
[box type=”bio”] Learning Point of the Article: [/box]
The fractures of the lateral end clavicle can be treated by indirect fixation technique in which the ethibond suture and mersilene tape are passed under the coracoid and through the clavicle. The technique is easy, inexpensive and lacks the side effects like hardware irritation.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 13-16 | Harshad G Argekar, Dipit Sahu. DOI: 10.13107/jocr.2020.v10.i02.1676
Authors: Harshad G Argekar[1], Dipit Sahu[1]
[1]Department of Orthopaedics, Dr. R.N. Cooper Municipal Hospital and HBT Medical College, Juhu Mumbai, Maharashtra. India.
Address of Correspondence:
Dr. Dipit Sahu,
Department of Orthopaedics, Dr. R.N. Cooper Municipal Hospital and HBT Medical College, Juhu Mumbai, Maharashtra, India.
E-mail: dip.it@me.com
Abstract
Introduction: Surgical management of Neer type 2 distal clavicle fractures may include tension band wiring, pre-contoured plate, hook plate or indirect fixation of coracoclavicular space by Endobutton, suture anchors, or Tightrope devices. We present our technique of suture and Mersilene tape fixation by passing them through the clavicle and under the coracoid which is a form of indirect fixation.
Technique: The fracture and the coracoid are exposed through a horizontal skin incision. The Mersilene tape and Ethibond suture are looped under the coracoid and then one limb of each is passed through the medial hole and then through the lateral hole to exit inferiorly and then tied underneath the clavicle, while the fracture is reduced.
Conclusion: Direct fixation by means of plate has good outcomes though high complication rate. Indirect fixation by means of Endobutton and Tightrope devices has shown successful outcome with less side effects. Our method of fixation by Ethibond suture and Mersilene tape is inexpensive while having the same principles of internal fixating the clavicle to the coracoid while the fracture heals.
Keywords: Distal clavicle fracture, mersilene tape, coracoclavicular fixation.
Introduction
Management of the distal clavicle fractures depends on whether the coracoclavicle ligaments are intact or ruptured [1]. Majority of the distal clavicle fractures can be managed non-operatively [1, 2]. Neer type 2 fractures have a partial or complete disruption of the coracoclavicle ligaments [1]. The pull of the trapezius muscle and the weight of the limb pulls the fracture ends far apart. Thus, these fractures are inherently unstable and have a non-union rate of 22–45% with conservative management [2, 3]. Conventionally, several different surgeries have been proposed to manage type 2 distal clavicle fractures such as tension band wiring, K-wire fixation, pre-contoured plate fixation, and hookplate fixation [2, 4, 5]. However, recently, there has been a trend toward minimal and indirect fixation between clavicle and coracoid [6]. The indirect fixation methods reduce and stabilize the fracture ends of the clavicle and the fracture heals by being converted into a stable configuration. Our purpose with this study is to describe our technique of coracoclavicle reduction and fixation with the help of an inexpensive Mersilene tape suture under the coracoid and through the clavicle (Under coracoid-through clavicle [UCTC]), which stabilizes the clavicle until the distal clavicle fracture heals. We describe here a case of type 2 distal clavicle fracture with a small distal fragment, which was managed by this technique.
