
[box type=”bio”] Learning Point of the Article: [/box]
Check rein deformity is equally well managed with midfoot Z plasty.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 18-20 | Mohnish V Gadhavi, Drumil D Majmundar, Rajesh A Solanki. DOI: 10.13107/jocr.2250-0685.1350
Authors: Mohnish V Gadhavi[1], Drumil D Majmundar[1], Rajesh A Solanki[1]
[1]Department of Orthpaedics, B.J. Medical College and Civil Hospital Ahmedabad, Gujarat. India.
Address of Correspondence:
Dr. Drumil D Majmundar,
Department of Orthpaedics, B.J. Medical College and Civil Hospital Ahmedabad, Gujarat – 380016, India.
E-mail: drumil24@gmail.com
Abstract
Introduction: Checkrein deformities are rare and involve entrapment or fixed tethering of the flexor hallucis longus (FHL) tendon.
Case Report: We present the case of a 25-year-old male who presented with complaint of clawing of his great toe. A history of previous open reduction internal fixation for distal tibia fracture was described 3 years back. Exploration of FHL tendons was performed at the level of the midfoot. Correction was achieved after z-plasty of FHL tendon. This case highlights another late complication of distal tibial fracture which should be actively looked for in patients with this injury. We describe the ease of surgical correction through an operative field free of scar tissue as compared to classical method of operating near fracture site and releasing adhesions of muscle belly.
Conclusion: We suggest that exploration at the midfoot should be the primary surgical intervention in similar cases of checkrein deformity.
Keywords: Checkrein deformity, Constant length phenomenon, Flexor hallucis longus, Z-plasty
Introduction
Checkrein deformities are rare and involve entrapment or fixed tethering of the flexor hallucis longus (FHL) tendon in the posterior foot, just proximal to the flexor retinaculum of the ankle. In literature, it has been called the “constant length phenomenon” of FHL [1, 2, 3]. The deformity will occur secondary to non-operative or surgical correction of fractures of the distal tibia. Case reports have described different surgical interventions for the checkrein deformity such as release of adhesions at the fracture site, Z-plasty lengthening of FHL tendon at the fracture site with release of the adhesions, and Z-plasty of the FHL tendon at the midfoot without release of adhesions [5].
Case Report
We present a case of a 25-year-old male who presented with complaint of clawing of his left great toe. The patient had sustained a left-sided distal tibia fracture treated with open fixation of the tibia fracture 3 years ago. The implant was removed 18 months after the procedure due to the patient’s preference. After 6 months, the patient initially noticed clawing of his left great toe when he climbed stairs barefoot. He also complained that he had started to find it difficult to sit cross-legged, squat, as well as ride his bicycle due to the tightness he felt in his toes with certain ankle movements on examination, the patient walked with a normal bipedal unassisted gait. He had well-healed surgical scars and a plantigrade foot. Active dorsiflexion of the ankle joint produced an exaggerated flexion of the great toe. With the ankle held in dorsiflexion, it was not possible for the patient to actively or passively fully extend any of the toes (Fig. 1 and 2).