
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Isolated displaced intra-articular ulnar head fractures are rare entities, early diagnosis and prompt management are the key determinants for an excellent result.
Case Report | Volume 10 | Issue 7 | JOCR October 2020 | Page 68-71 | Sijal Rivi, Ravi Chauhan, Siddharth Agrawal, Brajesh Nandan, Manish Dhawan, Sumedh Kumar. DOI: 10.13107/jocr.2020.v10.i07.1922
Authors: Sijal Rivi[1], Ravi Chauhan[1], Siddharth Agrawal[1], Brajesh Nandan[1], Manish Dhawan[1], Sumedh Kumar[1]
[1]Department of Orthopaedic Surgery, Sir Gangaram Hospital, New Delhi. India.
Address of Correspondence:
Dr. Siddharth Agrawal,
Department of Orthopaedic Surgery, Sir Gangaram Hospital, New Delhi. India.
E-mail: dr.agrawal.siddharth@gmail.com
Abstract
Introduction: Although trauma involving distal radioulnar joint due to fall on the outstretched arm is a common injury pattern, Articular isolated fractures of distal ulna without coexistent radius fracture are extremely rare.
Case Report: We report on a 19-year-old male who presented at the trauma center after a fall from a two-wheeler with pain and swelling at his right forearm and wrist. After an inconspicuous X-ray in two planes, a computed tomography (CT) scan was performed and detected an isolated distal ulna fracture with an intact distal radioulnar joint. The patient was treated with closed reduction and K-wire fixation with a full functional range of motion attended at 10 weeks.
Conclusion: We recommend mandatory CT scan of the wrist, along with the early closed reduction, to get excellent results in such rare cases.
Keywords: Closed reduction, distal ulna, displaced, isolated, K-wires.
Introduction
The present work has been reported in line with the SCARE criteria [1]. Distal ulna is an important weight-bearing component of the wrist joint and an essential element of forearm articulation. Coordinated movements of both proximal and distal radioulnar joints are necessary for the proper pronation and supination of the forearm and injury to any of these can affect the rotational movements of the forearm [2]. Injuries with intra-articular gaps, shortening, or angulation of the ulna can destroy the integrity of the stable construct and the functional unit of the distal radioulnar joint and finally result in a lack of mobility [3]. The conditions that can involve distal radioulnar joint are Colles and Smith’s fracture, Galeazzi’s fracture dislocation, and Essex-lopresti injuries [4]. Distal ulna fractures generally occur in conjunction with fractures to the distal radius in 5–10%, excluding fractures of the ulnar styloid. Isolated intra-articular fractures of the distal ulna are extremely rare with an incidence rate of 74 in 100,000 persons per year with 92% of them having a concomitant distal radius injury and isolated distal ulna head (Q4) type being only 1% of it [5, 6]. We are reporting this case due to its unique presentation and to stress on the management of such a rare variant. A comprehensive literature review was performed by searching the PubMed‐National Center for Biotechnology Information database, using the keywords “Intra-articular, distal ulna, and closed reduction.” The search yielded four case reports published before March 2020, and all these four included cases were included in our literature review (Table 1). To the best of our knowledge, we report a unique first known case in the English literature of a 20-year‐old man with isolated displaced intra-articular distal ulna fracture with an almost total loss of forearm rotation to be managed with closed reduction and K-wire fixation as well as first reported case of isolated distal ulna in India and aim to discuss intra-articular distal ulna fracture in the light of clinical, radiological, and surgical data.
Case Report
A 19-year-old male presented with an alleged history of fall from the bike. He sustained an injury to his right wrist, followed by pain and swelling over the ulnar aspect. The pain was acute in onset, non-radiating, aggravated on wrist movements, and relived on rest and medication. Tenderness was present around the ulnar styloid, forearm pronation and supination were painfully restricted. He was initially managed with below elbow slab elsewhere outside. Initially, we took a radiogram on in which the fracture fragment was not clearly visible (Fig. 1). 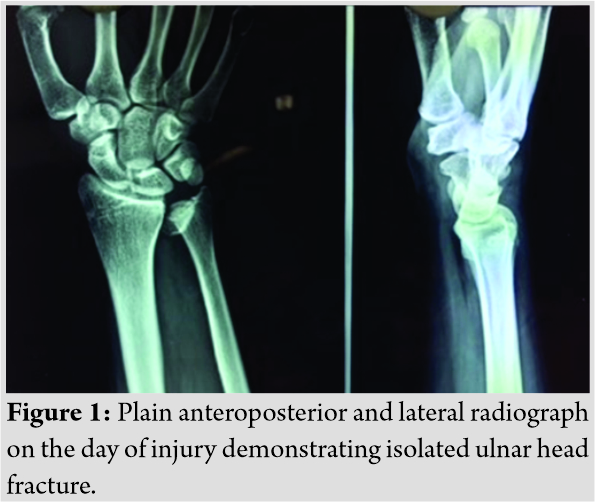 With respect to the clinical finding of a bony injury, an additional 3-D computerized tomography was done, on which there was an isolated intra-articular distal ulnar fracture with no disruption of distal radioulnar joint (Fig. 2). He was found to be having an isolated intra-articular distal ulna head fracture which was Q4 type according to AO Comprehensive classification [6].
