
[box type=”bio”] Learning Point of the Article: [/box]
Although bilateral Monteggia is a rare presentation like any other fracture if treated early and anatomically reduced, it has a good prognosis as described in the case report.
Case Report | Volume 10 | Issue 6 | JOCR September 2020 | Page 76-79 | Kavin Khatri, Karan Rajpal, Jagdeep Singh. DOI: 10.13107/jocr.2020.v10.i06.1884
Authors: Kavin Khatri[1], Karan Rajpal[2], Jagdeep Singh[2]
[1]Department of Orthopaedics, All India Institute of Medical Sciences, Bathinda, Punjab. India.
[2]Department of Orthopaedics, Guru Gobind Singh Medical College, Faridkot, Punjab, India.
Address of Correspondence:
Dr. Karan Rajpal,
Department of Orthopaedics, Guru Gobind Singh Medical College, Faridkot, Punjab, India.
E-mail: krnrajpal@gmail.com
Abstract
Introduction: Giovanni Monteggia was the first to describe two cases of fractures of the proximal third of ulna with dislocation of the radial head. Monteggia fractures much more commonly are seen in children than in adults, but the bilateral entity is rare in both age groups. The following case is about the course of treatment for bilateral Monteggia fractures in a young male.
Case Report: A 35-year-old male came to the emergency with alleged history of roadside accident. Radiography showed bilateral Monteggia fracture type III (by the Bados classification). Surgical intervention was required with locking compression plates put on the both sides. Closed reduction of the radial head was done on both sides. The patient was given pop slabs for bilateral forearms for 21 days. After removing the splints, the function of the elbow was determined by the Broberg Morrey score which was on the right side 45 and on the left side 47 and 100 on both sides after 5 months of follow-up.
Conclusion: Surgical intervention and early rehabilitation are the most important and ideal line of treatment for the return of the good function of both elbows. Diagnosis, surgical technique, rehabilitation program, and clinical results are reported. The bilateral nature of the presentation does not affect the outcome of the fractures.
Keywords: Bilateral, forearm fractures, Monteggia fracture, radius dislocation.
Introduction
Fracture of the proximal ulna with dislocation of the radius is known by its eponym as Monteggia fracture. In 1814, Giovanni Battista Monteggia first described a lesion characterized by a fracture of ulnar diaphysis associated with anterior dislocation of the radial head [1]. The most common mechanism of injury for Monteggia fractures in children is a fall on outstretched hand in a pronated position [2]. In adults, the usual presentation of ulna fractures is either a transverse comminuted fracture or a fracture with butterfly fragment, both of which are usually seen as a result of either a direct blow with a stick while trying to protect oneself or by falling on an outstretched hand in a pronated position which is a bending force rather than torsion [1]. In this report, we present a case of a patient with bilateral Monteggia fractures type III. As far as we know, very few cases of bilateral Monteggia fracture have been described in literature. Monteggia fracture was classified by Badou (1976) into four types of fracture depending on the side of the subluxated radial head. The most common are type I, where there is anterior dislocation of the radial head and type II where there is posterior or posterior-external dislocation of the radial head, type III radial head is dislocated in lateral direction (which almost exclusively occurs in children, a rare occurrence in adults as in this case report [3]). Type IV is defined as a fracture of both bones of the forearm with dislocation of the radial head [3]. Jupiter further classified the posterior Monteggia lesion (Bado type II) depending on the location and type of the ulnar fracture as well as the pattern of radial head injury [4]. In type IIA, the fracture of the ulna involves the distal part of the olecranon and the coronoid process; in type IIB, the fracture involves the transition from metaphysis to diaphysis, distally to the coronoid process; in type IIC, a diaphyseal fracture is present; and in type IID, the fracture extends from the olecranon to the proximal half of the ulna. The appearance of AO plates and stable osteosynthesis marked the end of these fractures being treated conservatively and, at large, functional results after conservative treatment used to be very unsatisfactory [1, 5, 6, 7, 8]. Bilateral Monteggia fracture in adults is very rare. Kloen et al. [9] described a case with bilateral Monteggia fracture that had been treated surgically. Another case reported by Ristic et al. [1] described a case with bilateral Moteggia fracture which was also operated on, as in the patient that we presented.
