
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Technique of partial acetabular resection and allograft reconstruction for a tumor involving posterior column of acetabulum is a unique learning point from this article.
Case Report | Volume 10 | Issue 9 | JOCR December 2020 | Page 33-37 | Tarun Goyal, Akriti Jain, Sajid Ansari, Souvik Paul, Michael Leonard Anthony. DOI: 10.13107/jocr.2020.v10.i09.1894
Authors: Tarun Goyal[1], Akriti Jain[2], Sajid Ansari[2], Souvik Paul[2], Michael Leonard Anthony[3]
[1]Department of Orthopaedics, All India Institute of Medical Sciences, Bathinda, Punjab, India.
[2]Department of Orthopaedics, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, Indi.
[3]Department of Pathology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
Address of Correspondence:
Dr. Tarun Goyal,
Department of Orthopaedics, All India Institute of Medical Sciences, Bathinda – 151 001, Punjab, India.
E-mail: goyal.tarun@gmail.com
Abstract
Introduction: The aim of this case report is to present an option of reconstruction in tumors involving the posterior wall and column of the acetabulum with sparing of the anterior column and the weight-bearing dome.
Case Report: We are reporting a case of a 25-year-old female with histopathologically proven synovial sarcoma involving the left inferior pubic ramus, ischium, and posterior wall of the acetabulum, along with a large soft-tissue extension in the posterior and medial thigh. Wide local excision involving partial acetabular resection and reconstruction using a femoral head allograft was carried out. The patient was allowed full weight-bearing mobilization after 6 weeks. At 3 months’ follow-up, the patient was able to walk without support and was able to do active straight leg raising. There were no radiological signs of joint degeneration at the 12-month follow-up.
Conclusion: Reconstruction with non-articular femoral head allograft can be a viable alternative after resection of tumor involving acetabulum. This procedure is expected to support the hip joint and restore function in the short term and recreate bone stock for future arthroplasty if the need arises.
Keywords: Synovial sarcoma, hemipelvectomy, pelvic sarcoma, acetabulum.
Introduction
Pelvic sarcomas are associated with poorer outcomes as compared to other skeletal sites. This may be attributed to the complex anatomy of pelvis and proximity to vital organs. Advances in chemotherapy and surgical reconstruction have improved the prognosis. However, the 5-year survival rate in localized cases remains between 50% and 60% [1]. Synovial sarcoma is a highly aggressive soft-tissue sarcoma occurring in the extremity of young adults, accounting for 6–9% of all adult soft-tissue sarcomas [2]. Synovial sarcoma of the pelvis is a rare entity with only a few cases reported in the literature [3, 4]. External hemipelvectomies are a highly mutilating surgeries. Limb salvage is the preferred surgical option whenever possible. Balancing goals of adequate margin control and biological reconstruction are a challenging task. Surgical resection aims at achieving 1–3 cm of tumor-free margins [5]. Reconstruction can be attempted with allografts or endoprosthesis [6, 7]. We are reporting a case of 25-year-old female with histopathologically proven synovial sarcoma involving left inferior pubic ramus, ischium, and posterior wall of the acetabulum, along with a large soft-tissue extension in the posterior and medial thigh. Wide local excision involving partial acetabular resection and reconstruction using a femoral head allograft was carried out.
