
[box type=”bio”] What to Learn from this Article?[/box]
Cases presenting with severe pain and restriction of movements after arthroscopic procedure, first and foremost rule out any chances of infection followed by removal of any foreign bodies and thereafter proceed with aggressive treatment.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 6-8 | Mukesh Kumar, Jai Thilak DOI: 10.13107/jocr.2250-0685.404.
Authors: Mukesh Kumar[1], Jai Thilak[1]
[1] Department of Orthopedics, AIMS, Kochi, Kerala. India.
Address of Correspondence
Dr. Mukesh Kumar,
DNB Resident, Department of orthopedics, Amrita Institute if medical science & research centre,
Ponekkara p.o, Kochi, Kerala. India. Pin- 682 041.
E-mail: mukesh_medico@yahoo.co.in
Abstract
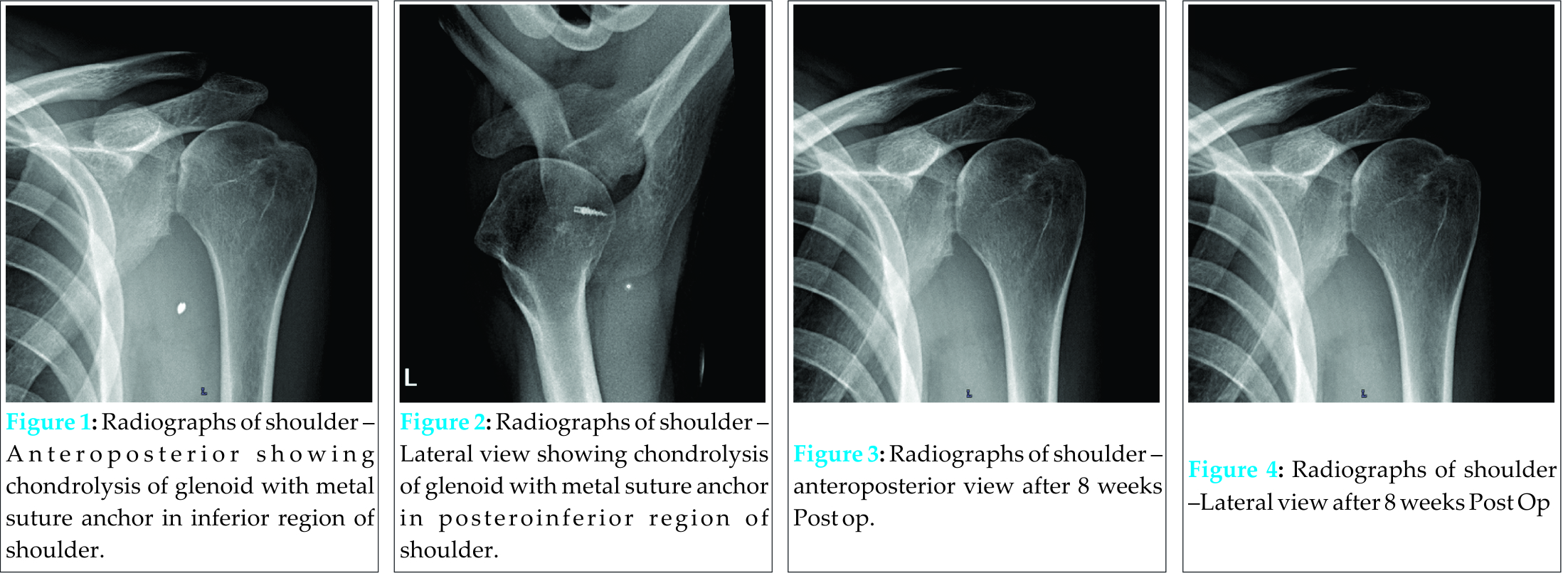
Introduction: The glenoid labrum is frequently torn in traumatic glenohumeral dislocation; arthroscopic repair is the standard method of treatment. The complications associated with this repair are pulling out of metal suture anchors, chondrolysis and joint infection. The infection of joint after arthroscopy is less than 1%. Staphylococcus is most common organism and rarely followed by Pseudomonas aeruginosa. We report a case of infected shoulder with chondrolysis of the joint and pulled out metal suture anchor lying inside the joint after Bankart’s repair.
