
[box type=”bio”] Learning Point of the Article: [/box]
It was important to remove the scar tissue surrounding the radial head.
Case Report | Volume 9 | Issue 3 | JOCR May-June 2019 | Page 30-33| Daichi Shinohara, Tomohiro Yasuda, Masayuki Arai, Kaoru Sato, Toshihiko Arima, Koji Kanzaki. DOI: 10.13107/jocr.2250-0685.1406
Authors: Daichi Shinohara[1], Tomohiro Yasuda[1], Masayuki Arai[1], Kaoru Sato[1], Toshihiko Arima[1], Koji Kanzaki[1]
[1]DepartmentofOrthopaedics, Fujigaoka Hospital, Showa University School of Medicine, Yokohama, Japan.
Address of Correspondence:
Dr. Daichi Shinohara,
Fujigaoka Hospital, Showa University School of Medicine, Yokohama, Japan.
Email: daichi09056@yahoo.co.jp
Abstract
Introduction: Monteggia fractures are rare and account for 1% of all pediatric forearm fractures. Dislocation of the radial head with plastic deformation of the ulna is particularly rare and can be overlooked, thereby resulting in long effects. Here, we report the treatment of a case of a long-standing Monteggia fracture in a child.
Case Report: A 6-year-old girl who was injured by a fall was examined by a local physician. 4 weeks later, she was referred to our hospital. Plain X-ray and computed tomography revealed a long-standing Monteggia fracture. Ulnar osteotomy was performed; however, complete realignment was not achieved. Scar tissue and the annular ligament remained intact, thereby hindering complete reduction. The scar tissue surrounding the radial head was surgically removed, and subluxation was reduced. The annular ligament was reconstructed, and the ulna was lengthened by external fixation. 1 year postoperatively, the patient’s elbow range of motion is good, and there has been no recurrence of radial head dislocation.
Conclusions: The patient achieved good progress through the use of annular ligament reconstruction and ulnar osteotomy to straighten and anatomically realign the ulna. Post-operative repeat dislocation was avoided by reducing radial head dislocation, removing the scar tissue, and reconstructing the annular ligament.
Keywords: Annular ligament reconstruction, External fixator, Monteggia fracture, Pediatric, Radial head dislocation.
Introduction
Pediatric forearm fractures are generally common and account for 20%–30% of all fractures [1]. Monteggia fractures are relatively rare, accounting for 1% of all pediatric forearm fractures [2]. It is relatively easy to treat fresh Monteggia fractures; however, for long-standing Monteggia fractures (chronic Monteggia lesions, i.e., those with unreduced dislocation of the radiocapitellar joint for 4 weeks [3]), the indications for surgery and the treatment methods remain controversial, and prognosis is not necessarily good. Here, we report on a patient with a long-standing Monteggia fracture that persisted for 4 weeks after injury. Good post-operative outcomes were achieved using ulnar osteotomy, bone lengthening, and annular ligament reconstruction.
Case Report
A 6-year-old girl was injured after falling off a kick scooter. A local physician diagnosed the injury as a left olecranon fracture, and she wore a splint for the following 3 weeks. Her plain X-ray revealed radial head dislocation and a proximal ulnar fracture (Fig. 1). A plain X-ray taken 1 month after injury revealed dislocation of the left radial head with surrounding calcification. The patient was referred to our department for examination due to persisting limited elbow range of motion. The patient exhibited considerably limited elbow range of motion at initial examination (flexion, 90°; extension, -25°; pronation, 90°; and supination, 0°) (Fig. 2). The plain X-ray also revealed anterior dislocation of the radial head with surrounding ossification as well as plastic deformation of the ulna (Fig. 3). Thus, a long-standing Monteggia fracture was diagnosed. The posterior elbow approach was used for surgery. Fasciotomy was performed using the Boyd approach, with an incision extending in a straight line from the olecranon to the triceps brachii muscle. Osteotomy of the proximal third-to-quarter of the ulna was performed, and the periosteum was preserved. Complete reduction could not be achieved using only ulnar osteotomy and straightening (Fig. 4).