Case Report
A 35-year-old male came to the emergency with alleged history of roadside accident. The patient was hit from behind from a speeding vehicle and with the impact patient was thrown onto the road with both outstretched hands planted firmly on the ground (to break the impact of fall) with varus stress on both elbows (Fig. 1). This usually produces ulna fracture with tension failure at radial side first and lateral radial head dislocation. There were no external wounds or any distal neurovascular deficit in both upper limbs. There was no history of loss of consciousness or any history of seizures or vomiting and the patient was brought to the emergency department. Here, the patient underwent radiographic imaging of both forearms with elbow with wrist anteroposterior and lateral views. Bilateral above elbow slabs given. X-rays showed proximal 1/3rd ulnar shafts with lateral radial head dislocation (Fig. 2a and b), which accounts for Bado classification typeIII Monteggia fracture bilaterally, which almost exclusively occurs in children, but a rare occurrence in adults as in this case report [3].  Workup for surgery was done and was taken to the OR, where the patient was placed in a supine position, skin preparation and draping was performed for both upper limbs. A posterior skin incision was first performed on the right forearm. An anatomical reduction was achieved, and open reduction and internal fixation of the bilateral ulna were done with posterior anatomical plates and closed repositioning of radial head was done bilaterally. Fluoroscopy was used to confirm appropriate articular reduction, position of the devices, and ulnohumeral joint reduction. The elbow appeared stable through full range of motion and wound closed in layers and suction drain out bilaterally. Postoperatively, bilateral above-elbow pop slabs were given. Post-operative X-rays were performed (Fig 3a, b, c, d). Drains were removed after 48 h; at that time, the patient started passive-assisted exercises and active motion and pop slabs reapplied. Alternate day dressings were done, and skin sutures removed on 21st post-operative day along with the slabs. The patient was advised physiotherapy. X-rays were performed at 1 month of follow-up (Fig. 4) and then again at 5 months of follow-up (Fig. 5) along with clinical pictures after 5 months of follow-up (Fig. 6a, b, c, d, e, f).
Workup for surgery was done and was taken to the OR, where the patient was placed in a supine position, skin preparation and draping was performed for both upper limbs. A posterior skin incision was first performed on the right forearm. An anatomical reduction was achieved, and open reduction and internal fixation of the bilateral ulna were done with posterior anatomical plates and closed repositioning of radial head was done bilaterally. Fluoroscopy was used to confirm appropriate articular reduction, position of the devices, and ulnohumeral joint reduction. The elbow appeared stable through full range of motion and wound closed in layers and suction drain out bilaterally. Postoperatively, bilateral above-elbow pop slabs were given. Post-operative X-rays