Case Report
A 25-year-old female presented with complaints of pain over the left groin for 3 months and swelling over the left hip and proximal thigh for 2 months. She was unable to bear weight on the affected limb due to pain and deformity for a month. There were no constitutional symptoms. On examination, bulk of the swelling was in the medial and posterior aspects of the thigh, extending posterosuperiorly toward the ischial tuberosity. It was firm in consistency, had a multilobulated surface, and measured about 16×12 cm in dimensions. The left hip was fixed in 40° of flexion and 20° of adduction with no further movements possible. Pre-operative radiographs showed a lytic lesion involving the left inferior pubic ramus, ischiopubic ramus, posterior wall, and column of the acetabulum. There was soft-tissue involvement in the medial and posterior aspects of the proximal thigh (Fig. 1).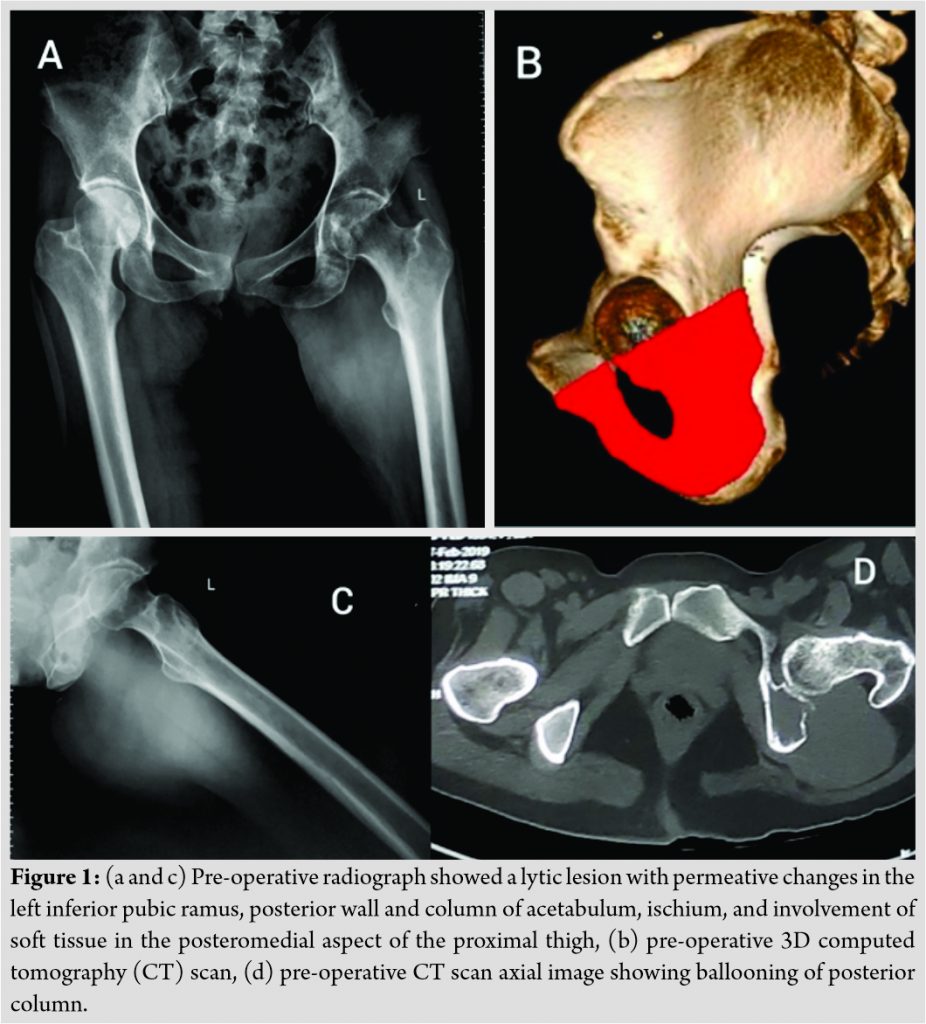
It had a permeative pattern of destruction. Magnetic resonance imaging revealed a large multilobulated, solid lesion in the muscle plane of adductor muscles and obturator externus, measuring 9.8 × 10 × 11.8 cm in size. It was T1W isointense and T2W hyperintense (Fig. 2).
