
[box type=”bio”] Learning Point of the Article: [/box]
Anti-Tubercular chemotherapy is main treatment of foot and ankle TB.
Case Report | Volume 10 | Issue 5 | JOCR August 2020 | Page 24-26 | Amit Kumar Yadav, Prasanna Kumar G S, Akshay K S, Abhishek Harsoor, Akash Mane, Shaswat Mishra. DOI: 10.13107/jocr.2020.v10.i05.1822
Authors: Amit Kumar Yadav[1], Prasanna Kumar G S[1], Akshay K S[1], Abhishek Harsoor[1], Akash Mane[1], Shaswat Mishra[1]
[1]Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra. India.
Address of Correspondence:
Dr. Amit Kumar Yadav,
Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra. India.
E-mail: amit_aur09@yahoo.com
Abstract
Introduction: Osteoarticular tuberculosis (TB) constitutes 1-3 % of cases and about 10% of osteoarticular TB affects the foot and ankle. In foot, TB calcaneus is the most commonly affected bone.
Case Report: A 21-year-old male presented with pain, swelling in the right heel for 5 months and difficulty in walking for 2 months. Plain X-ray (axial) view of calcaneus showed a lytic lesion in calcaneus. Biopsy was done under local anaesthesia and histologic examination revealed a characteristic granuloma, caseous necrosis, and Langhans giant cells which confirmed our diagnosis. The patient was treated with anti-TB chemotherapy for 12 months. Radiographs at 18 months follow-up showed a healed lesion. At present, the patient is comfortable with no complaints.
Discussion and Conclusion: TB calcaneus is rare condition and a high index of clinical suspicion along with imaging studies helps in diagnosis. Conservative management with anti-TB chemotherapy for adequate duration helps in complete resolution of the infection with good functional results.
Keywords: Calcaneus, foot, tuberculosis.
Introduction
Tuberculosis (TB) is a disease caused by Mycobacterium tuberculosis that most commonly affect the lungs. Osteoarticular TB constitutes 1–3% of cases and about 10% of osteoarticular TB affects the foot and ankle [1]. In most of the studies of foot TB, calcaneus was the most common affected bone [1, 2, 3]. According to some authors, talus is the most common bone affected followed by the calcaneus [4]. TB of foot and ankle is difficult to diagnose due to lack of awareness among treating surgeons. Early diagnosis and treatment is important for better clinical outcome. Here, we report the case of isolated TB of right calcaneus treated conservatively with antitubercular medication and immobilization of the ankle joint with protected weight-bearing leading to a good functional outcome.
Case Report
A 21 year-old male presented with pain and swelling in the right heel for 5 months, had difficulty in walking for 2 months. There was no significant history of fever, weight loss, trauma, and other constitutional symptom of TB but had a history of pulmonary TB in childhood for which he had taken treatment. On clinical examination, there was deep tenderness and swelling in the right calcaneus. Local temperature was not raised and there were no discharging sinus and lymphadenopathy. Plain X-ray (axial) view of calcaneus shows a lytic lesion in calcaneus (Fig. 1). The magnetic resonance imaging (MRI) of the right ankle shows hypointense and hyperintense lesion on T1- and T2-weighted images, respectively (Fig. 2). Laboratory investigation showed positive C-reactive protein (CRP), raised erythrocyte sedimentation rate (ESR) with lymphocytosis. Plain radiographs of the chest were normal. After informed consent, core biopsy was done under local anaesthesia and C-arm guidance. On histopathological examination shows granuloma with caseous necrosis. Subsequently, gene expert and Ziehl-Neelsen (ZN) stain were found to be positive. Anti-TB medications were given which included isoniazid, rifampicin, pyrazinamide, and ethambutol for the first 3 months followed by isoniazid, rifampicin, and ethambutol for 9 months. Nil weight-bearing was advised, and foot was protected in a below-knee cast for 4 weeks. Partial weight-bearing was allowed at 4 weeks and progressed to full weight bearing at 12 weeks. X-ray and ESR and CRP were performed every 3 months till treatment completion. After 18 months, X-ray of the right ankle showing healed lesion (Fig. 3).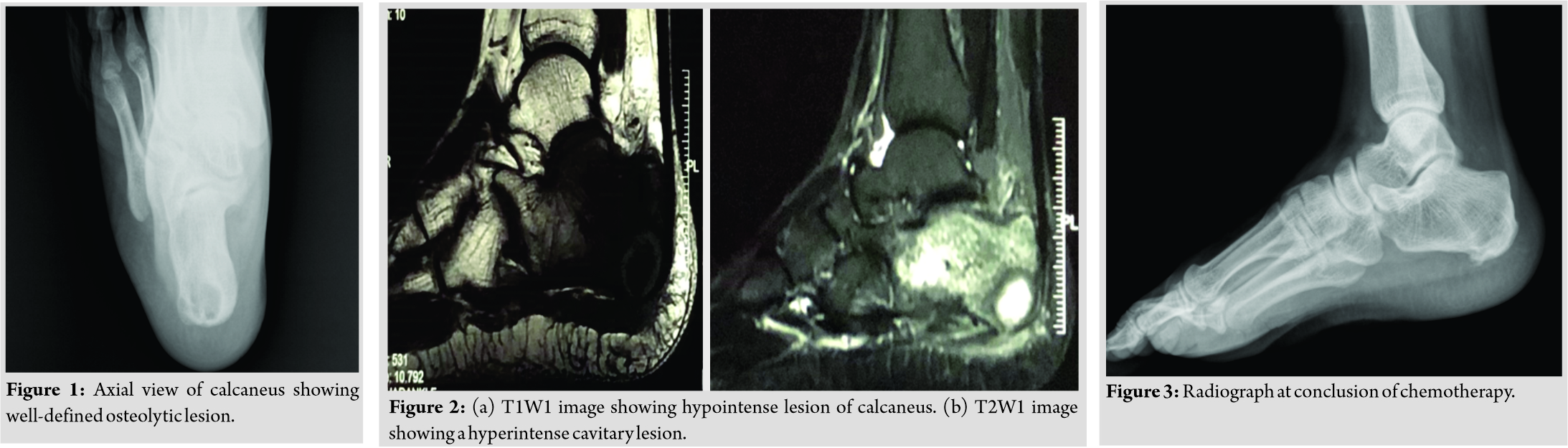
Discussion