The scar tissue and annular ligament remained intact, thereby hindering complete reduction (Fig. 5). The subluxation was reduced after surgically removing the scar tissue surrounding the radial head. The annular ligament was reconstructed using the Bell-Tawse method. Thereafter, 8 mm × 75 mm of the triceps muscle fascia was restored. To prevent obstruction of the triceps muscle fascia, two half-pins were inserted in the proximal and distal ulna, respectively. External fixation was performed using an Orthofix external fixator (M511). The correction angle was set at 20° (Fig. 6 and 7).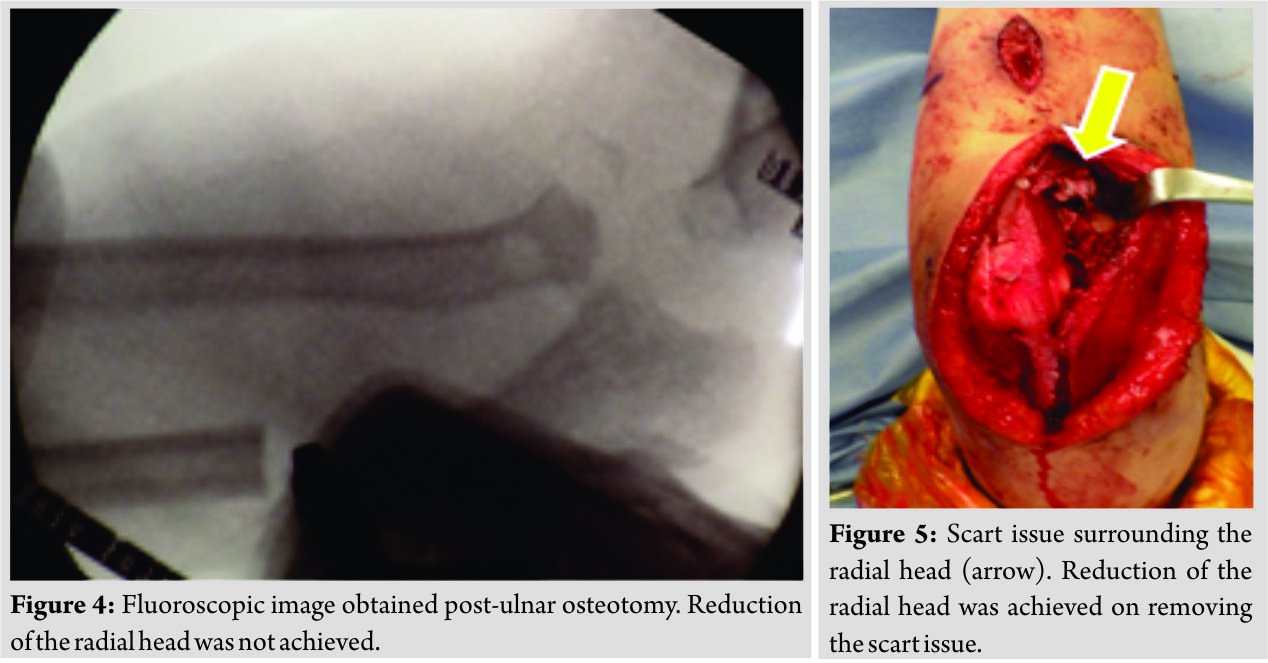
Furthermore, bone lengthening, and not bone grafting, was used. Bone lengthening at a rate of 0.5 mm/day for achieving a total of 7 mm was performed post-operative day 7 onward. 1 week postoperatively, elbow range of motion training was permitted without any limitations. Bone union was achieved at 8 weeks postoperatively, and the external fixation device was removed. At present, i.e., 1 year postoperatively, the patient’s elbow range of motion has considerably improved (flexion, 160°; extension, 10°; pronation, 75°; and supination, 75°), and the patient experiences no hindrance to daily life. The patient’s Mayo Elbow Performance Index was excellent (score, 100).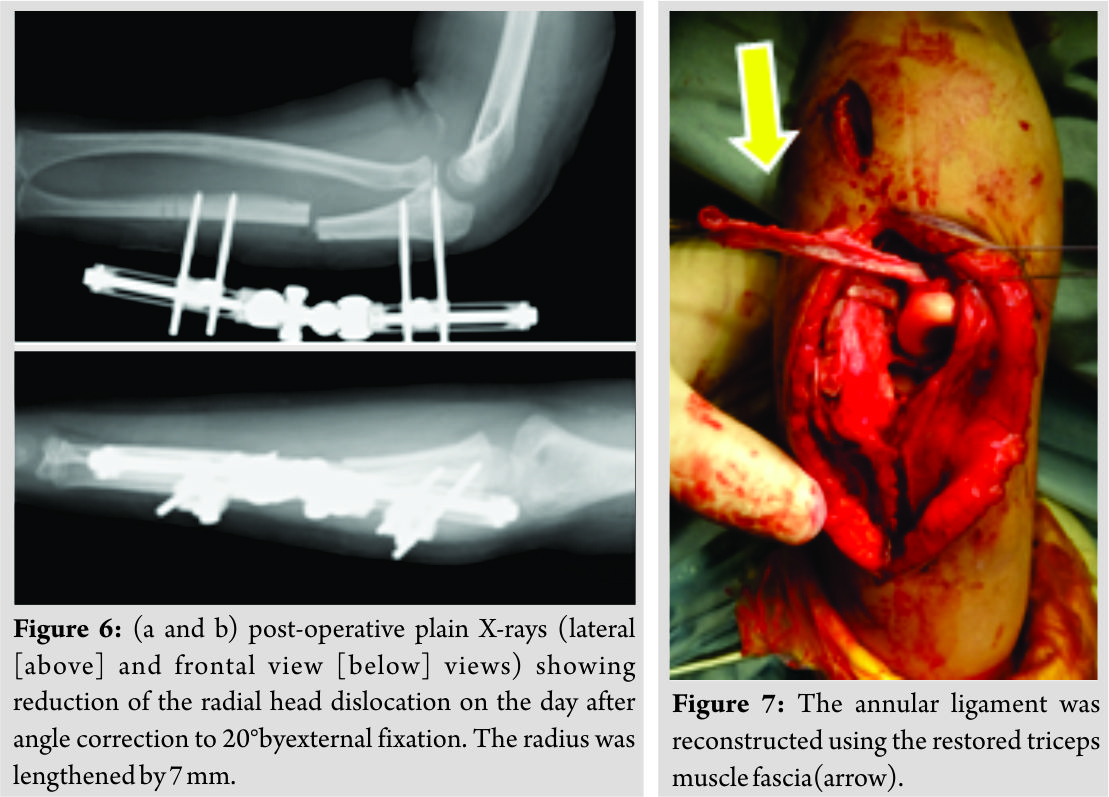
Discussion
The surgical indications for long-standing Monteggia fractures in children include pain, limited range of motion, and impaired functioning. In the treatment of radial head dislocation caused by a long-standing Monteggia fracture, early open reduction is performed when secondary deformities arise in the elbow and radial head reduction is