The lesion extended into ischium, posteroinferior acetabulum, and inferior pubic ramus. The bone scan showed no other lesion in the body. The sciatic nerve and femoral neurovascular bundle were free of disease. The femur was spared from any infiltration. Pre-operative computed tomography with 3D reconstruction was also performed to plan surgical excision (Fig. 1). Core biopsy from the lesion revealed spindle cells highly immunoreactive to TLE-1 suggesting the diagnosis of synovial sarcoma (Fig. 3).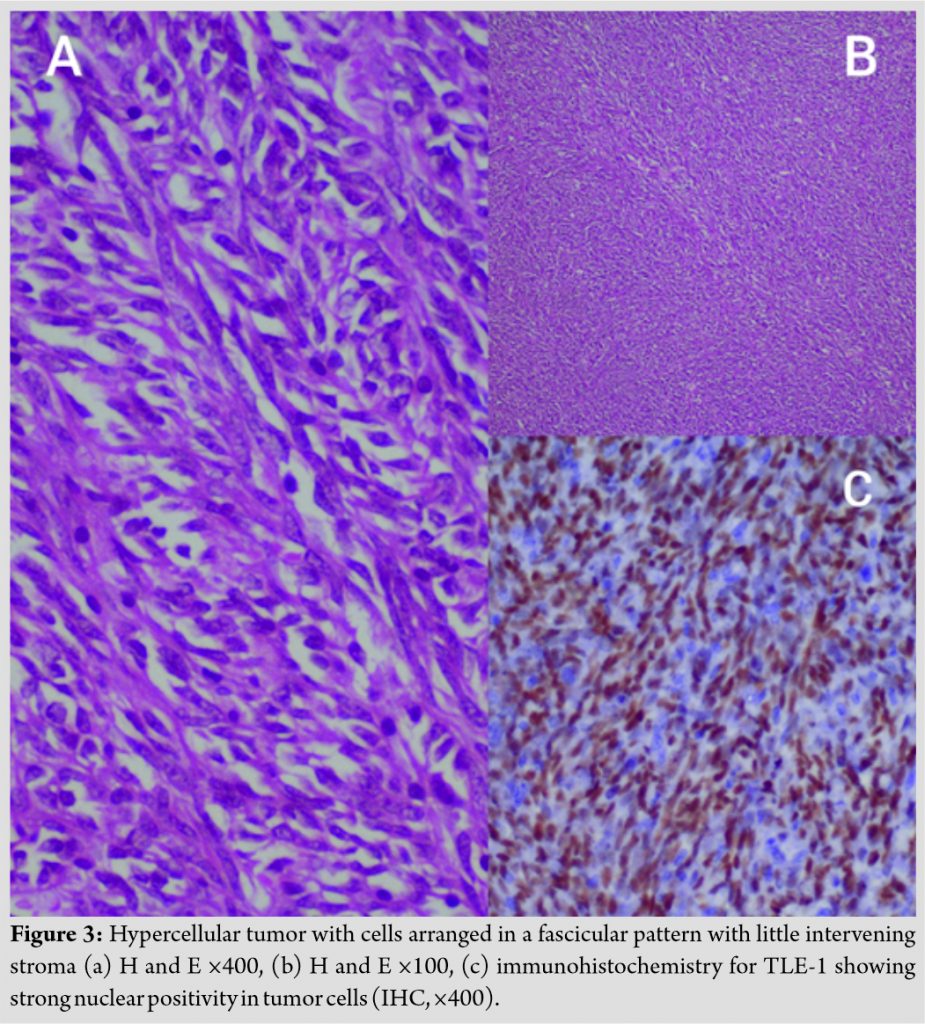
The diagnosis was further confirmed by a positive SYT translocation. Bone marrow biopsy revealed no infiltration by atypical cells. Pre-operative planning was done for wide local resection of the tumor (internal hemipelvectomy) and reconstruction of the acetabulum with allograft. The anterior wall and column of acetabulum were free of tumor extension. The weight-bearing dome was also free of tumor. Tumor only involved the ischium and posterior wall. Hence, a decision was made to take a 2 cm margin of tumor in the region of acetabulum and do a partial resection of acetabulum removing the inferior pubic rami, ischium, posterior wall, and column up to lateral wall of the greater sciatic notch along with inferior half of cotyloid fossa (Fig. 1). Exposure was achieved by a combined standard posterior approach and medial paralabial approach. The plane was developed between tumor and gluteus maximus posteriorly and adductor longus medially. Sciatic nerve was identified and protected while the obturator nerve and vessels entering the tumor mass were ligated. The short external rotators and posterior part of hip capsule were excised from femoral attachment for removal with the tumor. The hip joint was dislocated posteriorly to expose the acetabulum and complete acetabular resection. Adductor brevis and magnus muscles were detached distally and removed en bloc with the tumor. Hamstring muscles were also separated from the tumor mass proximally. The paralabial approach was used to separate inferior pubic ramus from superior pubic ramus, complete dissection of the adductor compartment and mobilize the tumor for removal after anterior and posterior cuts were complete. Intraoperative images are shown in (Fig. 4).