Osteoarticular TB is <3% of the cases of extrapulmonary TB, of which about 10% involve the foot and ankle region [5, 6]. The most common affected foot bone is calcaneus and talus [2]. The classical constitutional symptoms of TB such as evening rise of fever and weight loss are absent in many cases of foot and ankle TB. As calcaneus TB is rare, its awareness among surgeons is low and diagnosis is often delayed [1]. Thus a high index of clinical suspicion is required in those with chronic symptoms not responding to routine treatment, in patients with a history of TB and HIV. Calcaneus TB is debilitating if untreated; delayed treatment may lead to functional disability [7]. Imaging in cases of suspected TB infection should always include a chest radiograph given that the disease’s primary focus is in the lungs [8]. Plain X-ray of ankle and foot may not show any specific sign or bone lesions of TB. By the time, foot radiographs demonstrate destructive bony changes, the TB disease process is already advance and capable of contiguous and/or hematological spread to distant sites [9]. Computed tomography scan shows sequestrum and involucrum earlier than plain X-rays and also useful for biopsy. MRI of foot and ankle shows bone marrow edema and is useful to identify pre-destructive phase of bone involvement and spread of disease into soft tissue. ESR and CRP are not specific to the diagnosis of TB. Biopsy and culture had the advantage of demonstrating the mycobacterial TB bacillus. Culture also allows testing for resistance and drug sensitivity. Due to paucibacillary disease, bacteria may not always be isolated in cultures or identified on ZN stain. Histologic examination reveals a characteristic granuloma, caseous necrosis, and Langhans giant cells. Anti-tubercular chemotherapy is the main treatment of foot and ankle TB. Treatment should start as early as possible and should continue for at least 12 months. Surgery for foot and ankle TB is indicated for obtaining tissue diagnosis, cases resistant to chemotherapy. Indications for surgery in healed phase are primarily for pain relief, deformity correction, or joint reconstruction [10].
Conclusion
TB calcaneus is rare so a high index of clinical suspicion with positive imaging finding, histopathological examination, staining for acid-fast bacilli could help us in diagnosis. Early diagnosis is crucial to prevent disease progression to the adjacent bones and joints. Conservative management with adequate anti-TB chemotherapy along with immobilization helped in complete resolution of the infection with good functional results. Surgery is indicated for cases resistant to chemotherapy deformity correction or joint reconstruction.
Clinical Message
In foot, TB calcaneus is the most commonly affected bone. Early diagnosis is crucial to prevent disease progression to the adjacent bones and joints. Anti-tubercular chemotherapy is the main treatment of foot and ankle TB.
References
1. Dhillon MS, Nagi ON. Tuberculosis of the foot and ankle. Clin Orthop Relat Res 2002;398:107-13.
2. Agarwal A, Qureshi NA, Khan SA, Kumar P, Samaiya S. Tuberculosis of the foot and ankle in children. J Orthop Surg (Hong Kong) 2011;19:213-7.
3. Mittal R, Gupta V, Rastogi S. Tuberculosis of the foot. J Bone Joint Surg Br 1999;81:997-1000.
4. Gursu S, Yildirim T, Ucpinar H, Sofu H, Camurcu Y, Sahin V, et al. Long-term follow-up results of foot and ankle tuberculosis in Turkey. J Foot Ankle Surg 2014;53:557-61.
5. Dhillon MS, Tuli SM. Osteoarticular tuberculosis of the foot and ankle. Foot Ankle Int 2001;22:679-86.
6. Dhillon MS, Singh P, Sharma R, Gill SS, Nagi ON. Tuberculous osteomyelitis of the cuboid: A report of four cases. J Foot Ankle Surg 2000;39:329-35.
7. Dhillon MS, Aggarwal S, Prabhakar S, Bachhal V. Tuberculosis of the foot: An osteolytic variety. Indian J Orthop 2012;46:206-11.
8. Beigelman-Aubry C, Godet C, Caumes E. Lung infections: The radiologist’s perspective. Diagn Interv Imaging 2012;93:431-40.
9. Korim M, Patel R, Allen P, Mangwani J. Foot and ankle tuberculosis: Case series and literature review. Foot (Edinb) 2014;24:176-9.
10. Dhillon MS, Agashe V, Patil SD. Role of surgery in management of osteo-articular tuberculosis of the foot and ankle. Open Orthop J 2017;11:633‐50.
 |
 |
 |
 |
 |
| Dr. Amit Kumar Yadav | Dr. Prasanna Kumar G S | Dr. Akshay K S | Dr. Abhishek Harsoor | Dr. Akash Mane |
| How to Cite This Article: Yadav AK, Kumar GSP, Akshay KS, Harsoor A, Mane A, Mishra S. Tuberculosis of calcaneus – A case report and review of literature. Journal of Orthopaedic Case Reports 2020 August;10(5): 24-26. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


