique in 12 arthrogrypotic relapsed feet, plantigrade feet were achieved with improvements in the AOFAS scores [13, 14]. De La Huerta in 1994 reported his results on 12 neglected adult clubfeet using the Ilizarov differential distraction method. No corticotomies or osteotomies were performed. Frame time ranged from 5 to 8 months, and complete correction was achieved in all cases. There was a recurrence of adductus in three cases [1]. Ferreira et al.reported on a case series of 30 patients (38 feet) corrected with the Ilizarov method of distraction osteogenesis[15]. Achilles tenotomy and plantar fascia releases were performed before application of fixators. Average frame time was 16 weeks, after which a short-leg walking cast was applied for 6 weeks. An ankle-foot orthosis was then used for 6 months. 33 feet had a favorable outcome. Five feet were reported to have a poor outcome with a non-plantigrade foot with continuous pain. Early complications included a distal tibial fracture, a dislocation of the first metatarsophalangeal joint despite the use of intramedullary K-wires and arterial injury, resulting in toe amputations. 19 feet reported recurrence (50%), of which it was severe in only 5. Spontaneous ankylosis occurred in 28 feet (73.7%). Arthrodesis was performed on 9 feet (23.7%) for ankle or midfoot arthritis or residual deformity. The authors felt that this was a satisfactory method of correcting the deformity with minimal complications and avoidance of excessive shortening. They also felt that complexity of the deformity and stiffness and retraction of soft tissues limited the use of traditional osteotomies, talectomy, and modeling triple arthrodesis [15]. Ponseti has revolutionized the management of clubfoot in infants [2]. The serial manipulation and casting that are used are based on a sound understanding of ankle and subtalar kinematics [2, 3]. The first procedure is to correct the cavus by supinating the forefoot to line up with the hind foot. The second procedure is to push the foot into abduction, using the talus as a fulcrum. This is achieved by applying counter pressure using the thumb on the talar neck. The foot should be abducted to 60–70° to achieve correction of the subtalar joint and to stretch medial soft tissue structures. Equinus correction is then achieved with dorsiflexion, with or without Achilles tenotomy [2]. In the original study by Ponseti et al., children older than 6 years were excluded, as treatment in older children was considered too difficult, with the deformities being more rigid, soft tissues more contracted, and tarsal bones with altered shapes secondary to abnormal growth patterns[2, 3]. Tripathy et al. applied the Ponseti regimen for deformity correction in neglected and relapsed clubfoot using the Ilizarov fixator, treating 12 feet in two stages. Plantar fascia release and Achilles tenotomy were added to each of these stages. Total time in frame averaged 8.2 weeks. Improvements were noted in the Dimeglio score and the Laaveg and Ponseti functional score, and no complications were noted [3, 12]. Lamm et al. introduced the Ponsetaylor technique which applied Ponseti’s principles of correction using a hexapod external fixator[4]. A laterally placed olive wire in the talus serves as a fulcrum for correction and replaces the thumb that is placed on the talar neck in the Ponseti technique. In stage 1, the olive wire is attached to the tibial rings and the calcaneus is derotated. In the second stage, the olive wire is attached to the foot frame to allow for dorsiflexion of the ankle joint and correction of equinus [4, 13]. The Ponsetaylor technique has, to our knowledge only, been used in children. It has not been used in adults to achieve correction nor has it been used to achieve a triple arthrodesis. The technique presented combines all of these to achieve a plantigrade foot, using a hexapod external fixator. The limitations of the technique are that it is labor intensive and requires constant vigilance to avoid complications. The patient also needs to be able to cope with an external fixator.
Conclusion
The case reported here represents a new direction of thought for adult neglected clubfeet by combining triple arthrodesis, distraction osteogenesis, and three-dimensional corrective power of hexapod type circular fixators. The result achieved was plantigrade feet and a high level of patient satisfaction. Different types of hexapod circular fixators were used on each foot, and we, therefore, propose that a more generic name be used for this frame configuration and correction technique. We propose the Ponseti-Hex technique.