Case Example and Surgical Technique
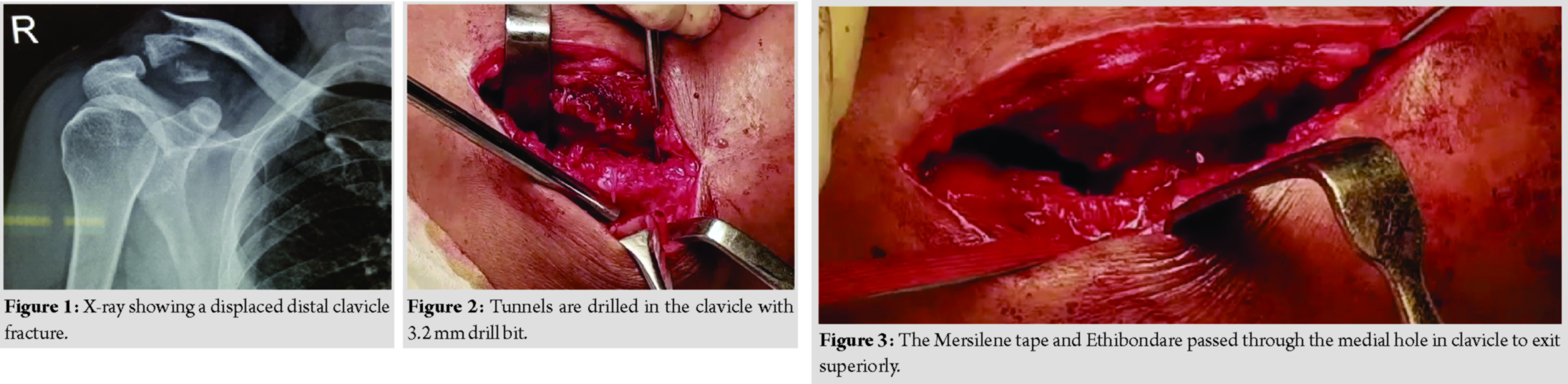
A 40-year-old patient presented to our facility, with a history of fall on the shoulder. After clinical and radiological examination, he was diagnosed with a distal clavicle Neer type 2B fracture (Fig. 1). The patient was operated within 1 week of the injury.
Surgical technique(Video 1)
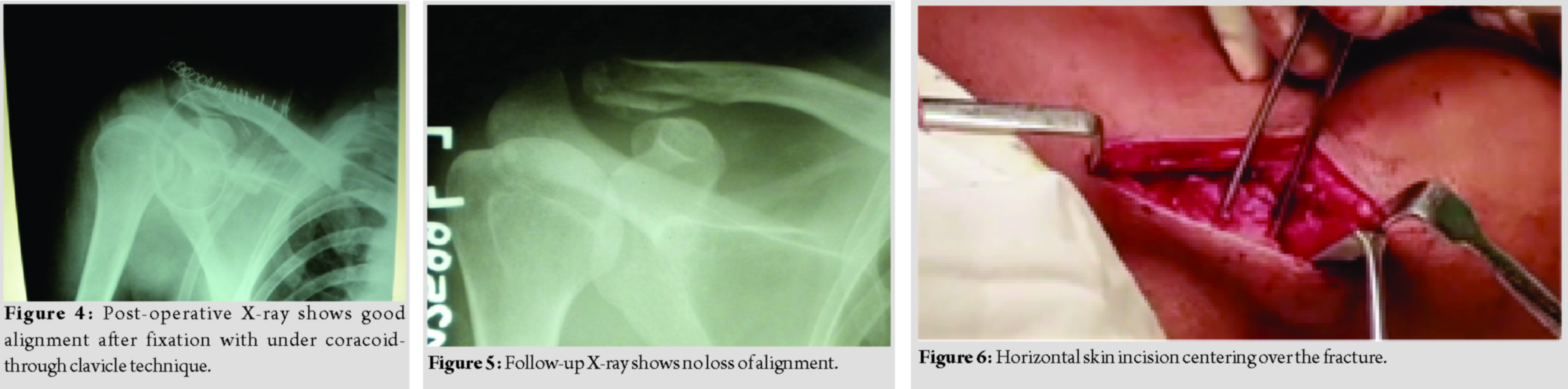
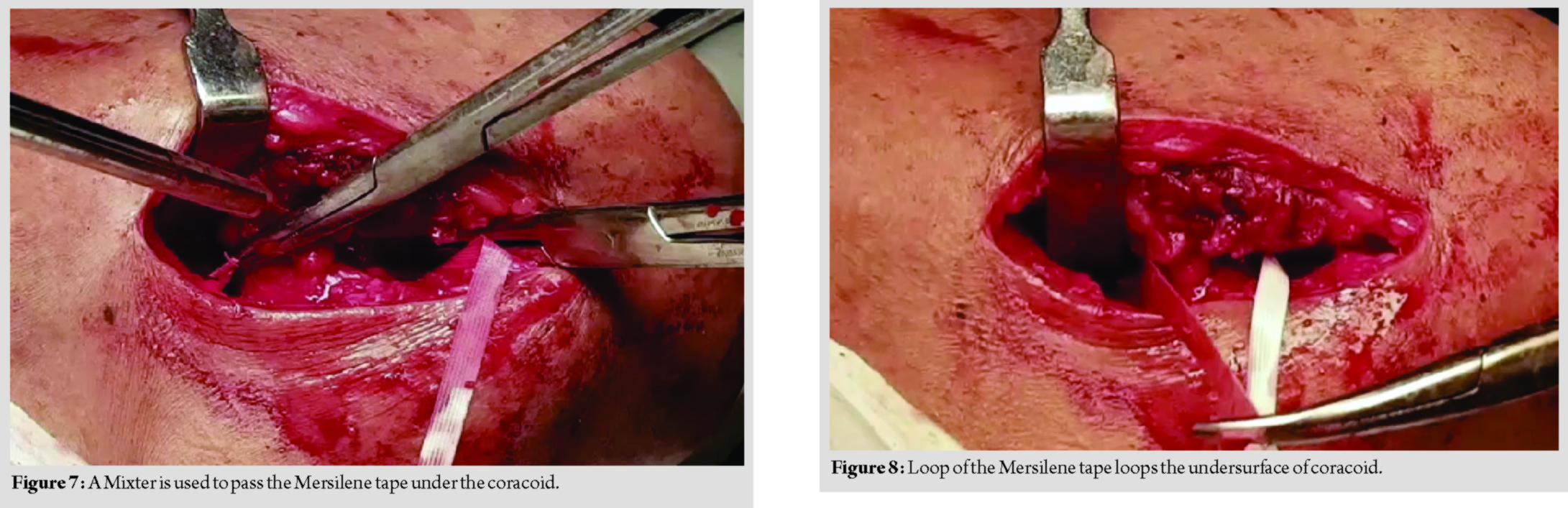
The patient was positioned supine on the operating table. A 5–6cm horizontal skin incision was utilized to expose the clavicle (Fig. 2). The deltoid-trapezoidal fascia was incised in line with the anterior border of the clavicle. The deltoid was divided along its fibers till the base of the coracoid was accessed. All the soft tissues from the superior surface of the clavicle were removed to gain access to the superior and inferior surface and to the distal and proximal fracture segments. The soft tissues were cleared from the medial and lateral end of the coracoid “knee” to enable passage of the sutures underneath the coracoid. A Mixter or a Satinsky clamp can beutilized to pass a Mersilene tape and Ethibond number 5 sutures below the coracoid from medial to the lateral side and near its “knee”(Fig. 3 and 4). Two holes, one each in the medial and lateral fragment, were drilled in the superior-inferior direction, 1–2 cm from the fracture site with the help of 3.2 mm drill bit (Fig. 5). One suture limb each of the Ethibond and the Mersilene tape was passed through the hole in the medial fragment in the inferior-superior direction (Fig. 6) and then passed through the second hole in the lateral fragment to exit inferiorly. The medial clavicle was reduced to the lateral end by a downward vertical pressure. First, the Ethibond was tied as it has good knotting properties and then the Mersilene tape was tied to give additional mechanical support. Since the knots were tied below the clavicle, there was no knot prominence or skin irritation. The deltoid-trapezius fascia and the skin are closed over the whole construct. Post-operative X-rays showed good reduction and opposition of the fracture (Fig. 7). Follow-up X-rays at 3 months showed good alignment with no loss of reduction (Fig. 8).