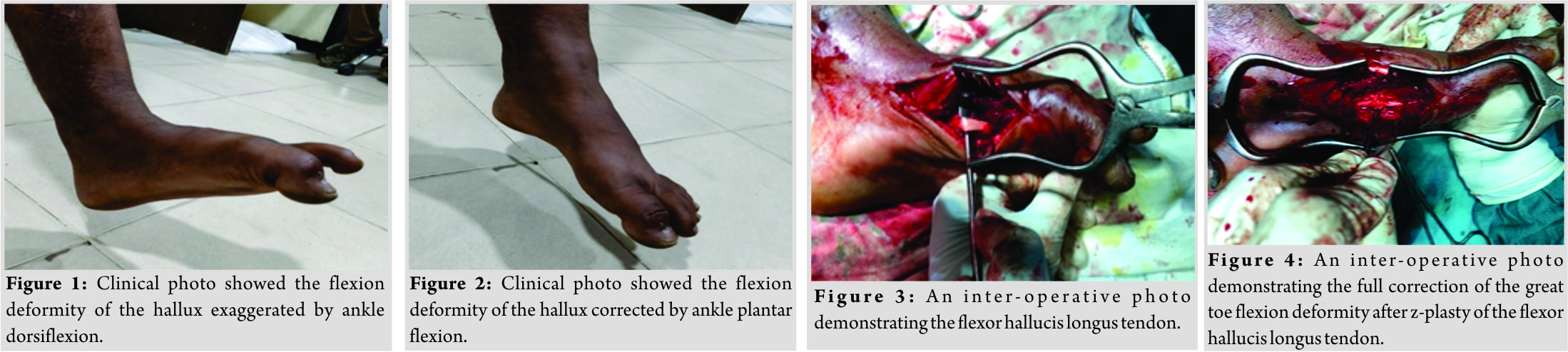 The diagnosis of checkrein deformity of the left great toe was made and attributed to the previous fracture of the distal tibia resulting in scarring or ischemic injury to the toe flexors. The possible patterns of injury could have been an isolated injury to FHL muscle or tendon causing fixed flexion of the great toe. The patient elected for surgical intervention and surgical exploration of FHL tendon at the level of the midfoot was planned. Exploration at the midfoot would give easier access to both tendons free from scar tissue making correction easier. The patient was suitably consented and the exploration was performed under spinal anesthetic with an inflated tourniquet at 250 mmHg. The tendon of FHL was identified (Fig. 3). Subsequent z-plasty of FHL tendon gave a full correction of the great toe flexion contracture (Fig. 4). The patient made an uncomplicated post-operative recovery and after final review, 3 months post-surgery had maintained the full range of movement in all toes (Fig. 5). Weight-bearing photograph is also shown before surgery (Fig. 6) and after surgery (Fig. 7).
The diagnosis of checkrein deformity of the left great toe was made and attributed to the previous fracture of the distal tibia resulting in scarring or ischemic injury to the toe flexors. The possible patterns of injury could have been an isolated injury to FHL muscle or tendon causing fixed flexion of the great toe. The patient elected for surgical intervention and surgical exploration of FHL tendon at the level of the midfoot was planned. Exploration at the midfoot would give easier access to both tendons free from scar tissue making correction easier. The patient was suitably consented and the exploration was performed under spinal anesthetic with an inflated tourniquet at 250 mmHg. The tendon of FHL was identified (Fig. 3). Subsequent z-plasty of FHL tendon gave a full correction of the great toe flexion contracture (Fig. 4). The patient made an uncomplicated post-operative recovery and after final review, 3 months post-surgery had maintained the full range of movement in all toes (Fig. 5). Weight-bearing photograph is also shown before surgery (Fig. 6) and after surgery (Fig. 7).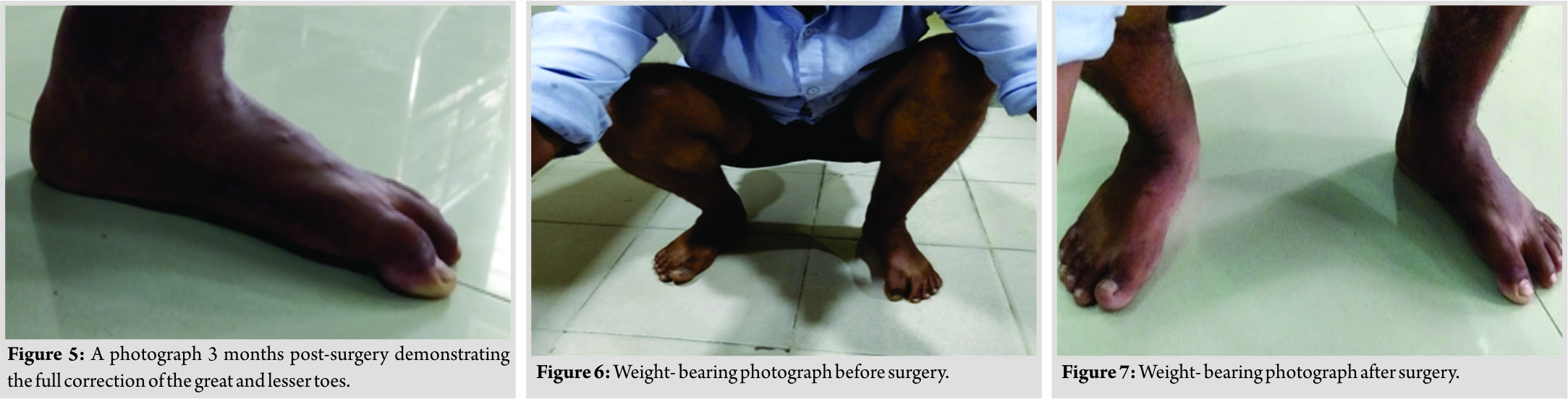
Discussion
Clawson first described the checkrein deformity following tibial fracture in 1974 [1]. The presumed causation for the deformity has been debated in the literature and ranges from a subclinical compartment syndrome due to fracture of talus, calcaneum, distal tibia, to direct scarring of FHL, and flexor digitorum longus (FDL) muscle bellies [2, 3, 4, 5]. This correlates well to the case presented above and we believe that the incidence is likely to be grossly under reported due to the variation in functional significance of the deformity. There have also been several surgical