Clinical Message
Treatment of neglected clubfoot in the adult can be daunting. We combined a correction with a triple arthrodesis. The Chopart and subtalar joints were prepared, and a hexapod fixator was applied. Correction was then achieved with manipulation of the fixator in a manner that was based on Ponseti’s technique, also known as the Ponsetaylor technique. This technique was described for stiff neglected or residual clubfeet in children. The successful addition of the triple arthrodesis was done as we had an adult patient. The process needed constant vigilance and care of the fixator. Plantigrade feet were achieved with the patient being satisfied. This technique avoids the loss of bone and length associated with acute surgery.
References
1. De La Huerta F. Correction of the neglected clubfoot by the Ilizarov method. Clin Orthop Relat Res 1994;301:89-93.
2. Radler C. The Ponseti method for the treatment of congenital club foot: Review of the current literature and treatment recommendations. Int Orthop 2013;37:1747-53.
3. Tripathy SK, Saini R, Sudes P, Dhillon MS, Gill SS, Sen RK, et al. Application of the Ponseti principle for deformity correction in neglected and relapsed clubfoot using the Ilizarov fixator. J Pediatr Orthop B 2011;20:26-32.
4. Lamm BM, Standard SC, Galley IJ, Herzenberg JE, Paley D. External fixation for the foot and ankle in children. Clin Podiatr Med Surg 2006;23:137-66.
5. Sobel E, Giorgini R, Velez Z. Surgical correction of adult neglected clubfoot: Three case histories. J Foot Ankle Surg 1996;35:27-38.
6. Storen H. Operative treatment of clubfoot in older children and adults. Acta Orthop Scand 1949;18:233-65.
7. Pandey S, Pandey AK, Jha N. Management of neglected clubfeet. In: Simons GW, editor. The Clubfoot. New York: Springer-Verlag; 1994. p. 505-6.
8. Salinas G, Chotigavanichaya C, Otsuka NY. A 30 year functional follow-up of a neglected congenital clubfoot in an adult: A case report. Foot Ankle Int 2000;21:1037-9.
9. Fernandes RM, Mendes MD, Amorim R, Preti MA, Sternick MB, Gaiarsa GP, et al. Surgical treatment of neglected clubfoot using external fixator. Rev Bras Ortop 2016;51:501-8.
10. El-Sayed M. Ilizarov external fixation for management of severe relapsed clubfeet in older children. Foot Ankle Surg 2013;19:177-81.
11. Johnson RR, Friedman JM, Becker AM, Spiegel DA. The Ponseti method for clubfoot treatment in low and middle-income countries: A Systematic review of barriers and solutions to service delivery. J Pediatr Orthop 2017;37:e134-9.
12. Paley D. Specific ankle malalignment deformities. In Herzenberg JE, editor. Principles of Deformity Correction. Berlin: Springer-Verlag; 2005. p. 611.
13. Ganger R, Radler C, Handlbauer A, Grill F. External fixation in clubfoot treatment a review of the literature. J Pediatr Orthop B 2012;21:52-8.
14. Choi IH, Yang MS, Chung CY, Cho TJ, Sohn YJ. The treatment of recurrent arthrogrypotic club foot in children by the Ilizarov method. A preliminary report. J Bone Joint Surg Br 2001;83:731-7.
15. Ferreira RC, Costo MT, Frizzo GG, da Fonseca Filho FF. Correction of neglected clubfoot using the Ilizarov external fixator. Foot Ankle Int 2006;27:266-73.
 |
 |
 |
| Dr. Ziyaad Mayet | Dr. Annette-Christi Barnard | Dr. Franz Birkholtz |
| How to Cite This Article: Mayet Z, Barnard AC, Birkholtz F. Use of a Ponseti-hex Assisted Triple Arthrodesis: A Case Study of Bilateral Neglected Adult Clubfoot.. Journal of Orthopaedic Case Reports 2019 Jan-Feb; 9(1): 85-89. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


