
[box type=”bio”] Learning Point of the Article: [/box]
In cases of displaced fracture of the distal phalanx, avulsion of flexor digitorum profundus tendon from its wide anomalous insertion should be kept in mind and such injuries should be treated with early open reduction and fixation to achieve satisfactory results.
Case Report | Volume 9 | Issue 3 | JOCR May-June 2019 | Page 65-67 | Amit Narang, Sumit Gupta, Rajesh Kumar Kanojia, Siddhartha Sinha. DOI: 10.13107/jocr.2250-0685.1424
Authors: Amit Narang[1], Sumit Gupta[1], Rajesh Kumar Kanojia[1], Siddhartha Sinha[1]
[1]Department of Orthopaedics, Lady Hardinge Medical College, New Delhi, India.
Address of Correspondence:
Dr. Amit Narang,
Department of Orthopaedics, Lady Hardinge Medical College, New Delhi -110001, India.
E-mail: draminarang@gmail.com
Abstract
Introduction: Avulsion injury of the flexor digitorum profundus (FDP) tendon, commonly known as jersey finger, is seen in contact sports players such as rugby and football. There are mainly three patterns of this type of injury as mentioned in the Leddy and Packer classification on the basis of the level of retraction of the tendon. Subsequently, a Type IV injury was added by Smith, where the tendon was also separated from the avulsed bony fragment. It is the level of tendon retraction and the status of the long and the short vincula post-injury that determines the outcome of repair in these types of injuries.
Case Report: Here, we report an unusual case of jersey finger injury in a 45-year-old male patient, where the FDP tendon was found in front of the middle phalanx with a large, fractured fragment of the middle third of the distal phalanx attached to it. This type of injury pattern has not been acknowledged in the commonly used classification systems. The patient was operated with open reduction and K-wire fixation of the bony fragment with a good functional outcome.
Conclusion: While treating the cases of jersey finger injuries in sports players and general population, one should be aware of such rare patterns which can then be easily managed with proper pre-operative planning.
Keywords: Jersey finger, Flexor digitorum profundus, Avulsion injury.
Introduction
Jersey finger is defined as avulsion of the flexor digitorum profundus (FDP) insertion from the base of the volar distal phalanx. The most common mechanism of injury is a forceful hyperextension of an actively flexed distal interphalangeal (DIP) joint. It is commonly seen in the ring finger FDP due to tethering effect of the FDP tendon by lumbricals in the palm [1,2,3]. The patient reports an inability to actively flex the DIP joint while making a fist and decreased pinch and grasp strength [4]. Here, we report an unusual pattern of jersey finger which does not fit in the previous classification system.
Case Report
A 45-year-old, right-hand-dominant, male desk worker presented to us with the chief complaint of inability to make a fist following an episode of injury when he was trying to get up from his chair and felt a popping sensation in his ring finger. At first, he ignored the pain and took some over the counter pain killers. After around 3 weeks of injury when the pain subsided, he noticed that he is not able to actively flex his ring finger completely. The medical history was not significant and there was no history of steroid use. On palpation, there was no tenderness along the ring finger, but there was swelling on the volar aspect around the middle phalanx. When asked to make a fist, his ring finger remained extended at the DIP joint (Fig.1). However, passive flexion was possible at DIP joint and range of motion at proximal interphalangeal (PIP), and metacarpophalangeal joints were within the normal range. We ordered radiographs of the hand in AP and oblique views with special focus on the ring finger and found that a fractured fragment from the distal phalanx was lying there in front of the middle phalanx (Fig. 2).
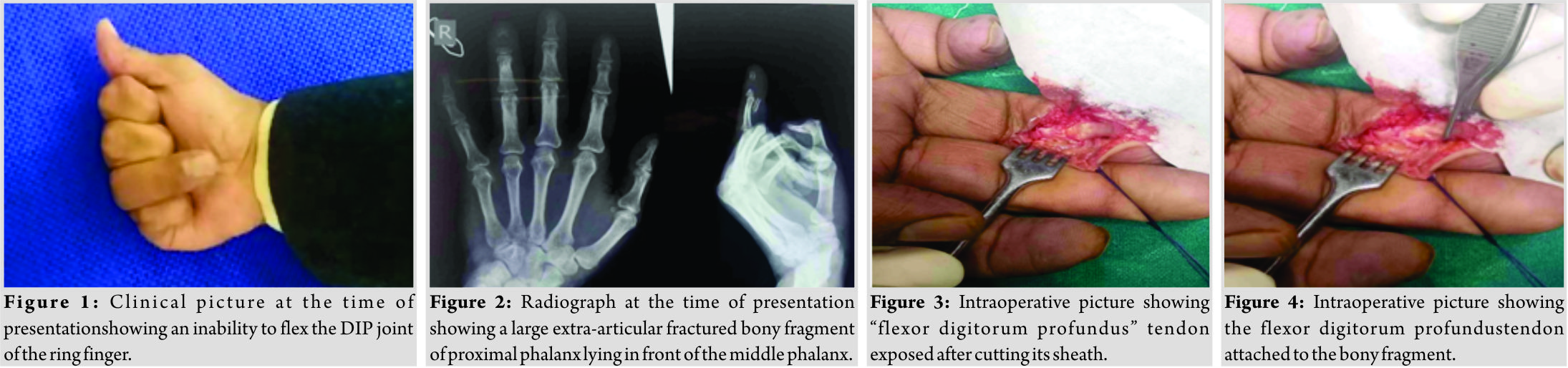 2 days after his visit, he was posted for surgery. The volar incision was used and the ring finger FDP tendon was found attached to the bony fragment. After a careful freshening of the margins, the bony fragment along with the attached tendon was reduced anatomically, and fixation was achieved using two K-wires (Fig. 3, 4, 5, 6, 7, and 8).