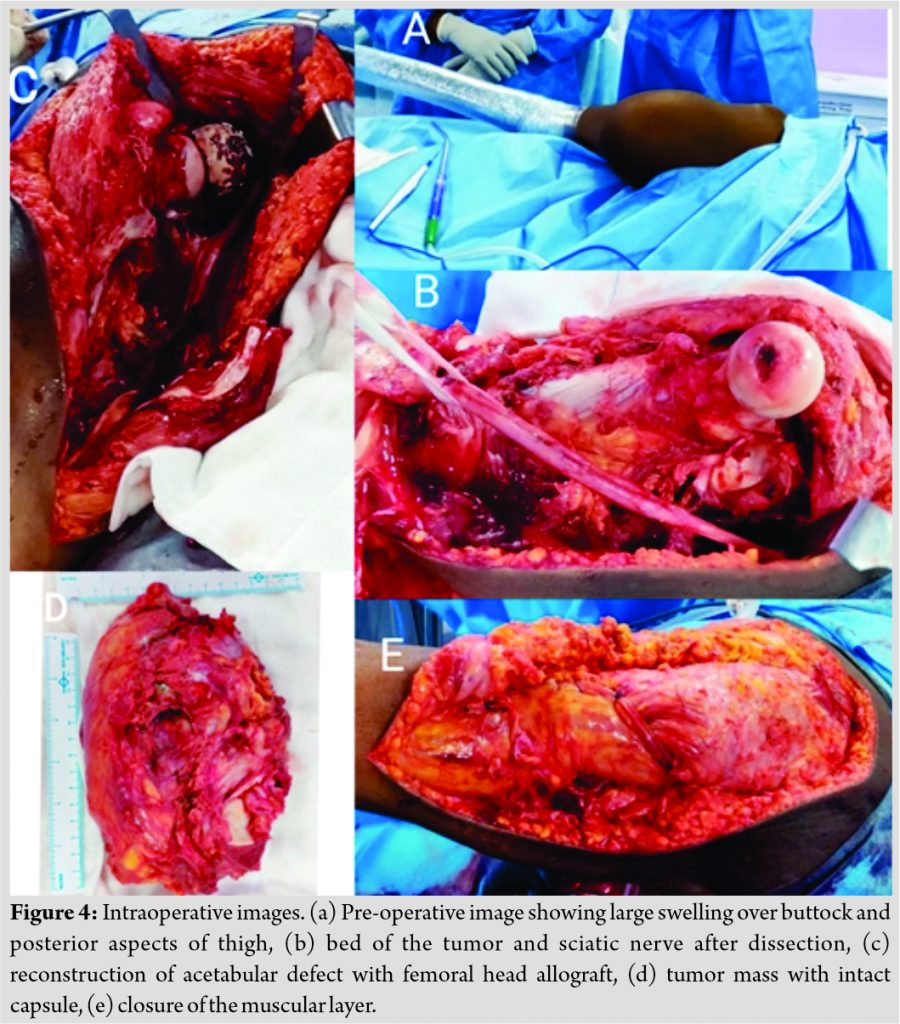
There was no breach found in the tumor capsule during excision. Intraoperative margins sent from five different medial and posterior sites for frozen section were free from tumor cells. Acetabular reconstruction was done with femoral head allograft, which was cut and reamed according to match the contour of remaining acetabulum. Femoral head was reduced and the allograft was fixed with three lag screws and a 5-hole recon plate used as a buttress plate. Blood loss was about 1600 ml and the duration of surgery was 130 min. Postoperatively, the histopathology report confirmed the diagnosis to be synovial sarcoma. The patient was allowed non-weight-bearing mobilization from the 1st day. The immediate post-operative period was uncomplicated except for seroma formation in the perineal region on the operated side, which was managed conservatively. The patient was allowed full weight-bearing mobilization after 6 weeks. At 3 months’ follow-up, the patient was able to walk without support and was able to do active straight leg raising (Fig. 5).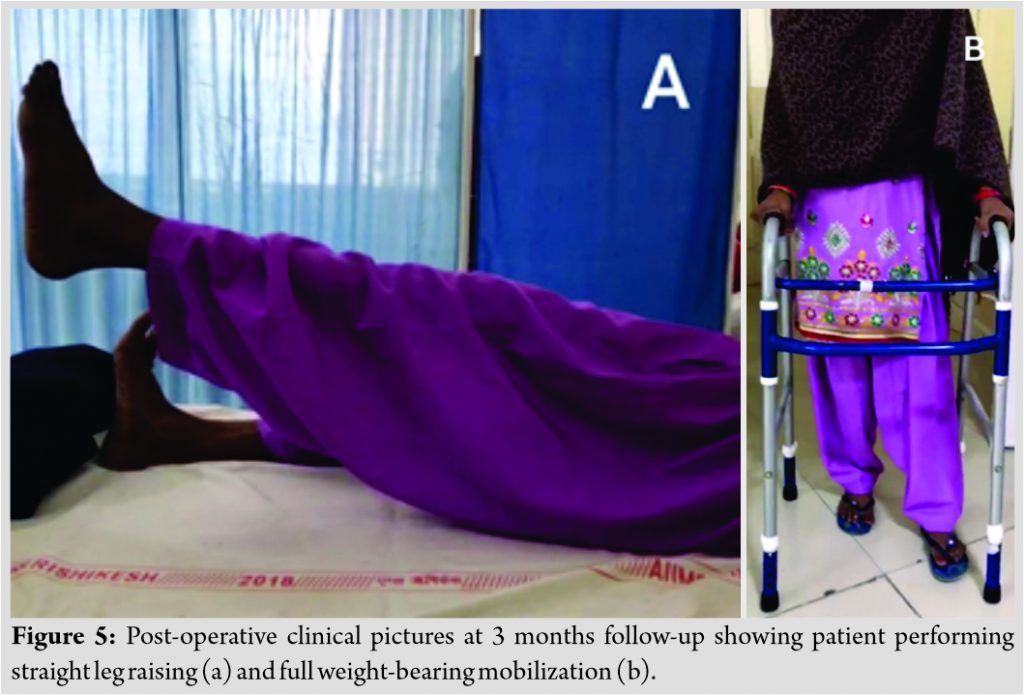
Post-operative radiographs and computed tomography revealed an optimum position of the graft with uptake of the graft with host bone (Fig. 6). The patient received 12 cycles of chemotherapy (VAC IE) and 60 Gy cumulative radiotherapy postoperatively.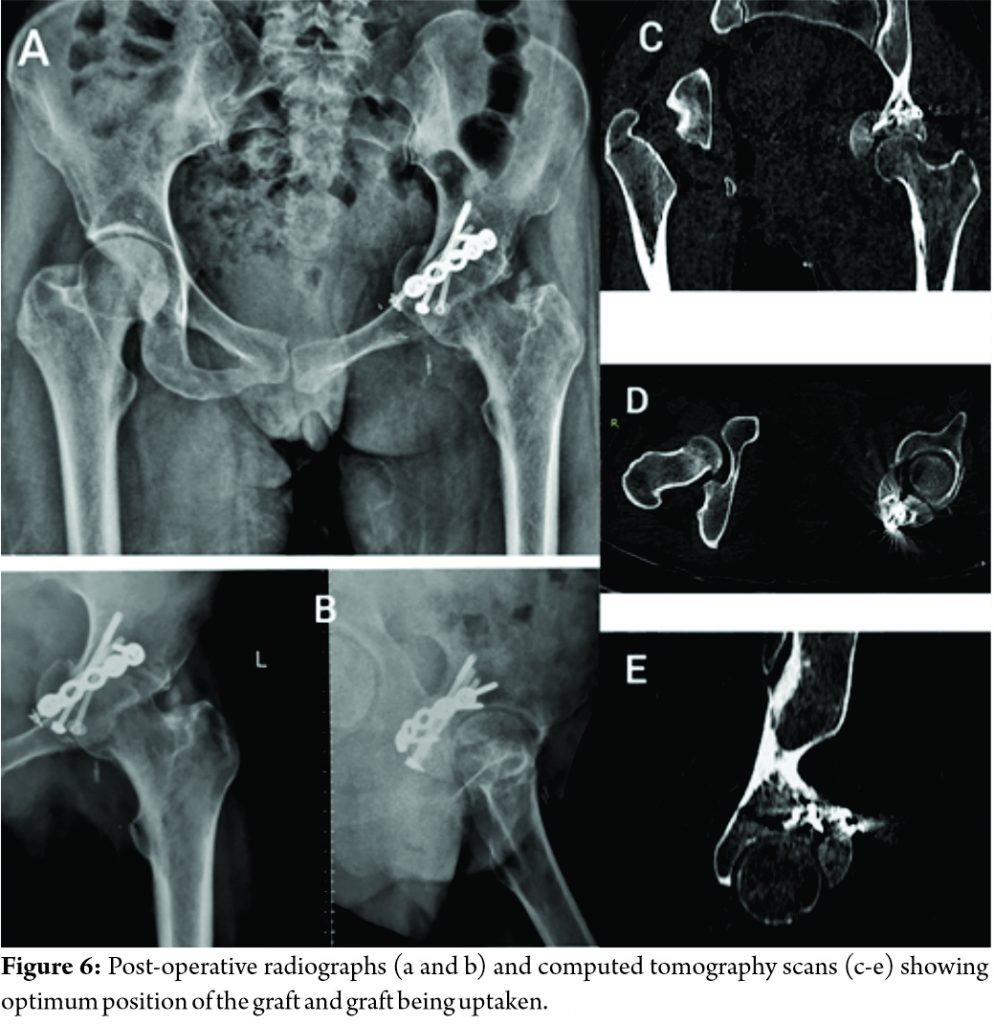
Discussion
