
[box type=”bio”] Learning Point of the Article: [/box]
Harmless-looking tiffin box can cause significant injury. Proper documentation, evaluation, aggressive debridement, antibiotics, and assessment of soft-tissue involvement are key to the successful outcome.
Case Report | Volume 10 | Issue 1 | JOCR January – February 2020 | Page 19-21 | Maneesh Singhal, Pankaj Kumar, Sushma Sagar, Mantu Jain. DOI: 10.13107/jocr.2020.v10.i01.1620
Authors: Maneesh Singhal[1], Pankaj Kumar[2], Sushma Sagar[3], Mantu Jain[2]
[1]Department of Burn and Plastic Surgery, All India Institute of Medical Sciences, New Delhi, India,
[2]Department of General Surgery, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India,
[3]Department of Surgical Disciplines, Jai Prakash NarayanApex Trauma Center, All India Institute of Medical Sciences, New Delhi, India.
Address of Correspondence:
Dr. Pankaj Kumar,
Department of General Surgery,All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
E-mail: drpkushwaha@gmail.com
Abstract
Introduction: Although the penetrating injuries to the foot are common and sometimes they may be associated with calcaneum fracture, this case highlights a very rare injury by relatively harmless “Indian tiffin box.”
Case Report: A 30-year-old man was admitted to our hospital with a history of stepping over the Indian tiffin box. He presented with a tiffin box embedded in his right sole with food particles (pulses) inside the wound. It was associated with undisplaced, extra-articular fracture of calcaneus. Contamination with food particles and delayed presentation had added extra risk of infection. Aggressive management by wound lavage, debridement, and intravenous antibiotics has prevented the delayed complication like osteomyelitis.
Conclusion: Harmless-looking tiffin box can cause significant injury. Evaluation and proper management of soft-tissue involvement, especially heel pad, is very important due to its association to outcome. Proper documentation is equally important to avoid tricky medicolegal situations.
Keywords: Calcaneus fracture, heel pad injury, tiffin box.
Introduction
Indian lunch box (metallic) causing penetrating injury to the sole is never reported before. Although the penetrating injuries to the foot are common and sometimes they may be associated with calcaneus fracture, this case highlights a very rare injury by the relatively harmless “Indian tiffin box.”This injury was also associated with contamination, circumferential heel pad injury, and calcaneus fracture. Delayed complications are not uncommon after penetrating injury to foot involving the bone.
Case Report
A 30-year-old man was admitted to our hospital with a history of stepping over the Indian tiffin box. He presented with a tiffin box embedded in his right sole with food particles (pulses) inside the wound (Fig. 1). At the time of his arrival in the emergency department, he had complained of severe pain in the right sole, unable to walk, and mild bleeding from the wound with a tiffin box stuck to his sole. On assessment, the primary survey was normal. The secondary survey revealed a lacerated wound over the right sole with a tiffin box embedded and stuck in the sole. Food particles containing pulses were visible inside the wound. The wound was tender to palpation and the tiffin box was stuck. X-ray (Fig. 2) right foot revealed an undisplaced extra-articular fracture of calcaneus. Spine and contralateral foot were normal on physical examination and no other injury was detected. Tiffin box was removed under anesthesia. The wound was washed and food particles were removed (Fig. 3). The wound was left open and sutured after 2 days once culture report came negative. Ciprofloxacin was administered for 3 days. Non-operative management of calcaneus fracture was done with the below-knee plaster slab. He improved and discharged on day 4 without complications with paracetamol as an analgesic and below-knee slab. At 4 years follow-up, he is asymptomatic and walking normally.
Discussion
Penetrating injuries of the foot are very common. Sharp objects, such as glass, nails, tacks, ice picks, knives, teeth, wood pieces, seashells, and various other objects, are reported in literature to cause penetrating injuries. In developing countries like India, penetrating injuries to sole are more common due to habit of walking barefooted and very often, the culprit is an unusual object. Injury to Achilles tendon by Indian toilet and open tuber calcaneal fracture by meat cleaver are some rare injuries reported earlier [1, 2]. Indian lunch box (metallic) causing penetrating injury to the sole is never reported before. Special consideration, in this case, was the presence of overnight food particle inside the wound. Few authors have reported a high incidence of infection and complications in injuries occurring in forefoot and metatarsal head, due to lack of soft-tissue cover, but it may not be correct as mentioned by Siu et al. [3]. Retained and neglected foreign body results in even higher complication rates and significant morbidity [4]. Complications include osteomyelitis, deformity, and cellulitis. Delayed presentation increases the incidence of infection and complications. There is controversy regarding the optimal management of these wounds, but most published literatures have recommended aggressive management of proper cleaning, debridement, and antibiotics [3]. Staphylococcus, Streptococcus, Enterococcus, and Pseudomonas are commonly isolated organisms. Ciprofloxacin is usually recommended as a drug of choice for empirical therapy by most of the authors, considering it is a broad spectrum of activity and sensitivity against Pseudomonas. To properly manage the penetrating wounds, Resnick and Fallat had suggested a classification system and our case was of Type III B according to this system [5]. A similar attempt was made by Krych and Lavery to score the puncture wounds to decide the management protocol [6]. The total score, in this case, was more than nine. Accordingly, through wound lavage and removal of food particle were done. Considering the contamination with pulses, he was treated with a broad-spectrum antibiotic, ciprofloxacin for 3 days. Our patient had associated undisplaced extra-articular calcaneal fracture. Bony injury associated with contamination by pulses, caused by a weapon/tiffin box, which is usually harmless, makes this case interesting and worth reporting. We managed calcaneus fracture in this case, nonoperatively. Calcaneus fracture accounts for 60% of tarsal fracture with fall from height and road traffic accident as a common mode of injury. Such a fracture is associated with contralateral foot and spinal injury in about 10% of cases and if displaced requires a computed tomography evaluation [7]. Our case was unique due to the mode of injury with relatively simple bony configuration yet complicated with compounding and lodgment of food particles deep inside the tissue. The management of bony injury was straightforward as it was non-articular and undisplaced, but our main concern was of management of soft-tissue injury and preventing complications like osteomyelitis. Soft-tissue involvement is associated with high complications such as cellulitis and osteomyelitis, especially if treatment is delayed. Ligament and tendon involvement should also be evaluated properly and managed accordingly. Heel pad is a specialized soft-tissue structure for the purpose of weight-bearing. The unique anatomical arrangement of the elastic fibrous septa enclosing tightly packed fat cells makes it a perfect cushion to bear high loading stresses. However, injury, namely, avulsion in this complex arrangement, can throw constant challenges to the surgeon as no tissue can substitute the nature cushion. Management requires additional fixation methods such as K-wires rather than simple suturing, which can cause persistence of internal degloving, hamper the blood circulation to the heel pad, and finally pressure necrosis [8, 9]. Fortunately, the circumferential injury did not cause the avulsion of heel pad and the intermediate septa were intact. However, early suturing, such as delayed primary in our case, was of paramount importance to avoid heel pad-related complications.