Case Report: A 22-year-old gentleman came to us with complaints of shoulder joint pain & gross restriction of movements for one year, with history of intermittent fever and treatment in nearby hospital. He also gives past history of recurrent dislocation of shoulder with last episode 18 months back, which was diagnosed as Bankart’s lesion and arthroscopic Bankart’s repair was done 15 months back. He was evaluated at our institute and suspected to have infection of shoulder joint with pulled out metal suture anchor inside the joint. Arthroscopic removal of suture anchor and debridement of shoulder joint was done, Culture was obtained and culture specific antibiotics were given for six weeks, and significant improvement was observed with this line of treatment. At 1year follow up, the patient was able to perform his daily activities with terminal restriction of range of motion.
Conclusions: Shoulder joint infection is rare after Bankart’s repair and required a high degree of suspicion. Any foreign materials inside the joint should be taken out & followed with aggressive treatment by debridement, irrigation and culture specific antibiotics. Suppression of joint infection with antibiotics should be avoided specially when there is foreign body inside the joint.
Key words: Bankart’s repair, Septic Arthritis, Suture anchor, Pseudomonas aeruginosa.
Introduction
The glenoid labrum, a crucial stabilizer of the joint, is frequently torn from the anteriorglenoid in traumatic glenohumeral dislocation. This injury iscalled the Bankart’s lesion [1]. The most common surgical method of treatment is an arthroscopic Bankart’s repair, in which the torn labrum undergoes refixation to the anterior glenoid rim [2,3,4]. Chondrolysis is a devastating complication of arthroscopic shoulder surgery that can result in long term disabling consequences [5]. Severe articular damage caused by a loose or intra-articular metal suture anchor has been documented [8]. The incidence of shoulder joint infection after shoulder arthroscopy is less than 1% [9,10]. The most common organism isolated from septic joint after arthroscopy is Staphylococcus aureus & Propionibacterium acnes and rarely by Pseudomonas aeruginosa [11,12]. We report a case of shoulder joint infection with Pseudomonas aeruginosa with pulled out metal suture anchors lying inside the joint.
Case Report
A 22-year-old man presented with complaints of pain in the left shoulder since 1yr. Patient gives history of dislocation of the left shoulder while working out in the gym 2 years back and the second episode of dislocation occurred after 6 months while playing basketball. Following that incident he was evaluated, diagnosed to have Bankart’s lesion and Bankart’s repair was carried out in another hospital. Following the surgery, he was asymptomatic for 2 months. There was no swelling or discharge from the wound site and the wound healed well. He then had fever with pain and swelling in the left shoulder, following which he consulted an orthopedic surgeon. He was evaluated and started on antibiotics. Cefuroxime was started and continued for 5 months. Swelling reduced, pain remained as it was. On routine radiograph evaluation, it was found that the suture anchor had displaced so he was referred at our centre for further management. On examination, there were healed arthroscopic portal scars, crepitus felt on movements of the left shoulder, range of motion was globally restricted, there was wasting of deltoid & rotator cuff muscles. We arthroscopically debrided the shoulder joint & the suture anchor was removed which was freely lying in inferior aspect of shoulder joint. The washout was sent for culture which reported growth of Pseudomonas aeruginosa, and culture specific antibiotics were given for 6 weeks.
At 1year of follow up, the patient is able to carry out his daily activities without pain and terminal restriction of range of motion.
Discussion
The reported incidence of infections after shoulder scopy in some studies is 0.04% to 3.4% [7,11,12,13]. Most common organism isolated from septic joint after arthroscopy is Staph aureus & Propionibacterium acnes and rarely by pseudomonas aeruginosa [9,10]. Chondrolysis of the glenohumeral joint after arthroscopic surgery appears to be rare [14,15,16], high-volume intraarticular pain pumps, bioabsorbable labral fixation devices, and thermal probes may be considered as cause of chondrolysis but the actual cause of even the reported cases has not been confirmed, study[5] has suggested against the use of large doses of intra-articular placement of local anesthetics.