2 days after his visit, he was posted for surgery. The volar incision was used and the ring finger FDP tendon was found attached to the bony fragment. After a careful freshening of the margins, the bony fragment along with the attached tendon was reduced anatomically, and fixation was achieved using two K-wires (Fig. 3, 4, 5, 6, 7, and 8). 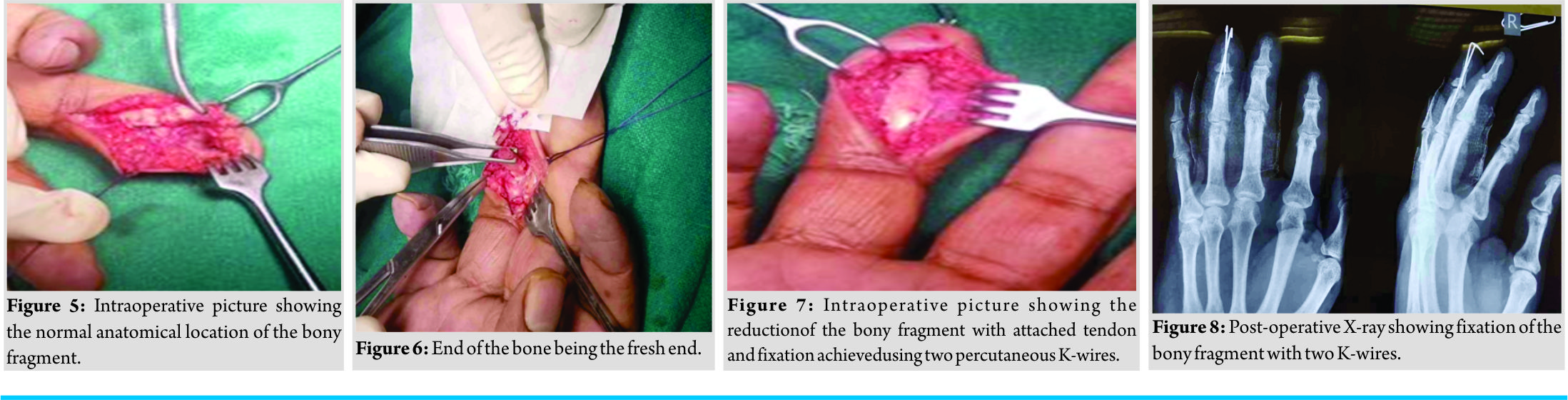 The patient was kept in a finger splint till 2 weeks when sutures were removed, and the wires were taken out at 3 weeks, and he was allowed active extension and passive flexion of the DIP joint. Gradually, he was allowed to pinch and grasp when the strength improved at 6 weeks. He was followed regularly every month initially and thereafter at 3 monthly intervals to a total of 1 year. At present, he is able to make a complete fist and is able to do all his routine activities without any difficulty (Fig. 9, 10, and 11).
The patient was kept in a finger splint till 2 weeks when sutures were removed, and the wires were taken out at 3 weeks, and he was allowed active extension and passive flexion of the DIP joint. Gradually, he was allowed to pinch and grasp when the strength improved at 6 weeks. He was followed regularly every month initially and thereafter at 3 monthly intervals to a total of 1 year. At present, he is able to make a complete fist and is able to do all his routine activities without any difficulty (Fig. 9, 10, and 11).
