
[box type=”bio”] Learning Point of the Article: [/box]
Clinicians should be aware of possible subluxation of the proximal radio- capitellar and proximal radio-ulnar joints in association with isolated fractures of the radial shaft.
Case Report | Volume 10 | Issue 5 | JOCR August 2020 | Page 61-64 | Deepankar Verma, Saurabh Kumar, Ish Kumar Dhammi, Rajnand Kumar, Rajat Kapoor. DOI: 10.13107/jocr.2020.v10.i05.1840
Authors: Deepankar Verma[1], Saurabh Kumar[1], Ish Kumar Dhammi[1], Rajnand Kumar[1], Rajat Kapoor[2]
[1]Department of Orthopaedics, University College of Medical Sciences and Guru Teg Bahadur Hospital, New Delhi, India,
[2]Department of Orthopaedics, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
Address of Correspondence:
Dr. Saurabh Kumar,
Department of Orthopaedics, University College of Medical Sciences and Guru Teg Bahadur Hospital, New Delhi, India.
E-mail: srbrai@gmail.com
Abstract
Introduction: Isolated fracture of the radial diaphysis with dislocation of the radial head is a rare injury, which requires careful evaluation. Combined injuries associated with forearm shaft fractures and elbow dislocations are well recognized.
Case Report: A 35-year-old male presented to our emergency department with a history of fall in ditch under influence of alcohol with swelling of her right elbow and deformity of right upper limb. Roentgenograms showed oblique fracture of the radial shaft and dislocation of radial head posteriorly. He underwent open reduction and internal fixation of fracture with limited contact dynamic compression plate and reduction of radial head and fixing with radiocapitellar wire. After 4 months, the fracture healed fully and he had complete full range of elbow movements.
Conclusion: Ipsilateral radial head dislocation and radial shaft fracture are extremely rare injury in a child. A good outcome can be achieved by applying principles of the management of proximal forearm fracture-dislocation. Ipsilateral radial head dislocation and radial shaft fracture is extremely rare injury in a child. A good outcome can be achieved by applying principles of management of proximal forearm fracture-dislocation.
Keywords: Radius, fracture, radial head, dislocation.
Introduction
Isolated fracture of the radial diaphysis with dislocation of the radial head is a rare injury, which requires careful evaluation [1-4]. Combined injuries associated with forearm shaft fractures and elbow dislocations are well recognized. Fractures of the distal radial shaft with disruption of the distal radioulnar joint are referred to as Galeazzi fractures. In Monteggia fractures, dislocation of the radial head occurs in conjunction with fracture of the proximal ulna shaft [5, 6]. And finally, an Essex-Lopresti lesion [7] is characterized by a radial head fracture with distal radioulnar joint dislocation caused by an interosseous membrane disruption. We present an uncommon case of an isolated radial shaft fracture with an unreducable posterior dislocation of the radial head. The authors have obtained the patient’s informed written consent for print and electronic publication of the case report.