With respect to the clinical finding of a bony injury, an additional 3-D computerized tomography was done, on which there was an isolated intra-articular distal ulnar fracture with no disruption of distal radioulnar joint (Fig. 2). He was found to be having an isolated intra-articular distal ulna head fracture which was Q4 type according to AO Comprehensive classification [6].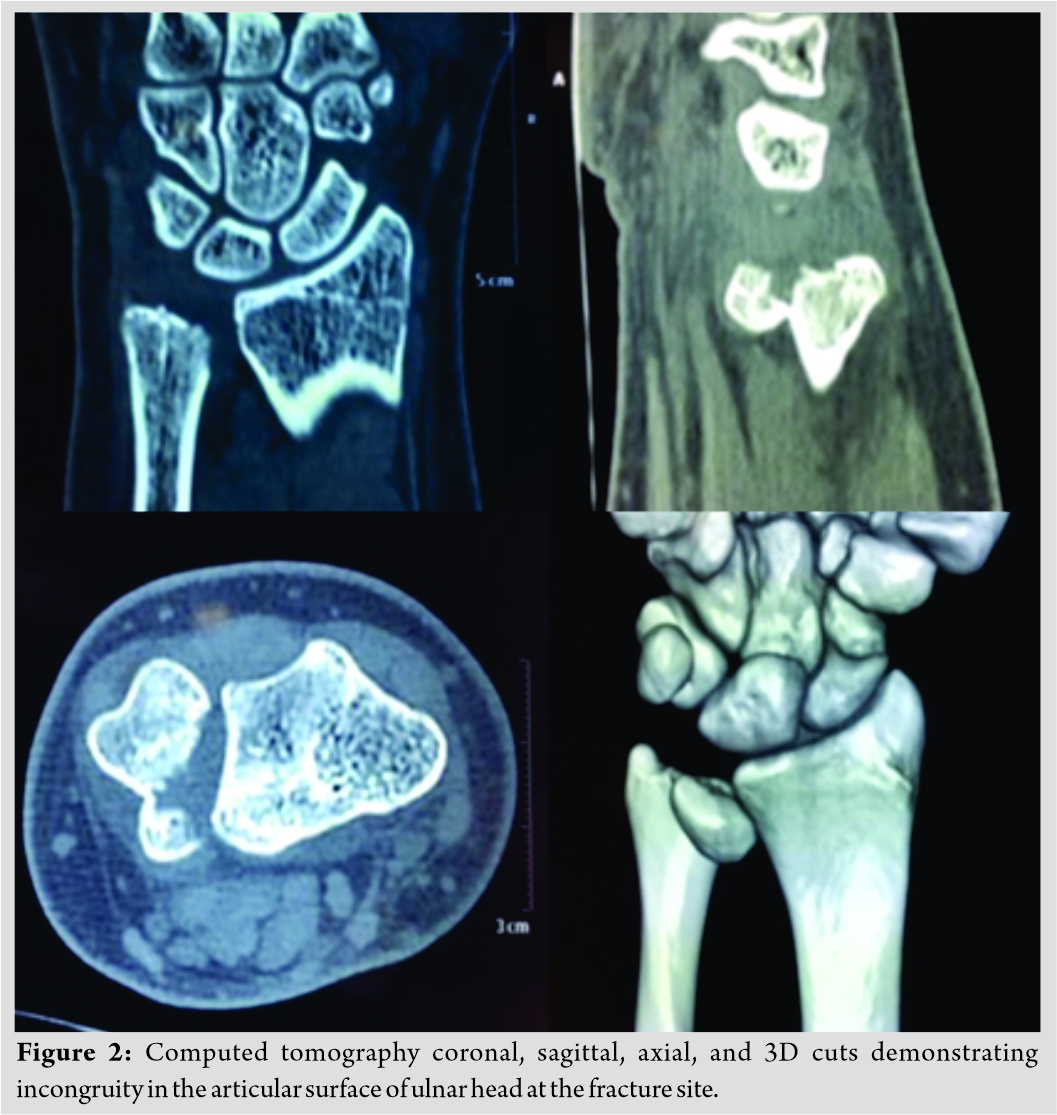
We managed it with closed reduction and internal fixation with K-wire on an emergency basis under regional anesthesia and kept in an above elbow forearm brace (Fig. 3).