Conclusion
“Indian tiffin box,” although looks harmless, due to its sharp edges, if significant force is applied, can cause fracture and pose significant management challenge. Associated contamination and delayed presentation can add extra risk of infection. Aggressive management by wound lavage, debridement, and intravenous (IV) antibiotics is necessary to prevent the delayed complication like osteomyelitis. Evaluation and proper management of soft-tissue involvement is very important due to its association to outcome. Heel pad has a significant role in weight-bearing; hence, aggressive management should be done to maintain its integrity.
Acknowledgment
The authors declared no conflict of interest. No funding was received for this study.
Clinical Message
Although the penetrating injuries to the foot are common and sometimes they may be associated with calcaneus fracture, this case highlights a very rare injury by relatively harmless “Indian tiffin box.” Associated contamination and delayed presentation have added extra risk of infection. Aggressive management by wound lavage, debridement, and IV antibiotics prevented the delayed complication like osteomyelitis.
References
1. DarTA, SultanA, DharSA, AliMF, WaniMI, WaniSA. Toilet seat injury of the Achilles tendon a series of twelve cases.Foot Ankle Surg2011;17:284-6.
2. TunaS, DuymusTM, MutluS, KetenciIE. Open tuber calcaneus fracture caused by a meat cleaver: A case report.Ann Med Surg (Lond)2015;4:221-4.
3. SiuA, WongT, LauC. Survey on plantar puncture injury in the emergency department.Hong Kong J Emerg Med2000;7:197-205.
4. ChandrashekaraCM, GeorgeMA, Al-MarboiBS. Neglected foreign body, the cause of navicular osteomyelitis in a paediatric foot: A case report.J Orthop Case Rep2013;3:26-9.
5. ResnickCD, FallatLM. Puncture wounds: Therapeutic considerations and a new classification.J Foot Surg1990;29:147-53.
6. KrychSM, LaveryLA. Puncture wounds and foreign body reactions.Clin Podiatr Med Surg1990;7:725-31.
7. PalmersheimK, HinesB, OlsenBL. Calcaneal fractures: Update on current treatments.Clin Podiatr Med Surg2012;29:205-20, 7.
8. JengSF, HsiehCH, LinTS, KuoYR, WeiFC. Classification and reconstruction options in foot plantar skin avulsion injuries: Follow-up.PlastReconstr Surg2003;112:220-1.
9. MohammedR, MetikalaS. Anchorage of partial avulsion of the heel pad with use of multiple kirschner wires: A report of four cases.JBJS Case Connect2012;2:e20.
 |
 |
 |
 |
| Dr. Maneesh Singhal | Dr. Pankaj Kumar | Dr. Sushma Sagar | Dr. Mantu Jain |
| How to Cite This Article: Singhal M, Kumar P, Sagar S, Jain M. Wrong Foot Forward– A Rare Injury by Indian Tiffin Box. Journal of Orthopaedic Case Reports 2020 Jan-Feb;10(1): 19-21. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Talus with Trimalleolar Fracture: A Three-planar Injury of Ankle Joint Complex: A Unique Case Report
May 1, 2025 Talus with Trimalleolar Fracture: A Three-planar Injury of Ankle Joint Complex: A Unique Case Report October 8, 2012 Distal Radius Fracture Hematoma Block with Combined Lidocaine and Bupivacaine can induce Seizures while within Therapeutic Window: A Case Report- Abstract
October 8, 2012 Distal Radius Fracture Hematoma Block with Combined Lidocaine and Bupivacaine can induce Seizures while within Therapeutic Window: A Case Report- Abstract December 10, 2021 Unusual Occurrence of Incarceration and Breakage of the Coiled Shaft of the Intramedullary Reamer during Closed Intramedullary Nailing of Tibia
December 10, 2021 Unusual Occurrence of Incarceration and Breakage of the Coiled Shaft of the Intramedullary Reamer during Closed Intramedullary Nailing of Tibia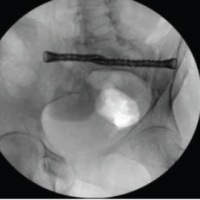 February 1, 2025 Stealth Navigation with iFuse-TORQ Implant for Sacroiliac Joint Fusion Technique Guide
February 1, 2025 Stealth Navigation with iFuse-TORQ Implant for Sacroiliac Joint Fusion Technique Guide