Case Report
A 35-year-old man under influence of alcohol fell in a ditch and sustained an injury to his right upper extremity. Clinical examination revealed swelling around the elbow and upper forearm. There was obvious flexion deformity of 30. There was no neurovascular deficit. There was no evidence of compartment syndrome. The patient’s elbow joint was evaluated carefully and showed no coronal instability on physical examination. Plain radiographic studies revealed a fracture middle one-third of radial shaft with a posterior-lateral dislocation of the radial head (Fig. 1). Attempts at reducing the radial head under sedation in the emergency ward were unsuccessful. An above elbow slab was put in the right extremity.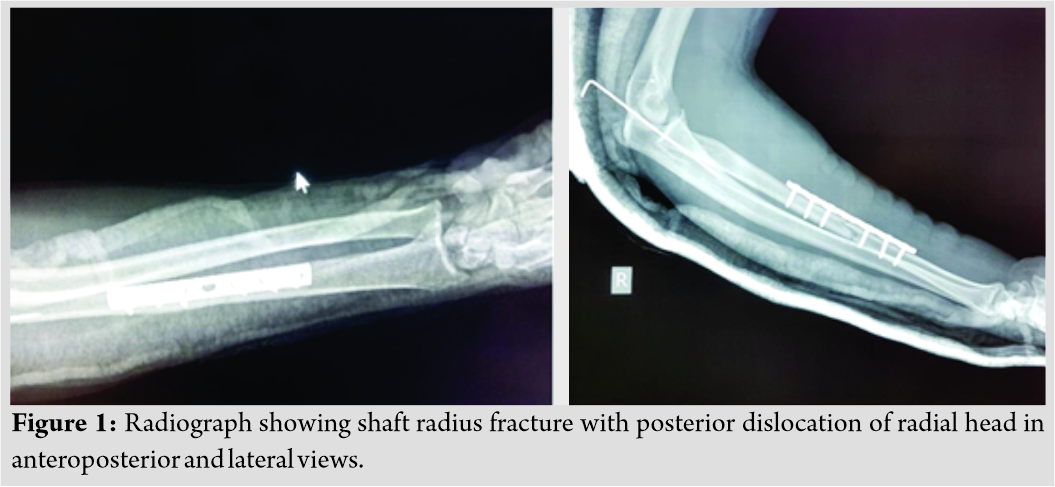
He was taken to the operating room the next day. An attempt was made to close reduce the radial head under fluoroscopy, but this could not be achieved. He then underwent open reduction and internal fixation of the radial shaft fracture through a Henry approach. The oblique fracture of radius was reduced and stabilized with a 7-hole 3.5 mm low contact dynamic compression plate on the volar aspect. Fluoroscopy in the operating room showed good reduction of the fracture but persistent widening of the radiocapitellar joint and the radial head dislocated posterior and laterally. Attempts to reduce the radial head with close reduction were unsuccessful. Next, the elbow joint was approached through Boyd’s approach, there was thick fibrocartilaginous soft tissue between radial head and capitellum. This was partially torn off annular ligament lying between radial head and capitellum. Once this soft tissue was removed, the head was reduced. However, it was still dislocating on 60–30 pronation. Hence, a radiocapitellar wire was put through radiocapitellar joint. X-ray showed good reduction of his radial head on the anteroposterior and lateral views (Fig. 2).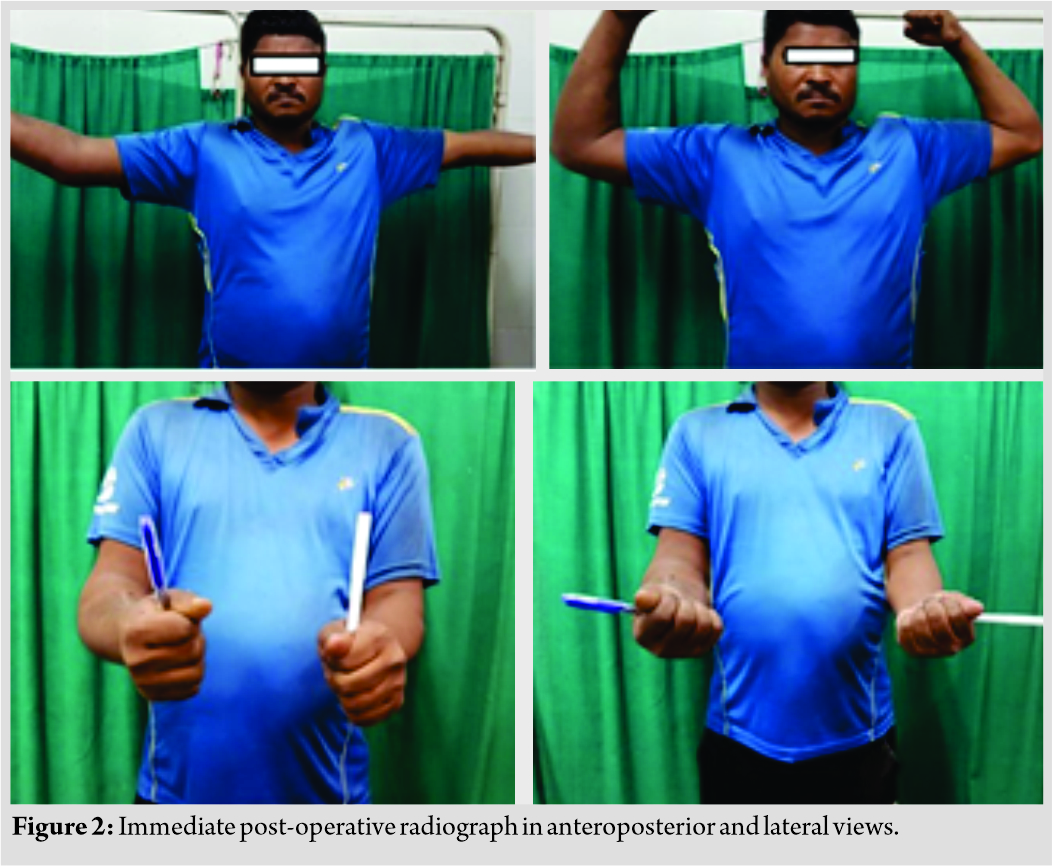 Postoperatively, the limb was immobilized in a splint at 90 of flexion and 45 of pronation. The radiocapitellar wire was removed at 3 weeks; then, he was started on gentle range of motion exercises after k-wire removal. At 6 months follow-up, range of motion of the elbow was 30 of extension to 120 of flexion and near-normal forearm pronation of 70 and supination of 60 (Fig. 3). On examination, he had no pain over the right forearm and his wounds were healed. At his last visit, 1 year after the operation, he had excellent range of motion with no major complaints. Radiographs showed that the fracture was healed in good alignment and the radiocapitellar joint remained reduced (Fig. 4).The patient reported no pain and was able to resume his normal daily activities, including working as a pharmacist.