were performed (Fig 3a, b, c, d). Drains were removed after 48 h; at that time, the patient started passive-assisted exercises and active motion and pop slabs reapplied. Alternate day dressings were done, and skin sutures removed on 21st post-operative day along with the slabs. The patient was advised physiotherapy. X-rays were performed at 1 month of follow-up (Fig. 4) and then again at 5 months of follow-up (Fig. 5) along with clinical pictures after 5 months of follow-up (Fig. 6a, b, c, d, e, f).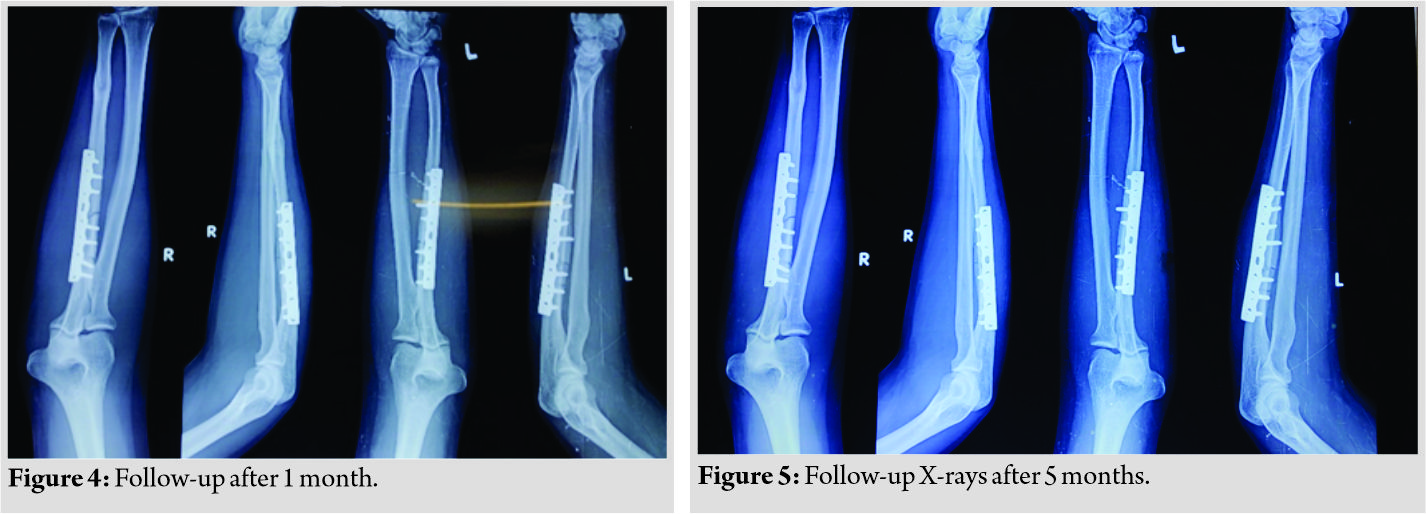
Discussion
Fractures involving the proximal end of the ulna with the dislocation of the radial head are serious injuries, and their correct management still poses a challenge to orthopaedicians. Monteggia fractures are produced by the direct force, most commonly a blunt force when a person tries to defend themselves. Evans EM proved that the cause of the fracture may be forced pronation and forearm during the fall by testing it on cadavers [10]. Roadside accidents are the leading cause of Monteggia fracture in the recent era. The presented patient, a 35–year-old male, came to the emergency with alleged history of roadside accident. The patient was hit from behind by a speeding vehicle and with the impact was thrown onto the road with both outstretched upper limbs (to break the impact of fall) with varus force on both elbows which lead to bilateral ulna fracture with tension failure at radial side first and lateral radial head dislocation, thus leading to bilateral type III Monteggia fractures. Until the appearance of AO plates and stable osteosynthesis, these fractures were treated non-operatively by plasters. Following the rule, this kind of treatment resulted in a very poor function of the elbow and led to a subsequent disability of the patient. The appearance of AO plate provides stable osteosynthesis of fractures and early mobilization of the elbow; as a result, the complications are significantly rare [6]. In addition to plate, Ring et al. announce the use of zuggurtung technique to achieve a satisfactory stability of fracture [11]. The patient was operated with bilateral small locking dynamic compression plates for ulna and closed repositioning of radial head was done. There were no complications during the treatment. Both fractures healed in the same period. Arenas et al. describe nerve lesions in Monteggia fracture primarily of the anterior interoseal nerve, with spontaneous remissions [12]. Ring et al. describe lesions of n. interossealis posterior, n. medianus, n. ulnaris, or both nerves, which are rare and occur in the open Monteggia fracture [11]. Konrad et al. described in their study the occurrence of non-healing fractures in six patients (out of 63) and heterotopic ossification in seven patients [13]. Korner et al. reported a revision of the surgery in 14 patients out of 68 as well as the appearance of osteoarthritis changes at the humeroradial and radioulnar joint [8]. In our study, we noted the appearance of the described complications. The function of both elbows was completely recovered – Broberg Morrey score for both right and left elbow was 100.