possible; further, if impossible, treatment is administered on a case-by-case basis. Fowles et al. [4] reported that good outcomes can be achieved if surgery is performed within 3–6 months after dislocation. On the contrary, Seel and Peterson [5] reported that the patient’s age and the duration of the dislocation are unimportant factors. They claimed that the importance of performing surgery lies in the normal shape of the humeroradial joint and the correction of the ulna and radius deformity. In cases of long-standing Monteggia fractures in children aged <12 years, surgery should be performed to normalize the humeroradial joint. If left untreated, even without any problems in the short term, arthropathic changes, limited range of motion, radial nerve palsy, and ulnar nerve palsy may possibly develop in adulthood [6]. Wang and Change [7] reported that bone grafting is essential when the gap at the osteotomy site is =2 mm. Bor et al. [8] reported good outcomes with bone lengthening of 20 mm by correction using an Ilizarov frame. In our patient, we performed post-operative bone lengthening using an external fixation device with the bone lengthening function. Further, the periosteum was preserved when performing osteotomy. No post-operative problems were observed and bone union was achieved. Hirayama et al. [9] performed single-stage ulnar osteotomy and bone lengthening of 1 cm. They used plate fixation for the osteotomy site; however, problems arose in that the implant got damaged and subsequently loosened. In our patient, fixation was performed using an external fixation device with the bone lengthening function. This method was effective, and no damages to the implant were reported.