solutions suggested into how to correct the deformity [6, 7]. It is the opinion of all the authors that exploration of FHL and FDL tendons at the midfoot is the best surgical approach. This supports the opinion of Lee et al. [7] who presented a case series of 11 patients with similar deformities. They found midfoot exploration to be a better approach than performing a more proximal dissection. As demonstrated in this case, the simple exploration of an area free of scar tissue allows the easy identification of FHL tendon. This case highlights another possible complication of tibial fracture which should be actively looked for in patients with this injury. We describe and illustrate the ease of surgical correction through an operative field free of scar tissue. We suggest that exploration at the midfoot should be the primary surgical intervention in similar cases of checkrein deformity.
Conclusion
Checkrein deformities are rare and involve entrapment or fixed tethering of FHL tendon in the posterior foot, just proximal to the flexor retinaculum of the ankle. It is an important complication of tibial fracture, which can be managed by midfoot Z-plasty, as mentioned in our case.
Clinical Message
It is suggested that exploration of the midfoot should be the primary surgical intervention in cases of checkrein deformity.
References
1. Berentey G, Tamásy S. Adhesion of the tendon of the m. Flexor hallucis longus following tibial fracture. Magy Traumatol Orthop Helyreallito Seb 1973;16:161-8.
2. Burda R, Morochovic R, Kitka M. Hallux flexus-The result of posttraumatic entrapment of the flexor hallucis longus tendon in the tibial fracture site. Rozhl Chir 2010;89:466-7.
3. Clawson DK. Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-8.
4. Carr JB. Complications of calcaneus fractures entrapment of the flexor hallucis longus: Report of two cases. J Orthop Trauma 1990;4:166-8.
5. Leitschuh PH, Zimmerman JP, Uhorchak JM, Arciero RA, Bowser L. Hallux flexion deformity secondary to entrapment of the flexor hallucis longus tendon after fibular fracture. Foot Ankle Int 1995;16:232-5.
6. Carranza-Bencano A, Go´mez-Arroyo JA, Ferna´ndez-Torres JJ. Hallux flexus deformity due to entrapment of the flexor hallucis longus tendon after an open fracture of the tibia and fibula. Foot Ankle Surg 2000;6:133-5.
7. Rosenberg GA, Sferra JJ. Checkrein deformity-An unusual complication associated with a closed salter-harris Type II ankle fracture: A case report. Foot Ankle Int 1999;20:591-4.
8. Feeney MS, Williams RL, Stephens MM. Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-8.
9. Lee HS, Kim JS, Park SS, Lee DH, Park JM, Wapner KL, et al. Treatment of checkrein deformity of the hallux. J Bone Joint Surg Br 2008;90:1055-8.
 |
 |
 |
| Dr. Mohnish V Gadhavi | Dr. Drumil D Majmundar | Dr. Rajesh A Solanki |
| How to Cite This Article: Gadhavi M V, Majmundar D D, Solanki R A. Checkrein Deformity of the Great toe Managed by Midfoot Flexor Hallucis Longus Z-Plasty: A Case Report. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 18-20. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