The glenohumeral arthrosis after arthroscopic Bankart repair is quite common but the symptoms are generally mild and comparable to nonoperative treatment [17]. The use of metallic suture anchors about the shoulder is common place and useful, but, as with other hardware used about the shoulder, there are significant risks if the anchors are improperly placed or if the index procedure fails [6]. Complications with metallic suture anchors are more common than plastic suture anchors [6]. As with any metallic or plastic implant, infection is a potential complication that must be considered before using suture anchors, as well as during the postoperative period. The exact cause for the infection in this case was not determined, but a high index of suspicion is essential in making the diagnosis, particularly in the event of an indolent infection. Irrigation, debridement, and removal of the hardware, with wound closure addressing the soft tissues and postoperative administration of antibiotics, have resulted in a satisfactory short term result.
Conclusion
Shoulder joint infection is rare after Bankart’s repair, and a high degree of suspicion is needed if patient presents with pain in shoulder joint and fever. Diagnosis is to be confirmed & any foreign materials inside the joint should be taken out & followed with aggressive treatment by debridement, irrigation and culture specific antibiotics. Suppression of joint infection with antibiotics should be avoided specially when there is foreign body inside the joint.
Clinical Message
Joint Infection after shoulder arthroscopy is rare but high degree of susciption, early diagnosis and appropriate treatment is needed in this type of situation to prevent further and permanent damage to the joint.
References
1. Bankart AS, Cantab MC. Recurrent or habitual dislocation of the shoulder-joint. 1923. Clin Orthop Relat Res 1993:3-6.
2. Bankart AS. The pathology and treatment of recurrent dislocation of the shoulder joint. Br J Surg 1938;26:23-9. doi:10.1002/bjs.18002610104.
3. Freedman KB, Smith AP, Romeo AA, Cole BJ, Bach BR Jr. Open Bankart repair versus arthroscopic repair with transglenoid sutures or bioabsorbable tacks for recurrent anterior instability of the shoulder: a meta-analysis. Am J Sports Med 2004;32:1520-7.
4. Marquardt B, Witt KA, Liem D, Steinbeck J, Potzl W. Arthroscopic Bankart repair in traumatic anterior shoulder instability using a suture anchor technique. Arthroscopy 2006;22:931-6.
5. Bailie D S, , Ellenbecker T S. Severe chondrolysis after shoulder arthroscopy: A case series, J Shoulder Elbow Surg 2009;18: 742-747.
6. Kaar T K, Schenck R C Jr,Wirth M A, and Rockwood C A Jr. Complications of Metallic Suture Anchors in Shoulder Surgery: A Report of 8 Cases. Arthroscopy: The Journal of Arthroscopic and Related Surgery 2001;17(1):31-37.
7. Johnson L, Shneider DA, Austin MD et al. Two per cent glutaraldehyde: A disinfectant in arthroscopy and arthroscopic surgery. J Bone Joint Surg Br 1982;64:237-239.
8. McAllister DR, Parker RD, Cooper AE et al. Outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. Am J Sports Med 1999;27:562-570.
9. Babcock H M, Carroll C, Matava M, Paul L’Ecuyer, and Fraser V. Surgical Site Infections After Arthroscopy: Outbreak Investigation and Case Control Study. The Journal of Arthroscopic and Related Surgery 2003;19(2):172-18.
10. Wang B , Toye B, Desjardins M, Lapner P, Lee C. A 7-year retrospective review from 2005 to 2011 of Propionibacterium acnes shoulder infections in Ottawa, Ontario, Canada. Diagnostic Microbiology and Infectious Disease 2013;75:195-199.
| How to Cite This Article: Kumar M, Thilak J. Infected shoulder joint with loose Suture Anchor in the joint after Bankart’s Repair- A Case Report. Journal of Orthopaedic Case Reports 2016 April-June;6(2): 6-8. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-404-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