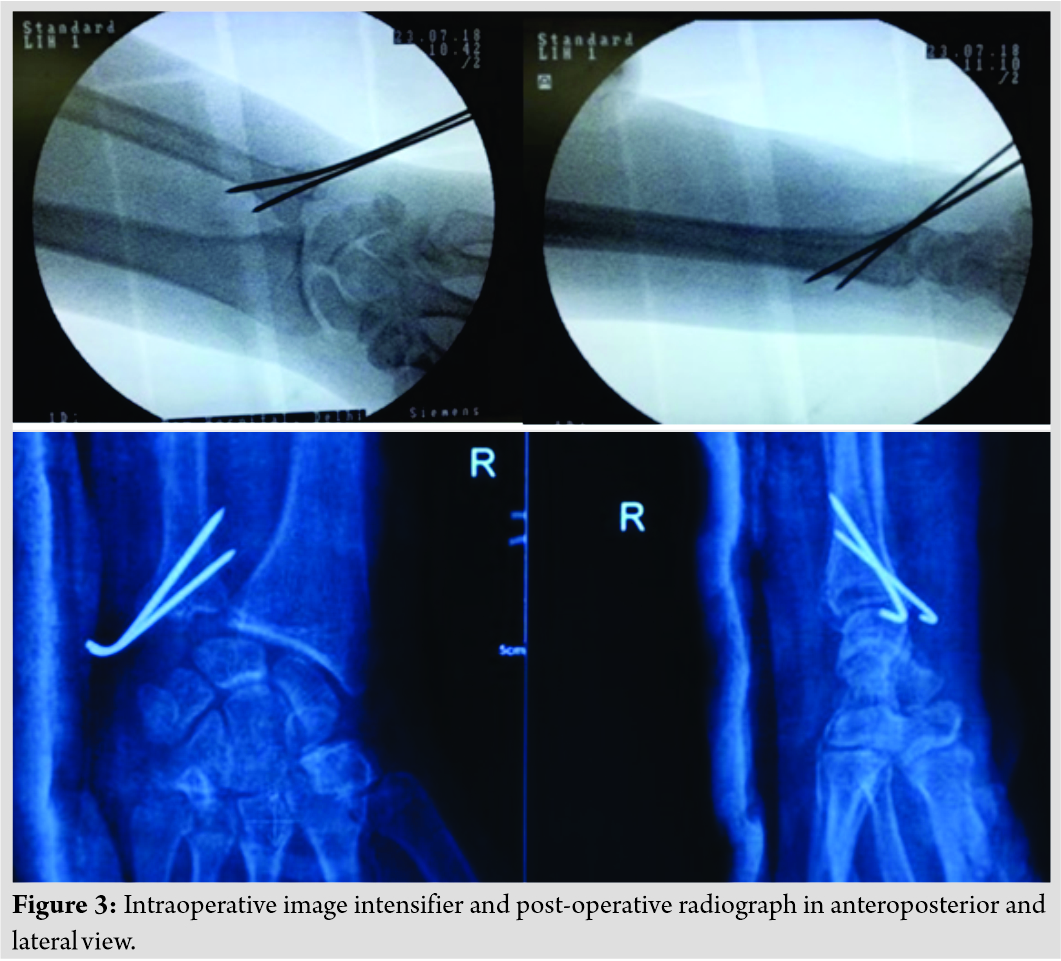 The procedure followed during reduction was sustained traction, and 1.8 mm K-wire was placed temporary and used as a simple joystick to reduce the fractured head part with and 2 K-wires of size 2.0 mm were inserted volarly under C-Arm guidance. In the follow-up at 4 weeks, K-wire was removed as an outpatient procedure and a below-elbow cast was given, and forearm rotation was started and brace was kept for further 2 weeks (Fig. 4).
