
[box type=”bio”] Learning Point of the Article: [/box]
The actions and inactions of patients and their relative may greatly influence treatment outcome bone malignancies. The similarities in the clinical presentation of benign and malignant bone tumours in many situations result in delay in accurate diagnosis and prompt treatment by clinicians.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 96-100 | Der Muonir Edmund, A D B Buunaaim, R Mikdad, Y Tolgou. DOI: 10.13107/jocr.2019.v09i04.1498
Authors: Der Muonir Edmund[1], A D B Buunaaim[1], R Mikdad[1], Y Tolgou[2]
[1]Department of Pathology, School of Medicine and Health Science of the University for Development Studies and the Tamale Teaching Hospital, Ghana, West Africa,
[2]Department of Surgery, School of Medicine and Health Science of the University for Development Studies and the Tamale Teaching Hospital, Ghana, West Africa.
Address of Correspondence:
Dr. Der Muonir Edmund,
Department of Pathology, School of Medicine and Health Science of the University for Development Studies and the Tamale Teaching Hospital, Ghana, West Africa.
E-mail: maadelle@yahoo.com
Abstract
Introduction: Management outcome of osteosarcoma as a primary bone malignancy is challenged in Ghana by many factors. We presented two male patients; aged 18 and 14 years, respectively, who were referred to the Tamale Teaching Hospital with advanced right knee tumors. Both patients had above knee amputation as part of treatment. The tumors were confirmed histologically as fibroblastic variants of osteosarcoma. The patients died within the immediate post-operative period without the initiation of the appropriate chemotherapy.
Conclusion: Unacceptable delay diagnosis and management of cancers worsened survival of patients. Education of patients, health workers and others along the patient management chain on the need early reporting and accurate diagnosis and management are recommended.
Keywords: Osteosarcoma, advanced presentation, prayer camps, herbal treatment, Ghana, Tamale.
Introduction
Osteosarcoma is cancer derived from primitive bone-forming mesenchymal cells and is the most common primary bone malignancy in children and adolescents [1, 2, 3, 4]. Secondary form of osteosarcoma is common in the elderly [3]. It has an estimated incidence of approximately 3–5 cases/million population per year in the United States of America [3]. African-American children have a higher risk of developing osteosarcoma than Caucasians [3]. Osteosarcoma as a primary bone malignancy typically occurs in young patients (10–20 years) with 75% taking place before the age of 20 years [3, 4, 5, 6, 7, 8, 9, 10]. This disease has a slight male predominance [3, 10]. The clinical features of malignant and benign bone tumors are a non-specific thus long period of time may elapse before definitive diagnosis may be made [4]. This category of bone tumors commonly present’s as a swelling involving the knee joint (distal femur and proximal tibia bones), with pain, limited mobility, and spontaneous fracture [10, 11]. The overlying skin may show features of acute inflammation, overstretched of ulcerated [10, 11]. There is very little published data on the clinicopathological features of osteosarcoma as a primary bone tumor in Ghana. We present two cases of advanced bone tumors beyond salvage, which were confirmed histologically as fibroblastic variants of primary osteosarcoma in two male patients aged 18 and 14 years, respectively
Case Report
Case one: Clinical history and physical examination findings
An 18-year-old adolescent male presented to the Accident and Emergency Department of Tamale Teaching Hospital (TTH) on November 2, 2016, with right knee ulcer of 5 months duration. In 2015, he noticed a swelling involving the right distal thigh that has progressively increased in size over the period. The swelling was associated with a constant severe at night. The patient also had a history of weight loss, anorexia, and inability to use the right lower limb. At the trauma and Orthopaedics Outpatient Department of the TTH, a working clinical diagnosis of a malignant bone tumor (osteosarcoma) was made, and the patient was advised to do a bone biopsy for confirmation and management decision. He was, however, sent home by her aunty and never returned until the current state she presented with a fungating ulcerated mass on the right knee joint. The mother admitted that after the first presentation to the hospital when they were asked to do a biopsy, the boy’s grandmother did not agree and decided to take him to about three different prayer camps for healing which never was and they resorted to treatment with herbal treatments. It was when all these attempts failed that she agreed for them to finally come back to the hospital without her presence. On examination, a young male adolescent who looked chronically ill, emaciated, with pallor of the mucous membranes, jaundice, and mildly dehydrated. Pulse on presentation was 96 bpm, blood pressure – 82/56 mmHg. There was a fungating and necrotic mass on the right knee joint, with raised irregular nodular edges, associated with enlargement of the thigh.