Postoperatively, the limb was immobilized in a splint at 90 of flexion and 45 of pronation. The radiocapitellar wire was removed at 3 weeks; then, he was started on gentle range of motion exercises after k-wire removal. At 6 months follow-up, range of motion of the elbow was 30 of extension to 120 of flexion and near-normal forearm pronation of 70 and supination of 60 (Fig. 3). On examination, he had no pain over the right forearm and his wounds were healed. At his last visit, 1 year after the operation, he had excellent range of motion with no major complaints. Radiographs showed that the fracture was healed in good alignment and the radiocapitellar joint remained reduced (Fig. 4).The patient reported no pain and was able to resume his normal daily activities, including working as a pharmacist.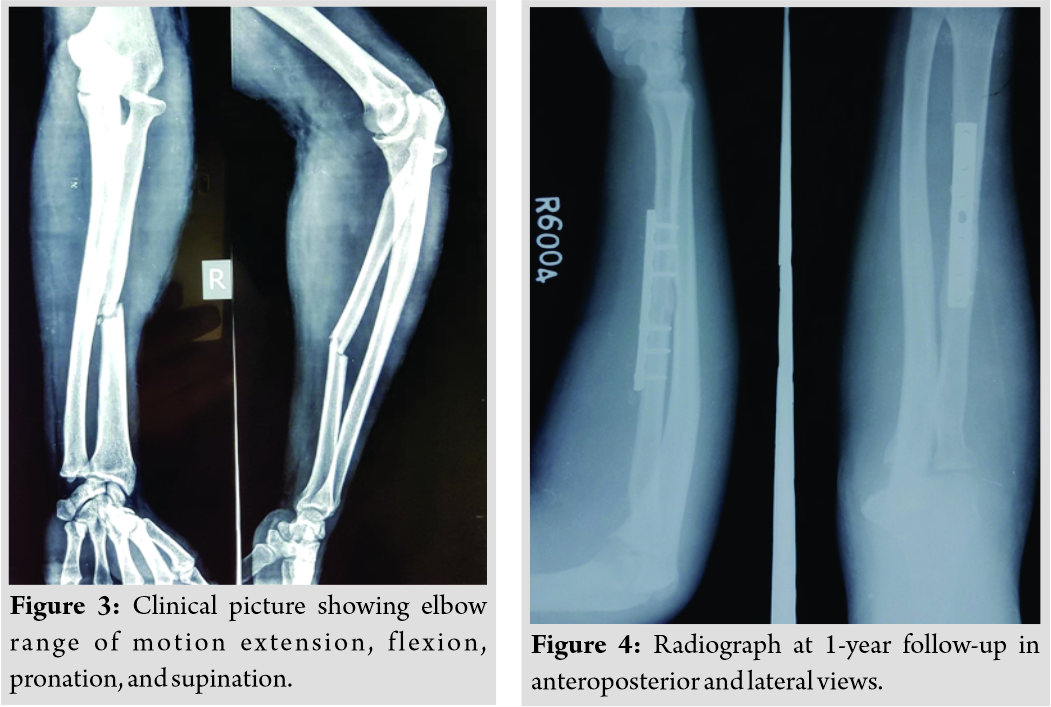
Discussion
Dislocation of the radial head is commonly associated with fracture of the proximal ulna. In 1814, Monteggia [8] first described this type of injury. It is somewhat unusual, accounting for only 1–2% of all forearm fractures [9]. Later, in 1967, Bado [10] further classified the injury into four types. Dormans and Rang [11] later added Type V to the Bado classification, which describes fracture of the radius with dislocation of the proximal radioulnar and the radiocapitellar joint. Cases of an isolated radial shaft fractures with elbow joint dislocations have been previously described [12-18]. However, isolated dislocation of the radial head with an associated radial shaft fracture is an extremely rare injury. Monteggia variants are of four types, (a) type I – isolated radial head dislocation, (b) type II – ulna and proximal radius (neck) fracture, (c) type III – isolated radial neck fracture, and (d) type IV – elbow dislocation (ulnohumeral) [19]. Simpson et al. [1] reported a case of a 29-year-old man that sustained an isolated proximal radial shaft fracture with anterior radial head dislocation caused by a fall on the outstretched forearm. Closed reduction of the radial head dislocation in the emergency room was unsuccessful. The patient was taken to the operating room. After applying direct traction on the proximal fragment, the radial head was reduced. The radial shaft was then reduced and stabilized with a dynamic compression plate supplemented with an autogenous cancellous graft. Mehara and Bahn [2] reported a concomitant traumatic anterior radial head dislocation with radial shaft fracture in a 25-year-old man due to a direct blow by a heavy wooden stick during a fight. Open reduction of the radial