The procedure followed during reduction was sustained traction, and 1.8 mm K-wire was placed temporary and used as a simple joystick to reduce the fractured head part with and 2 K-wires of size 2.0 mm were inserted volarly under C-Arm guidance. In the follow-up at 4 weeks, K-wire was removed as an outpatient procedure and a below-elbow cast was given, and forearm rotation was started and brace was kept for further 2 weeks (Fig. 4).  At 10 weeks, our patient had a painless good functional range of motion at the wrist joint with complete forearm pronation and supination (Fig. 5). As the triangular fibrocartilage complex load test and fovea ulnaris sign were negative and complete painless functional range of motion, additional MRI was needed to assess any other soft-tissue injury. No evidence of arthritis clinically or radiology was seen.
At 10 weeks, our patient had a painless good functional range of motion at the wrist joint with complete forearm pronation and supination (Fig. 5). As the triangular fibrocartilage complex load test and fovea ulnaris sign were negative and complete painless functional range of motion, additional MRI was needed to assess any other soft-tissue injury. No evidence of arthritis clinically or radiology was seen.
Discussion
As the above-mentioned review of the literature suggests that isolated intra-articular ulnar head fracture is rare, and to the best of our knowledge, this is first reported literature where closed reduction with K-wires was done in isolated fractures of ulnar head. From the patient’s mode of trauma and review of X-ray and CT scan results, the likely mechanism of injury was forced supination of the forearm, combined with a direct blow to the ulnar aspect of the wrist. “In full supination, the ulnar head is almost completely uncovered with contact occurring only at the volar aspect of the sigmoid notch” [7]. Therefore, a direct blow to the medial aspect of the wrist in full supination would generate collective shear and compressive loading and result in the fracture pattern seen here. In managing such fractures of distal radioulnar joint, open management is indicated when there is more than 2 mm step in the articular congruity when managed with a closed reduction which in our case, due to prompt and anticipated response, our patient was taken into the emergency procedure and a closed reduction was achieved as the trauma was fresh and was fixed with 2 K-wires for additional stability under image intensifier which ultimately led to early rehabilitation and functional improvement.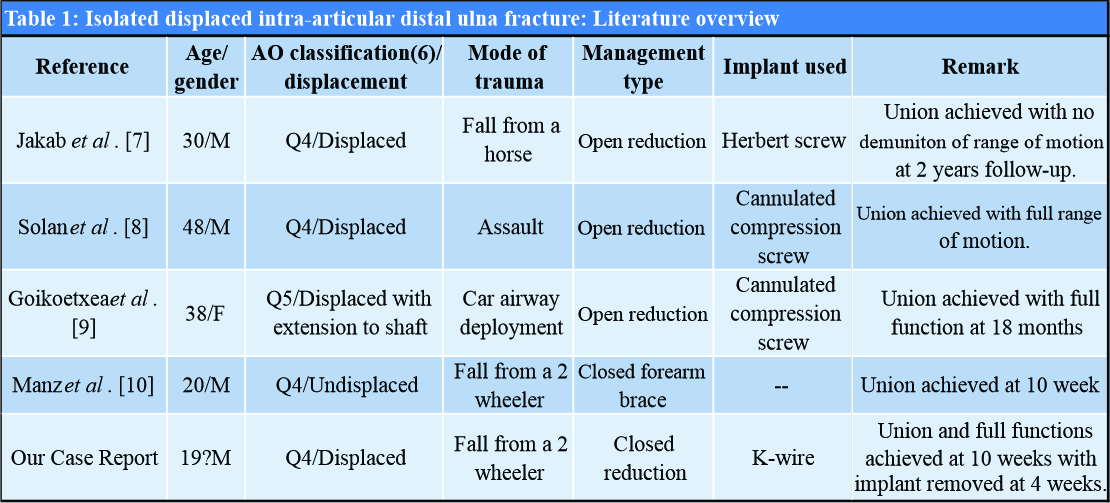
“The distal radioulnar joint is a complex anatomical structure. Its stability is important, both for the function of the wrist and for rotation of the radius about the ulna [8].” Fracture of the distal ulna is often associated with fracture of the distal radius, along with dislocation of the distal radioulnar joint, which was not the case here as there was no injury to the radius and there was no joint subluxation or dislocation at all, thus also making closed reduction possible. Only two cases of isolated displaced ulna fracture [7, 8] have been reported previously; in the other literature reviewed above, Goikoetxea et al. [9] had an ulnar head with shaft extension and Manz et al. [10] had an isolated undisplaced ulnar head fracture. Both Jakab et al. [7] and Solan et al. [8] treated the fracture with open reduction and screw fixation compared to us, we had a closed reduction and K-wire fixation, and thus, we had an early rehabilitation and full functional recovery at 10 weeks. Furthermore, closed reduction with K-wire meant the patient did not had to go another operative procedure for implant removal and lesser wound-related complication. Thus, this case of ours represents a newer method with a faster and less expensive method to treat such fractures, being the first to be reported. Furthermore, removing the implant early facilitates a better MRI if any associated soft-tissue