Pelvic bone tumors present as a challenge to the surgeon due to variable involvement of pelvic bone and soft tissues and difficult resection. Pelvic reconstructions have to be individualized to the patient and type of resection. Advances in imaging and prosthetic designing have vastly improved reconstruction techniques. The aim of reconstruction in the pelvic ring or acetabular resection is to provide support to the salvaged limb and restore limb length. If acetabulum cannot be salvaged after resection, reconstruction becomes more complex. Iliofemoral and ischiofemoral arthrodesis provides satisfactory results in terms of durability but is often complicated by limb shortening, gait abnormality, and non-union [8]. Saddle prosthesis has been used as a reconstruction option in such cases and has the advantage of shorter operation time, earlier ambulation, and good limb length restoration. However, it has been associated with high complication rates (component migration, high hip center, and infection) and modest functional outcomes [9]. Another reconstruction technique using a pedestal cup provides better stability due to the more anatomical position of the implant but has a high risk of dislocation and prosthesis loosening [10]. Sun et al. [11] described five cases of sarcoma involving the posterior wall and column of the acetabulum. Resection of the posterior part of the acetabulum and ischium was carried out using posterior approach. Autologous femoral head graft was used for reconstruction of the defect fixing it to the remaining posterior column. Total hip arthroplasty was carried out primarily in these cases. Xiao et al. [12] described seven patients of giant cell tumor involving acetabulum. Partial excision of the acetabulum was carried out along with reconstruction using the autologous femoral head. Hip was reconstructed with total hip arthroplasty. Reconstruction of posterior wall of the acetabulum with a non-articular graft is not new. This technique has been described in comminuted fractures of posterior wall of the acetabulum. Sen et al. [13] used strut tricortical autograft from iliac crest for non-reconstructable fractures of posterior wall of the acetabulum in eight patients. 