Discussion
Jersey finger injury is commonly seen in contact sports players following a tackle when the DIP joint is hyperextended. Usually, it is the avulsion fracture with attached FDP at the base of the distal phalanx, but isolated tendon ruptures without any bony injury are also seen. Our patient presented with a rare mode of injury where the tendon failed under loading when the patient tried to get up from the chair. Patients presenting with acute injuries come with pain and inability to flex the DIP joint, and usually, the pain subsides after 4–6 weeks and the only complaint is the inability to make a complete fist. Sometimes the level of retraction of the tendon can be identified if there is point tenderness along the course of FDP tendon. Above-mentioned clinical findings and a simple radiograph of the involved digit are enough to reach a diagnosis in cases of bony avulsion. However, with isolated tendon ruptures, an ultrasound of the involved digit or magnetic resonance imaging is useful modalities to reach a definitive diagnosis [5]. Leddy and Packer classified the jersey finger injuries into three categories:
• Type I: The FDP tendon is retracted into the palm and there is a rupture of the vincula leading to compromise of the blood supply.
• Type II: The FDP tendon is retracted to the level of the PIP joint and the long vinculum is spared thus preserving the blood supply.
• Type III: The FDP tendon is avulsed with a bony fragment and is at the level of A4 pulley [6].
Later on, a Type IV injury was described by Smith, where there is avulsion of the bony fragment and the tendon is also separated from the fractured fragment [7]. Rizis and Mahoney reported a case of FDP avulsion with an associated intra-articular fracture [8]. These types of injuries were earlier proposed by Al-Qattan as Type V injuries with further subtypes Va and Vb having extra-articular and intra-articular fractures, respectively [9]. However, in our case, the tendon was ruptured with a bony fragment of the middle one-third of the distal phalanx making it a unique pattern which has not been described earlier. Acute jersey finger injuries are usually treated operatively. In cases of chronic injuries, the preferred treatment option is chosen as per the patient requirements of the DIP function. Asymptomatic patients presenting with chronic ring finger injury can be left alone as they function well with the PIP joint flexion being preserved by the intact FDS tendon. Those requiring DIP joint function for intricate movements such as musicians are repaired with flexor tendon graft and patients who have persistent instability of the DIP joint are offered DIP joint arthrodesis [10]. In our case, the patient presented 3 weeks after the injury and he was concerned about his inability to use DIP joint function. Hence, he opted for surgical treatment. A volar surgical approach was used and FDP tendon was found to be attached to the large bony fragment, which was then anatomically reduced and fixed with percutaneous K-wires. Intraoperatively, there were no signs indicative of pathological fracture and it was concluded that the large bony fragment might be due to a broader and more distal insertion of FDP on the distal phalanx.
Conclusion
Not all the FDP avulsion cases can be classified according to the conventional classification systems. Hence, one must keep a high index of suspicion while dealing with such injuries and these rare injury patterns must be reported so that one will be vigilant while diagnosing and planning appropriate treatment for the patients.
Clinical Message
Such type of injuries can be tricky in terms of presentation and a detailed clinicoradiological examination is necessary with prior knowledge about the various types of injury patterns for better and prompt management of the patients.
References
1. Aronowitz ER, Leddy JP. Closed tendon injuries of the hand and wrist in athletes. Clin Sports Med 1998;17:449-67.
2. Tuttle HG, Olvey SP, Stern PJ. Tendon avulsion injuries of the distal phalanx. Clin Orthop Relat Res 2006;445:157-68.
3. Stamos BD, Leddy JP. Closed flexor tendon disruption in athletes. Hand Clin 2000;16:359-65.
4. Bachoura A, Ferikes AJ, Lubahn JD. A review of mallet finger and jersey finger injuries in the athlete. Curr Rev Musculoskelet Med 2017;10:1-9.
5. Goodson A, Morgan M, Rajeswaran G, Lee J, Katsarma E. Current management of Jersey finger in rugby players: Case series and literature review. Hand Surg 2010;15:103-7.
6. Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg Am 1977;2:66-9.
7. Smith JH Jr. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanxcase report. J Hand Surg Am 1981;6:600-1.
8. Rizis D, Mahoney J. A rare presentation of flexor digitorum profundus Type V avulsion injury with associated intra-articular fracture: A case report. Can J Plast Surg 2011;19:62-3.
9. Al-Qattan MM. Type 5 avulsion of the insertion of the flexor digitorum profundus tendon. J Hand Surg Br 2001;26:427-31.
10. Rettig AC. Athletic injuries of the wrist and hand: Part II: Overuse injuries of the wrist and traumatic injuries to the hand. Am J Sports Med 2004;32:262-73.
 |
 |
 |
 |
| Dr. Amit Narang | Dr. Sumit Gupta | Dr. Rajesh Kumar Kanojia | Dr. Siddhartha Sinha |
| How to Cite This Article: Narang A, Gupta S, Kanojia RK, Sinha S. An unusual Pattern of Flexor Digitorum Profundus Avulsion Injury with a Large Extra-articular Bony Fragment. Journal of Orthopaedic Case Reports 2019 May-June; 9(3): 65-67. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