Discussion
Our technique of indirect reduction and stabilization of the unstable distal end clavicle fracture with the coracoclavicle suture construct has several distinct advantages. It provides good stability in the vertical plane, which balances the upward pull of the sternocleidomastoid muscle. Since the coracoclavicle ligament may be torn in type 2 fractures, a vertical plane reconstruction is thus logical and desirable for optimum stability. The sutures keep the fractures end in opposition with each other until the fracture heals. We have observed that no additional fixation by plates is necessary if the vertical plane stabilization by sutures is robust as per this technique. The fracture heals in 6–8 weeks and no implant removal is needed. As compared to other methods, this technique is also economically cheaper and readily available. Several methods have been described to treat unstable type 2 distal clavicle fractures. K-wire fixation from acromion to the proximal fragment, tension band wiring fixation, small fragment plating, distal radius plate fixation, hook plate fixation, and distal clavicle plate fixation are some of the direct fixation methods described in the literature [4, 7, 8, 9, 10]. However, some of the complications reported are migration of the K-wire, skin irritation by wires, plates, and wire loosening, non-union, and deep infection [7, 11]. Hook plates have been known to cause acromion osteolysis, rotator cuff rupture, acromion fracture, and migration of the hook in the acromion [2, 12, 13, 14]. If the distal fragment is small, the plate construct will not be able to have a stable construct. A second surgery may also be required for the removal of the plate or wires [15]. Some authors have recommended plate fixation along with the coracoclavicle suture construct [4, 16]. This construct has been proved to be biomechanically superior to a stand-alone plate fixation of the fracture [17]. Indirect methods of fixation have been recently described with good outcomes. Closed-loop Endobutton fixation, suture anchor fixation, dog bone fixation, and Tight rope fixation are some of the indirect methods, which have been used recently [6, 9, 18]. Coracoid-clavicle fixation has been proved to be biomechanically superior to plate fixation [19]. In addition, the coracoid-clavicle button fixation has been proved to be as biomechanically strong as the plate and button together [19]. However, drilling through the coracoid has resulted in coracoid fracture and neurovascular injury [20, 21]. Closed-loop Endobutton technique has been reported to have good outcomes, but it requires additional exposure and dissection of the undersurface of the coracoid with an open technique or a risk of eccentric placement of the coracoid hole through the arthroscopic techniques, while also increasing the cost of the treatment at the same time [22]. Cortical Endobutton construct has also been reported to fail overtime or subside in the clavicle cortex in few cases [23, 24].
Some authors have recommended passing the sutures around the clavicle or through one hole in the clavicle [25]. However, passing the sutures through two holes in the clavicle and then under the coracoid has a distinct biomechanical advantage in dissipating the forces over a large area than if passed through a single hole or using one Endobutton which might result in a construct failure. The UCTC technique described in this paper can be challenging if the fracture extends far into the medial or the lateral fragment making the placement of the holes, precariously close to the fracture. Alternatively, if the distal fragment is small, both holes can be made in the proximal fragment, while the rest of the technique remains the same. Theoretically, the suture construct can also cut through the clavicle bone over long term in osteoporotic bone.
Conclusion
The UCTC surgical technique described in this paper is a simple, cheap, and easily available option to stabilize the distal clavicle fractures. The fracture is reduced and stabilized indirectly by the suture construct, which results in predictable fracture healing.
Clinical Message
The fractures of the lateral end clavicle can be treated by indirect fixation technique, in which the Ethibond suture and Mersilene tape are passed under the coracoid and through the clavicle. The technique is easy, inexpensive and lacks the side effects of plate, screws, and metal irritation.
References
1. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin OrthopRelat Res 1968;58:43-50.
2. Oh JH, Kim SH, Lee JH, Shin SH, Gong HS. Treatment of distal clavicle fracture: A systematic review of treatment modalities in 425 fractures. Arch Orthop Trauma Surg 2011;131:525-33.
3. Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta OrthopScand1993;64:87-91.
4. Seyhan M, Kocaoglu B, Kiyak G, Gereli A, Turkmen M. Anatomic locking plate and coracoclavicular stabilization with suture endo-button technique is superior in the treatment of Neer Type II distal clavicle fractures. Eur J Orthop Surg Traumatol2015;25:827-32.
5. Lee SK, Lee JW, Song DG, Choy WS. Precontoured locking plate fixation for displaced lateral clavicle fractures. Orthopedics 2013;36:801-7.
6. Struhl S, Wolfson TS. Closed-Loop Double Endobutton Technique for Repair of Unstable Distal Clavicle Fractures. Orthop J Sports Med. 2016;4(7). Published 2016 Jul 26. doi:10.1177/2325967116657810
7. Kao FC, Chao EK, Chen CH, Yu SW, Chen CY, Yen CY. Treatment of distal clavicle fracture using Kirschner wires and tension-band wires. J Trauma 2001;51:522-5.
8. Andersen JR, Willis MP, Nelson R, Mighell MA. Precontoured superior locked plating of distal clavicle fractures: A new strategy. Clin OrthopRelat Res 2011;469:3344-50.
9. Shin SJ, Roh KJ, Kim JO, Sohn HS. Treatment of unstable distal clavicle fractures using two suture anchors and suture tension bands. Injury 2009;40:1308-12.
10. Tan HL, Zhao JK, Qian C, Shi Y, Zhou Q. Clinical results of treatment using a clavicular hook plate versus a T-plate in Neer Type II distal clavicle fractures. Orthopedics 2012;35:e1191-7.
11. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: A comparative study of Kirschner wire and clavicular hook plate fixation. Acta OrthopScand2002;73:50-3.
12. Lee YS, Lau MJ, Tseng YC, Chen WC, Kao HY, Wei JD. Comparison of the efficacy of hook plate versus tension band wire in the treatment of unstable fractures of the distal clavicle. Int Orthop2009;33:1401-5.
13. Chaudry SN, Waseem M. Clavicular hook plate: Complications of retaining the implant. Injury 2006;37:665.
14. Kashii M, Inui H, Yamamoto K. Surgical treatment of distal clavicle fractures using the clavicular hook plate. Clin OrthopRelat Res 2006;447:158-64.
15. Tiren D, van Bemmel AJ, Swank DJ, van der Linden FM. Hook plate fixation of acute displaced lateral clavicle fractures: Mid-term results and a brief literature overview. J Orthop Surg Res 2012;7:2.
16. Martetschläger F, Kraus TM, Schiele CS, Sandmann G, Siebenlist S, Braun KF, et al. Treatment for unstable distal clavicle fractures (Neer 2) with locking T-plate and additional PDS cerclage. Knee Surg Sports TraumatolArthrosc2013;21:1189-94.
17. Rieser GR, Edwards K, Gould GC, Markert RJ, Goswami T, Rubino LJ. Distal-third clavicle fracture fixation: A biomechanical evaluation of fixation. J Shoulder Elbow Surg 2013;22:848-55.
18. Zheng YR, Lu YC, Liu CT. Treatment of unstable distal-third clavicule fractures using minimal invasive closed-loop double endobutton technique. J Orthop Surg Res 2019;14:37.
19. Yagnik GP, Brady PC, Zimmerman JP, Jordan CJ, Porter DA. A biomechanical comparison of new techniques for distal clavicular fracture repair versus locked plating. J Shoulder Elbow Surg 2019;28:982-8.
20. Martetschläger F, Horan MP, Warth RJ, Millett PJ. Complications after anatomic fixation and reconstruction of the coracoclavicular ligaments. Am J Sports Med 2013;41:2896-903.
21. Milewski MD, Tompkins M, Giugale JM, Carson EW, Miller MD, Diduch DR. Complications related to anatomic reconstruction of the coracoclavicular ligaments. Am J Sports Med 2012;40:1628-34.
22. Lim TK, Oh WK. Intraoperative and postoperative complications after arthroscopic coracoclavicular stabilization. Clin Orthop Surg 2019;11:103-11.
23. Cho CH, Kim BS, Kwon DH. Importance of additional temporary pin fixation combined coracoclavicular augmentation using a suture button device for acute acromioclavicular joint dislocation. Arch Orthop Trauma Surg 2016;136:763-70.
24. Cho CH, Jung JH, Kim BS. Coracoclavicular stabilization using a suture button device for Neer Type IIB lateral clavicle fractures. J Shoulder Elbow Surg 2017;26:804-8.
25. Soliman O, Koptan W, Zarad A. Under-coracoid-around-clavicle (UCAC) loop in Type II distal clavicle fractures. Bone Joint J 2013;95-B:983-7.
 |
 |
| Dr. Harshad G Argekar | Dr. Dipit Sahu |
| How to Cite This Article: Argekar HG, Sahu D. Under Coracoid-through Clavicle Suture Fixation in Type 2 Distal Clavicle Fracture. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 13-16. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
- November 10, 2020 Intra-articular Olecranon Osteotomy and Adhesiolysis for Treatment of Post-traumatic Elbow Stiffness
 July 10, 2024 A Rare Case Report of Enchondroma of Triquetrum and Pisiform
July 10, 2024 A Rare Case Report of Enchondroma of Triquetrum and Pisiform October 1, 2024 Sclerotherapy as a Primary or Salvage Procedure for Aneurysmal Bone Cyst: A Case Report
October 1, 2024 Sclerotherapy as a Primary or Salvage Procedure for Aneurysmal Bone Cyst: A Case Report November 10, 2018 Yersinia enterocolitica Arthritis after Total Hip Arthroplasty – A Case Report
November 10, 2018 Yersinia enterocolitica Arthritis after Total Hip Arthroplasty – A Case Report