Surgical procedure
Surgery for long-standing Monteggia fractures in a child involves the following: (1) Annular ligament reconstruction, (2) ulnar osteotomy alone or combined with annular ligament reconstruction, and (3) radial osteotomy. Radial head osteotomy is usually not performed in children. Tajima and Yoshizu [10] reported better outcomes on performing ulnar osteotomy with annular ligament reconstruction. Similarly, some researchers have argued on the effectiveness of ulnar osteotomy combined with annular ligament reconstruction in children [11, 12]. On the contrary, there exist studies, wherein ulnar osteotomy alone has been performed, and the effectiveness of annular ligament reconstruction remains unclear [13]. Our patient presented with limited elbow range of motion; furthermore, although asymptomatic, radial head and neck strangulation were observed. Tendon tension at reconstruction and the suitable age for performing the procedure remains open to discussion. However, because annular ligament reconstruction appears relatively simple, it should be performed concurrently as required.
In our patient, the scar tissue and annular ligament remained intact, hindering complete reduction, which was not achieved despite performing ulnar osteotomy and straightening. Further, we believe that the good post-operative progress was achieved and post-operative repeat dislocation was avoided by reducing radial head dislocation, removing the scar tissue, and reconstructing the annular ligament.
Conclusion
We performed ulnar osteotomy and straightening, bone lengthening, and annular ligament reconstruction for a long-standing Monteggia fracture. While ulnar osteotomy and straightening are the basic treatment, it is important to remove the scar tissue from the site of the radial head.
Clinical Message
In case of chronic anterior Monteggia lesions, the remainder of the annular ligament and the scar tissue became an obstacle to the reduction of the radial head. It was important to remove the scar tissue surrounding the radial head.
References
1. Noonan KJ, Price CT. Forearm and distal radius fractures in children. J Am Acad Orthop Surg 1998;6:146-56.
2. Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-24.
3. Stoll TM, Willis RB, Paterson DC. Treatment of the missed Monteggia fracture in the child. J Bone Joint Surg Br 1992;74:436-40.
4. Fowles JV, Sliman N, Kassab MT. The Monteggia lesion in children. Fracture of the ulna and dislocation of the radial head. J Bone Joint Surg Am 1983;65:1276-82.
5. Seel MJ, Peterson HA. Management of chronic posttraumatic radial head dislocation in children. J Pediatr Orthop 1999;19:306-12.
6. Minami A, Takahara M. Diagnosis and treatment of Monteggia fractures. MB Orthop 1991;36:87-97.
7. Wang MN, Chang WN. Chronic posttraumatic anterior dislocation of the radial head in children: Thirteen cases treated by open reduction, ulnar osteotomy, and annular ligament reconstruction through a boyd incision. J Orthop Trauma 2006;20:1-5.
8. Bor N, Rubin G, Rozen N, Herzenberg JE. Chronic anterior Monteggia lesions in children: Report of 4 cases treated with closed reduction by ulnar osteotomy and external fixation. J Pediatr Orthop 2015;35:7-10.
9. Hirayama T, Takemitsu Y, Yagihara K, Mikita A. Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna. J Bone Joint Surg Br 1987;69:639-42.
10. Tajima T, Yoshizu T. Treatment of long-standing dislocation of the radial head in neglected Monteggia fractures. J Hand Surg Am 1995;20:S91-4.
11. Degreef I, De Smet L. Missed radial head dislocations in children associated with ulnar deformation: Treatment by open reduction and ulnar osteotomy. J Orthop Trauma 2004;18:375-8.
12. Hui JH, Sulaiman AR, Lee HC, Lam KS, Lee EH. Open reduction and annular ligament reconstruction with fascia of the forearm in chronic Monteggia lesions in children. J Pediatr Orthop 2005;25:501-6.
13. Goyal T, Arora SS, Banerjee S, Kandwal P. Neglected Monteggia fracture dislocations in children: A systematic review. J Pediatr Orthop B 2015;24:191-9.
 |
 |
 |
| Dr. Daichi Shinohara | Dr. Tomohiro Yasuda | Dr. Masayuki Arai |
| How to Cite This Article: Shinohara D, Yasuda T, Arai M, Sato K, Arima T, Kanzaki K. ALong-standing MonteggiaFracture inaChild whounderwent Bone Lengthening andAnnular Ligament Reconstruction: ACase Report. Journal of Orthopaedic Case Reports 2019 May-June; 9(3): 30-33. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