Conclusion
Bilateral Monteggia fracture in adults is very rare. Furthermore, type III Monteggia fracture (Bado’s classification) which almost exclusively occurs in children as said by Bado himself, but is a rare occurrence in adults as is emphasized through this case report. It requires anatomical repositioning of the ulna, its stable osteosynthesis, repositioning of the subluxated radial head, and early rehabilitation. This method of treatment allows complete recovery of elbow function.
Clinical Message
Although bilateral Monteggia is a rare presentation like any other fracture if treated early and anatomically reduced, it has a good prognosis as described in the case report above.
References
1. Bilateral Monteggia Fracture in Adults Obostrana Monteggia Fraktura kod Odraslih Dejan Ristić, Nebojša Jovanović, Voja Cvetković, Biljana Stanković, Branislav Vračević Clinical Hospital Center Zemun, Traumatology Center, Belgrade, Serbia.
2. Bojanić B, Stefanović Z Fractures and dislocation of the elbow joint. In: Banović D, editor. Traumatology of the Bone-joint System. Beograd: Zavod za Udžbenike i Nastavna Sredstva; 1998. p. 385-464.
3. Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50:71-86.
4. Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM. The posterior monteggia lesion. J Orthop Trauma 1991;5:395-402.
5. Andrew HC Jr. Fractures of shoulder girdle, arm, and forearm. In: Campbels CS, editor. Operative Orthopaedics. St. Louis: Mosby; 1998. p. 2281-362.
6. Perez ML, Lamas C, Martínez I, Pidemunt G, Mir X. Monteggia fractures in adults. Review of 54 cases. Chir Main 2002;21:293-7.
7. Babb A, Carlson WO. Monteggia fractures: Beware! S D J Med 2005;58:283-5.
8. Korner J, Hoffmann A, Rudig L, Müller LP, Hessmann M, Lill H, et al. Monteggia injuries in adults: Critical analysis of injury pattern, management, and results. Unfallchirurg 2004;107:1026-40.
9. Kloen P, Rubel IF, Farley TD, Weiland AJ, Helfet DL. Bilateral monteggia fractures. Am J Orthop 2003;32:98-100.
10. Evans EM. Pronation injuries of the forearm with special reference to the anterior Monteggia fracture. J Bone Joint Surg 1949;31B:578.
11. Ring D, Jupiter JB, Simpson NS. Monteggia fractures in adults. J Bone Joint Surg Am 1998;80:1733-44.
12. Arenas AJ, Artazcoz FJ, Tejero A, Arias C. Anterior interosseous nerve injury associated with a monteggia fracture-dislocation. Acta Orthop Belg 2001;67:77-80.
13. Konrad GG, Kundel K, Kreuz PC, Obrest M, Sudkamp NP. Monteggia fractures in adults: Long-term results and prognostic factors. J Bone Joint Surg Br 2007;89:354-60.
 |
 |
 |
| Dr. Kavin Khatri | Dr. Karan Rajpal | Dr. Jagdeep Singh |
| How to Cite This Article: Khatri K, Rajpal K, Singh J. Bilateral Monteggia Fracture: A Rare Case Presentation. Journal of Orthopaedic Case Reports 2020 September;10(6): 76-79. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2023 Atypical Monteggia Fracture Dislocation Type 3 Equivalent Lesion in a 4-Year-Old Boy
November 10, 2023 Atypical Monteggia Fracture Dislocation Type 3 Equivalent Lesion in a 4-Year-Old Boy June 1, 2025 A Rare Case of Bilateral Congenital Radial Head Dislocation: A Case Report
June 1, 2025 A Rare Case of Bilateral Congenital Radial Head Dislocation: A Case Report December 1, 2024 Bilateral Traumatic Rupture of the Quadriceps Tendon – A Case Report
December 1, 2024 Bilateral Traumatic Rupture of the Quadriceps Tendon – A Case Report December 1, 2024 Treatment and Rehabilitation of Complicated Fractures of Both Lower Limbs: A Case Report
December 1, 2024 Treatment and Rehabilitation of Complicated Fractures of Both Lower Limbs: A Case Report