Investigations
1. Blood count: White blood cell (raised) 21.34 × 109/L (5.00–10.00), hemoglobin (low) 4.4 g/dl (12.0–16.0), and PLT- (Normal) 208 × 109/L
2. An abdominal ultrasound: Mildly enlarged and echogenic liver with moderate ascites and bilateral pleural effusion (asymptomatic).
3. Plain X-ray of the distal femur and knee joint: It showed sun-burst appearance, periosteal reaction with the formation of Codman’s triangle. There are complete medullary and cortical bone destruction and the formation of new bone in the soft tissues.
4. Plain chest X-ray: Metastatic lesions in both lung fields
5. Chest computed tomography scan: Multiple enhancing nodules of varying sizes with calcifications in both lung fields consistent with calcified metastases.
Working diagnosis: Osteosarcoma of right knee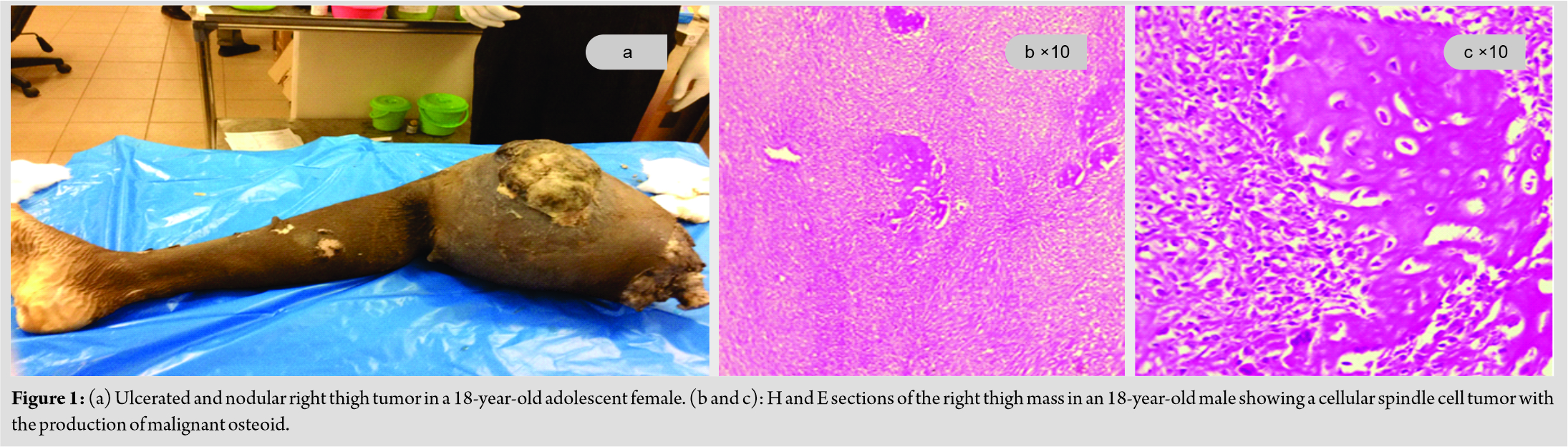
Management
The patient was managed with antibiotics, opioid analgesics, and transfused a total of 14 units of whole blood. The nutritionist was consulted to counsel on a diet. On November 11, 2016, patient had an above right knee amputation. Refashioning of the stump was done on December 12, 2016. On consultation with the oncologist, chemotherapy was to be started when the patient was optimized. The patient was discharged home on the February 3, 2107, and to start chemotherapy in 6 weeks. The patient was next seen at A and E on March 24, 2017, in respiratory distress and passed on a few hours after presentation.