shaft fracture was impossible due to the subluxation of the radial head. The radial head was exposed through a separate incision and was found to dislocate anteriorly through a tear in the annular ligament. After reduction of the radial head, the shaft was reduced and fixed with a compression plate, Haddad [3] reported a case of a 37-year-old man who fell backward on his pronated right arm while playing football which resulted in radial shaft fracture with posterolateral radial head dislocation. The radial head was easily reduced with traction and pronation, and the radial shaft fracture was stabilized with dynamic compression plate. In our case report, the radial head was dislocated posterolaterally and was unreducable due to an interposed radial collateral ligament, requiring open reduction and repair of the collateral ligament. Recently, Linzel et al. [20] reported four cases of radial shaft fractures associated with dislocation of the proximal radioulnar joint. In two cases, closed manipulative reduction and plating of the radial shaft resulted in reduction of the proximal radial ulnar joint. In another patient, attempt to maintain the proximal radioulnar joint reduced was difficult after fixation of the radial shaft. With flexion of 110° and full supination, the radial head was able to be reduced in the operating room. Subsequent radiographs showed recurrent displacement of the radial head. This persisted despite a second operation which included realignment of the radial shaft fracture, open reduction of the proximal radioulnar joint, and repair of the annular ligament. The patient opted not to pursue additional treatment. In the last case, dislocation of the proximal radioulnar joint was noted 1 month after repair of the radial shaft. This patient required excision of the radial head due to restricted range of motion by the deformity. They had no reported cases of unreducable radial head dislocations. Shamian et al. [21] reported a case in a 30-year-old male with isolated radial shaft fracture with unreducable posterior dislocation of radial head with rupture of the lateral collateral ligament, in which plating was done for radius and open reduction was done for radial head with separate incision. The fracture united clinically and radiologically and the patient had excellent elbow range of motion. Jadaan et al. [22] reported a case in a 4.5-year-old child with ipsilateral radial head dislocation with shaft radius fracture in which nailing for radius shaft and open reduction for radial head was done. After 4 months, fracture healed completely and the child had full elbow range of motion. Singh et al. [23] reported a case with ipsilateral radial head dislocation and proximal one-third radial shaft fracture in an adult for which plating for radius and reduction of radial head was done at later stage. The patient had good functional outcome at 2-year follow-up.