3.5 mm lag screws and buttress plates were used for the fixation of the fragment. After a mean follow-up of 3.34 years, no resorption of graft or conversion to total hip arthroplasty was seen. Reconstruction in acetabular defects requires a comprehensive appreciation of regional anatomy and bone defect. With the advancement in imaging and manufacturing technology, three-dimensional osseous models can be easily procured. In addition to visual reconstructions, 3-D printing creates life size models which have been used as an aid in templating and pre-operative decision-making. Rapid prototyping has also been applied for designing surgical tools such as patient-specific cutting guide as well as custom-made implantable prosthesis in pelvis [14]. With laser sintering and electron beam technologies, implants with complex designs with variable porous structures for minimizing shield stress, soft-tissue irritation, and promoting osteointegration [15]. Although published literature on 3D-printed acetabular components is limited to short-term clinical outcomes, it remains a potential viable option when considering pelvic and periacetabular reconstruction in limb salvage surgeries. Our patient had ischial and posteroinferior acetabular involvement, which left us with a good amount of native bone and articular surface post-resection. Bone in sciatic buttress was intact for fixation of the allograft. Cartilage was intact in the weight-bearing dome and anterior part of the acetabulum. The allograft could not provide cartilage in the region of articular surface of posterior wall. Thus, this reconstruction of the posterior acetabulum with femoral head allograft may result in hip joint arthritis in the long term. However, there were no radiological signs of arthritis at 12 months follow-up. No such procedure has been reported in the literature before. The procedure is expected to support the hip joint and restore function in the short term and recreate bone stock for future arthroplasty if the need arises.