Histopathology
Macroscopic features
A right above knee amputated (upper thigh) specimen was received in the department of pathology. It shows a swollen thigh with a raised nodular and necrotic tumor. Slicing through the thigh reveals a necrotic bony tumor that has destroyed the femur bony completely with infiltration of the skeletal muscles and the skin (Fig. 1a).
Microscopy
Sections of representative portions of the right thigh mass showed a cellular tumor predominantly composed of proliferating monomorphic spindle cells in interlacing fascicles. In areas, the tumor is composed of cells with plump hyperchromatic nuclei. There is production of osteoid by the malignant cells. There rare chondroblastic areas. Mitotic figures are present (Fig. 1b and 1c). The proximal resections margin is free of tumor. Histological diagnosis:Right lower limb (Above knee amputation): Osteosarcoma; fibroblastic variant
Case two
Clinical history and physical examination findings
A 14-year-old adolescent male presented to the accident and emergency unit of the Tamale Teaching (TTH), with a painful, huge ulcerated and necrotic right leg tumor of an unspecified duration. The condition began as small palpable and painful swelling for which the family had different treatment modalities from the herbalists. However, while on the herbal treatments, the lesion kept increasing in size, until 1 day he saw an ulcer over the swelling. The ulcer also subsequently increased in size; thus, extending from the right knee to involving the entire leg. 2 months before the presentation at the TTH; he sought medical attention at the Zebilla District Hospital in the Upper East Region of Ghana, where he was referred to TTH for further management. On examination, the patient was not pale, not jaundice, afebrile and hydration was satisfactory. He had a near circumferential (63.5 cm) fungating, nodular and necrotic right knee joint tumor that extends inferiorly to involve the entire leg. The tumor was soft to firm in consistency, pussy, and offensive. There was right inguinal lymphadenopathy (matted: 2.0 cm × 4.0 cm).
Investigations
1. Full blood count: Essentially normal.
2. Renal function test: Elevated blood urea level.
3. Liver function test: Elevated aspartate transaminase and alanine transaminase levels.
4. Abdominal ultrasound: Normal findings.
5. Plain X-ray of the proximal tibia and knee joint: It showed sun-burst appearance, periosteal reaction with the formation of Codman’s triangle. There are complete medullary and cortical bone destruction and the formation of new bone in the soft tissues.
Working diagnosis: Metastatic right knee osteosarcoma
Management
The patient was managed with intravenous antibiotics and opioid analgesics. The wound was cleaned and dressed with cotton and quaze. The treatment modality and the outcome were explained to relatives. The patient and the relatives were also counseled. The patient had 3 units of whole blood transfused and when hydration was accessed to be satisfactory, a right above knee amputation was done on March 15, 2017.
Histopathology
Macroscopy
Received a right above knee amputated specimen. It shows a near complete circumferential massively ulcerated nodular tumor with areas of necrosis and hemorrhages. The tumor spans the entire length of the leg (Fig. 2a). Slicing the specimen reveals a tan nodular and fleshy tumor that has completely destroyed the bones with infiltration of the skeletal muscles and the skin.
Microscopy
Sections show a tumor with highly cellular areas that alternate with loose myxoid areas. The tumor is composed of pleomorphic cells with plump to elongated nuclei with a vaguely fascicular pattern of growth (Fig. 2b). There is the production of malignant osteoid by the tumor cells. Scattered within a tumor is tumor giant cells and multinucleated giants (Fig. 2c). There are areas of necrosis and hemorrhages. Mitotic figures are abundant including abnormal forms.
Final histological diagnosis: Right knee (Above knee amputation): Osteosarcoma; fibroblastic variant.