Conclusion
Although a rare occurrence, clinicians should be aware of possible subluxation of the proximal radiocapitellar and proximal radioulnar joints in association with isolated fractures of the radial shaft. This joint incongruity may not reduce with fixation of the radial shaft and could require open treatment with repair of the collateral or annular ligament. After fixation of all forearm shaft fractures, careful clinical and radiographic examination of both the proximal and distal associated joints is imperative. The patient in our report had a successful clinical outcome and functional range of motion after rigid fixation of the radial shaft fracture and exploration of the elbow joint, reduction of the radial head, and repair of the lateral collateral ligament.
Clinical Message
Although ipsilateral radial head dislocation with radial shaft fracture is a rare entity, high index of clinical suspicion and urgent management by applying basic fracture-dislocation principles can give outstanding results.
References
1. Simpson JM, Andreshak TG, Patel A, Jackson WT. Ipsilateral radial head dislocation and radial shaft fracture. A case report. Clin Orthop 1991;266:205-8.
2. Mehara AK, Bahn S. Ipsilateral radial head dislocation with radial shaft fracture: A case report. J Trauma 1993;35:958-9.
3. Haddad FS. Radial head dislocation with radial shaft fracture. Injury 1995;26:502-3.
4. Cherif MR, Chehimi A, Ghozlen RB, Mbarek M. Traumatic dislocation of the radial head associated with ipsilateral fracture of the radial shaft: A case report. Acta Orthop Belg 2002;68:529-31.
5. Ovesen O, Brok KE, Arreskøv J, Bellstrøm T. Monteggia lesions in children and adults: An analysis of etiology and long-term results of treatment. Orthopedics 1990;13:529-34.
6. Stans AA, Heinrich SD. Dislocations of the elbow. In: Beaty JH, Kasser JR, editors. Rockwood and Green’s Fracture in Children. 6th ed., Vol. 2. Philadelphia, PA: Lipincott Williams &Wilkins; 2006. p. 661-70.
7. Wegmann K, Dargel J, Burkhart KJ, Brüggemann GP, Müller LP. The essex-lopresti lesion. Strategies Trauma Limb Reconstr 2012;7:131‐9.
8. Monteggia GB. Instituzioni Chirurgische. Milan: Maspero; 1814.
9. Kellam JF, Jupiter JB. Diaphyseal fractures of the forearm. In: Browner BD, Jupiter JB, Levine AM, Trafton P, Krettek C, editors. Skeletal Trauma. Philadelphia, PA: Saunders; 1992. p. 1095-124.
10. Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50:71-86.