Conclusion
Reconstruction with non-articular femoral head allograft can be a viable alternative after resection of tumor involving acetabulum. This procedure is expected to support the hip joint and restore function in the short term and recreate bone stock for future arthroplasty if the need arises.
Clinical Message
Maintaining the function of the hip joint is an essential but challenging part of pelvic tumors involving acetabulum. Reconstructions in these cases need to be individualized to the patient and type of resection. Allograft reconstruction may be an option with satisfactory short-term functional outcomes.
References
1. Synovial Sarcoma: Background, Pathophysiology, Etiology. Available from: https://www.emedicine.medscape.com/article/1257131-overview#a2. Accessed on 30 June 2019.
2. Eilber FC, Dry SM. Diagnosis and management of synovial sarcoma. J Surg Oncol 2008;97:314-20.
3. Hasan R, Kumar S, Rao L. Dumb-bell shaped poorly differentiated pelvic synovial sarcoma with molecular confirmation: A rare presentation of an uncommon disease entity. Indian J Pathol Microbiol 2013;56:396-8.
4. Rekhi B, Jambhekar N, Desai S, Basak R, Puri A, Agrawal M. A t(X; 18) SYT-SSX2 positive synovial sarcoma in the pelvis of a young adult male: A rare case report with review of literature. Indian J Cancer 2008;45:67-71.
5. Zagars GK, Ballo MT, Pisters PW, Pollock RE, Patel SR, Benjamin RS, et al. Prognostic factors for patients with localized soft-tissue sarcoma treated with conservation surgery and radiation therapy: An analysis of 1225 patients. Cancer 2003;97:2530-43.
6. Perry KI, Abdel MP, Lewallen DG, Rose PS, Sim FH. Innovative methods of reconstruction after pelvic tumor resection. Curr Surg Rep 2014;2:41.
7. Traub F, Andreou D, Niethard M, Tiedke C, Werner M, Tunn PU. Biological reconstruction following the resection of malignant bone tumors of the pelvis. Sarcoma 2013;2013:745360.
8. Fuchs B, O’Connor MI, Kaufman KR, Padgett DJ, Sim FH. Iliofemoral arthrodesis and pseudarthrosis: A long-term functional outcome evaluation. Clin Orthop Relat Res 2002;397:29-35.
9. Aljassir F, Beadel GP, Turcotte RE, Griffin AM, Bell RS, Wunder JS, et al. Outcome after pelvic sarcoma resection reconstructed with saddle prosthesis. Clin Orthop Relat Res 2005;438:36-41.
10. Dominkus M, Darwish E, Funovics P. Reconstruction of the pelvis after resection of malignant bone tumours in children and adolescents. Recent Results Cancer Res 2009;179:85-111.
11. Sun W, Zan P, Ma X, Hua Y, Shen J, Cai Z. Surgical resection and reconstructive techniques using autologous femoral head bone-grafting in treating partial acetabular defects arising from primary pelvic malignant tumors. BMC Cancer 2019;19:969.
12. Xiao C, Zhou Y, Zhang W, Luo Y, Tu C. An acetabular-preserving procedure for pelvic giant cell tumor involving partial acetabulum. World J Surg Oncol 2017;15:200.
13. Sen RK, Tripathy SK, Aggarwal S, Tamuk T. Posterior wall reconstruction using iliac crest strut graft in severely comminuted posterior acetabular wall fracture. Int Orthop 2011;35:1223-8.
14. Gouin F, Paul L, Odri GA, Cartiaux O. Computer-assisted planning and patient-specific instruments for bone tumor resection within the pelvis: A series of 11 patients. Sarcoma 2014;2014:842709.
15. Fang C, Cai H, Kuong E, Chui E, Siu YC, Ji T, et al. Surgical applications of three-dimensional printing in the pelvis and acetabulum: From models and tools to implants. Unfallchirurg 2019;122:278-85.
 |
 |
 |
 |
| Dr. Tarun Goyal | Dr. Akriti Jain | Dr. Souvik Paul | Dr. Michael Leonard Anthony |
| How to Cite This Article: Goyal T, Jain A, Ansari S, Paul S, Anthony ML. Intra-articular partial Acetabular Resection and Allograft Reconstruction for Synovial Sarcoma. Journal of Orthopaedic Case Reports 2020 December;10(9): 33-37. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