Discharged summary: The oncologist was consulted to start chemotherapy, but the patient could not afford cost of treatment and further stay in the hospital, so patient requested to be discharged against medical advice. The patient later died at home a monthafter discharge.
Discussion
Primary osteosarcoma is a rare malignancy that may share similar clinical manifestation as any benign bone tumor [1, 2, 3, 4] thus a long period time may elapse before the tumor is diagnosed clinically and confirmed by histology. The age at presentation of patients with osteosarcoma has been reported to be common during the second and third decades of life [5, 6, 7, 8, 9, 10]. Both patients in the current case report, the first of its kind in northern Ghana is within this age category. Our patients were both males, and this is in line with studies that found this histological type of primary bone tumor to be common in males [3, 10]. Patients in this current case report, presented with huge, nodular and ulcerated knee tumors with complete destructions of the involved bones; all features of advanced clinical stage of bone disease. Osteosarcoma is a primary bone tumor that typically affects the metaphyseal region of long bones, with the distal femur and proximal tibia making up the majority of the cases [3, 5, 6, 7, 11, 12]. The anatomic location of the tumors in our patients was exclusively in the distal femur and proximal tibia and thus supports previous studies [3, 7, 8, 11, 12]. Furthermore, both patients had pulmonary metastasis at presentation, confirmed by plain chest X-rays. This is similar to reports of previous studies in Africa and beyond which documented that most patients with osteosarcoma had pulmonary metastasis at presentation [12, 13, 14]. For instance, Uribe-Botero et al. [13] in their study of the clinicopathological features of primary osteosarcoma found that almost all the patients had pulmonary metastasis at diagnosis. Similarly, Ferreira and Marais [14], in 2012, reported that 66.7% of their patients had metastatic disease, of which 75.0% was to the lungs. The histopathological reports on these cases did not only confirm fibroblastic variants of osteosarcoma but also gave description of gross picture of these cases. It is stated in the macroscopic sections of the reports that the tumors had completely destroyed the involved bones with the invasion of the skeletal muscle and skin as huge ulcers, thus beyond leg salvage as indicated in the gross histopathological descriptions. Amputation as surgical management of advanced bone tumors beyond salvage in this modern time has been documented by Lisenda et al. [15] study in South Africa. For instance, approximately 54.1% of their study population had limb amputations. None of the patients in this case report had the benefit of chemotherapy before they died within the immediate post-operative period. The fibroblastic variant of osteosarcoma is said to have a good prognosis compared to the osteoblastic and chondroblastic types [13, 14]. The relatively short survival in these patients potentially raises issues regarding the clinicopathological characteristics of the patients at presentation.
Sociocultural factors (patient and family):
In both cases, it cleared that the patient family had a role play in most countries i the support and management and the outcome of the treatment. However, in these cases family resulted in delay and hence the advanced and neglected state at presentation with the resultant poor outcome. The situation may be attributed high-level illiteracy in this part of the country, ignorance, accessibility, and the strong belief in traditional and herbal healers as demonstrated in this current report. These attributes are similar to those reported by Brown et al., (2015) in Ibadan; Nigeria [16]. Delay presentations and initiation of appropriate management modality for malignant bone tumors have been found to be associated with poor prognostic outcome. This may explained the outcome of cases in this case report.
The high cost of treatment:
Affordability of treatment in our health facilities is a major determinant of patient management and the outcome. The cost of managing many major surgical conditions, especially orthopedics and trauma are very high for the average Ghanaian particularly the rural folks. This is compounded by the additional cost for chemotherapy as in these cases. The picture is further complicated due to the fact that most patients on chemotherapy must do frequent blood investigations including hemoglobin, liver, and renal function tests. Although some of these investigations are covered by the national health insurance scheme, institutional laboratories have either faulty equipment or no reagents to perform these tests. Very sad situation and one wonders if our health delivery systems are meeting their missions and visions. In this situation, patients and patient relatives have to resort private medical laboratory with very high laboratory charges. This point is correctly illustrated in the two cases in this report. For instance, relatives of the second patient could not afford the cost of treatment and further stay in the hospital, so patient requested to be discharged against medical advice, and finally died at home.