11. Dormans JP, Rang M. The problem of monteggia fracturedislocations in children. Orthop Clin North Am 1990;21:251-6.
12. Beach PM, Hewson JS. Elbow dislocation with comminuted fracture of the proximal radial shaft. Thoughts on the mechanism. Am J Surg 1966;112:941-2.
13. Walker R, Tanner J. Fracture of the proximal shaft of the radius associated with posterior dislocation of the elbow. A case report and review of the literature. Clin Orthop 1982;168:35-7.
14. Barquet A. Posterior dislocation of the ulna at the elbow with associated fracture of the radial shaft. Injury 1984;15:390-2.
15. Shukur MH, Noor MA, Moses T. Ipsilateral fracture dislocation of the radial shaft head associated with elbow dislocation: Case report. J Trauma 1995;38:944-6.
16. Domingo A, Fernandez-Valencia JA, Saz L, Prat S, Arandes JM. Elbow dislocations associated with ipsilateral radial shaft fractures: A case report and review of the literature. J Trauma 2008;64:221-4.
17. Soon JC, Kumar VP, Satkunanartham K. Elbow dislocation with ipsilateral radial shaft fracture. Clin Orthop 1996;329:212-5.
18. Wong-Chung J, Jahromi I, Aradi AJ. Fracture of the upper radius with ipsilateral dislocations of the elbow and superior radio-ulnar joints. A case report. Int Orthop 1998;22:62-4.
19. Bucholz RW, Heckman JD, Court-Brown C, Rockwood CA, Green DP, editors. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
20. Linzel D, Ring D, Jupiter J. Diaphyseal fracture of the radius with dislocation of the proximal radioulnar joint. J Trauma 2008;64:503-6.
21. Shamian B, Capo JT. Isolated radial shaft fracture with unreducable posterior dislocation of the radial head and rupture of the lateral collateral ligament: A case report. J Clin Orthop Trauma 2012;3:126-9.
22. Jadaan M, Jain SK, Ahmed A, Khayyat G. Ipsilateral radial head dislocation and radial shaft fracture in a child-a case report. J Orthop Case Rep 2014;4:9-11.
23. Singh J, Kalia A, Dahuja A. Ipsilateral radial head dislocation and proximal one-third radial shaft fracture in an adult: A case report. Open Orthop J 2018;12:189‐95.
 |
 |
 |
 |
 |
| Dr. Deepankar Verma | Dr. Saurabh Kumar | Dr. Ish Kumar Dhammi | Dr. Rajnand Kumar | Dr. Rajat Kapoor |
| How to Cite This Article: Verma D, Kumar S, Dhammi IK, Kumar R, Kapoor R. Isolated Radial Shaft Fracture with Unreducable Posterior Dislocation of the Radial Head in Adult: A Case Report. Journal of Orthopaedic Case Reports 2020 August;10(5): 61-64. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 A Rare Case of Xanthogranulomatous Osteomyelitis of Radius Presenting as Pathological Fracture – A Case Report
April 1, 2025 A Rare Case of Xanthogranulomatous Osteomyelitis of Radius Presenting as Pathological Fracture – A Case Report January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report
January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report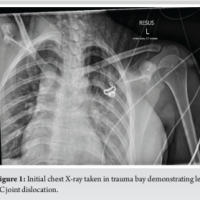 July 10, 2024 Management of Bilateral Posterior Sternoclavicular Joint Dislocation: A Case Report
July 10, 2024 Management of Bilateral Posterior Sternoclavicular Joint Dislocation: A Case Report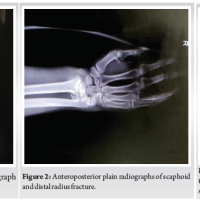 April 10, 2024 Terrible Triad of the Elbow with Ipsilateral Complete Triceps Tearing, Distal Radius and Scaphoid Waist Fracture: A Case Report
April 10, 2024 Terrible Triad of the Elbow with Ipsilateral Complete Triceps Tearing, Distal Radius and Scaphoid Waist Fracture: A Case Report