injury needs to be ruled out due to persistent pain even after surgeries. Thus, we conclude that when managing such a rare entity basic principles should be applied, any positive physical finding should be investigated, and if the proper assessment is hindered, examination under local anesthesia should be performed. Injury to surrounding soft-tissue structures should also be ruled out with thorough clinical assessment. Intra-articular pathologies, a CT scan is a must as such injuries are often missed in initial radiographs which might lead to significant problems in forearm movement and wrist joint. Thus, if a displaced fragment is noted, that immediate reduction should be performed and stabilized. The distal radioulnar joint is a complex anatomical structure. Although closed reduction with internal fixation is a favourable option, we highly recommend open reduction and fixation if the fractured fragment is too small to hold it with a K-wire, or the fracture has communition or the fractured is old to get a proper reduction as anatomical reduction is of utmost importance to regain the favorable functional outcome. Its stability is important both for the function of the wrist and for rotation of the radius about the ulna. To allow normal rotation of the forearm, both proximal and distal radioulnar joints must be normal [4].
Conclusion
Isolated displaced intra-articular fractures of the distal ulna with intact distal radioulnar joint are rare. They should be properly assessed clinically and radiologically. CT scan should be done even if the initial radiograph is unobtrusive. They should be reduced and stabilized as early as possible to facilitate closed reduction to avoid unwanted alterations in forearm kinematics.
Clinical Message
Isolated displaced intra-articular ulnar head fractures are rare entities, early diagnosis and prompt management are the key determinants for an excellent result.
References
1. Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler AJ, Orgill DP. The scare 2018 statement: Updating consensus surgical case report (SCARE) guidelines. Int J Surg 2018;60:132-6.
2. Sinnatamby CS. Last’s Anatomy. 10th ed. Edinburgh: Churchill Livingstone; 1998.
3. Walz M, Kolbow B, Mollenhoff G. Fracture of the distal ulna accompanying fracture of the distal radius. Minimally invasive treatment with elastic stable intramedullary nailing (ESIN). Unfallchirurg 2006;109:1058-63.
4. Cooney WP, Linscheid RL, Dobyns JH. Fractures and dislocations of the wrist. In: Rockwood and Green’s Fractures in Adults. 4th ed. Philadelphia, PA: Lippincott-Raven; 1996.
5. Moloney M, Farnebo S, Adolfsson L. Incidence of distal ulna fractures in a Swedish county: 74/100,000 person-years, most of them treated non-operatively. Acta Orthop 2020;91:104-8.
6. Müller ME, Koch P, Nazarian S, Schatzker J. Radius/ulna=2. In: The Comprehensive Classification of Fractures of Long Bones. Berlin, Heidelberg: Springer; 1990.
7. Jakab E, Ganos DL, Gagnon S. Isolated intra-articular fracture of the ulnar head. J Orthop Trauma 1993;7:290-2.
8. Solan MC, Rees R, Molloy S, Proctor MT. Internal fixation after intra-articular fracture of the distal ulna. Bone Joint J 2003;85:279-80.
9. Goikoetxea X, Garmilla I, Etxebarria I, Careaga M. Isolated intra-articular fracture of the distal ulna: A rare injury related to airbag deployment. J Orthop Trauma 2006;20:292-4.
10. Manz MH, Jensen KO, Allemann F, Simmen HP, Rauer T. If there is smoke, there must be fire-isolated distal, non-displaced, intraarticular ulna fracture: A case report. Int J Surg Case Rep 2019;60:145-7.
 |
 |
 |
 |
 |
 |
| Dr. Sijal Rivi | Dr. Ravi Chauhan | Dr. Siddharth Agrawal | Dr. Brajesh Nandan | Dr. Manish Dhawan | Dr. Sumedh Kumar |
| How to Cite This Article: Rivi S, Chauhan R, Agrawal S, Nandan B, Dhawan M, Kumar S. Isolated Intra-articular Displaced Distal Ulna Injury: A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2020 October;10(7): 68-71. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