The lack of infrastructure and qualified health personals in most parts of our country:
There is skewed distribution of health infrastructure across the length and breadth of our country Ghana. Most of the modern and well-equipped facilities are located within the southern part of the country with one or two within the northern part. For instance, it is the only the TTH in the northern region of Ghana that acts as a major referral point for specialist attention or cares for the three regions in the north and beyond. Patients who need specialist care are, thus, referred from the district and regional hospitals to the teaching hospital for further management. In the process, some patients and relatives may lose their lives through road traffic accidents. Some may not go at all, thus defeating the health care of the human being in question. Furthermore, most qualified specialist health personals in Ghana refused posting to other parts of the country, particularly the northern regions and this also deprives patients within these parts from the benefits of specialist care.
Conclusion
This case report illustrates the challenges patients go through in seeking for health in the northern part of Ghana and the factors that contribute to delay in receiving the appropriate medical care. Fibroblastic variants of osteosarcoma are known to be associated with good prognosis, but these two patients lost their limbs and eventually died from the disease because of the advanced stage at presentation.
Clinical Message
Most bony malignancies start as painless swellings and patients may give none or little attention to the condition. In most cases, native treatment is started by patient and only resort to health facilities when the primary clinical features are masked as in this case report. Again the similarities in the clinical presentation of benign and malignant bone tumours in many situations result in delay in accurate diagnosis and prompt treatment by clinicians.
References
1. Newman NJ. Perioperative visual loss after nonocular surgeries. Am J Ophthalmol 2008;145:604-10.e1.
2. Stewart RJ, Landy DC, Lee MJ. Unilateral acute angle-closure glaucoma after lumbar spine surgery: A case report and systematic review of the literature. Spine (Phila Pa 1976) 2016;41:E297-9.
3. Lee AG, Taber KH, Hayman LA, Tang RA. A guide to the isolated dilated pupil. Arch Fam Med 1997;6:385-8.
4. Gala PK, Henretig FM, Alpern ER, Sampayo EM. An interesting case of a unilaterally dilated pupil. PediatrEmerg Care 2013;29:648-9.
5. Pejic R, Klaric B. Transient anisocoria in a patient treated with nebulized ipratropium bromide. Am J Ophthalmol Case Rep 2017;7:11-3.
6. Steck RP, Kong M, McCray KL, Quan V, Davey PG. Physiologic anisocoria under various lighting conditions. ClinOphthalmol 2018;12:85-9.
7. Patel R, Davis C, Sivaswamy L. Anisocoria – Not always cause for alarm. J Pediatr 2014;164:1497.
8. Carey TW, Shaw KA, Weber ML, DeVine JG. Effect of the degree of reverse trendelenburg position on intraocular pressure during prone spine surgery: A randomized controlled trial. Spine J 2014;14:2118-26.
9. American Society of Anesthesiologists Task Force on Perioperative Blindness. Practice advisory for perioperative visual loss associated with spine surgery: A report by the American Society of Anesthesiologists task force on perioperative blindness. Anesthesiology 2006;104:1319-28.
10. Zimmerer S, Koehler M, Turtschi S, Palmowski-Wolfe A, Girard T. Amaurosis after spine surgery: Survey of the literature and discussion of one case. Eur Spine J 2011;20:171-6.
 |
 |
 |
| Dr. Der Muonir Edmund | Dr. A D B Buunaaim | Dr. Y Tolgou |
| How to Cite This Article: Der Muonir Edmund, A D B Buunaaim, R Mikdad, Y Tolgou. The Limb beyond Salvage: A Case Report on Two Cases of Fibroblastic Variants of Osteosarcoma. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 96-100. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


