
[box type=”bio”] What to Learn from this Article?[/box]
Early diagnosis and intervention reduces the intra articular damage which may vary from minor abrasions to ligamentous tears
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 13-15 | Shishir S.M, Abhay Harsh K, Kanagasabai.R, James J Gnanadoss. DOI: 10.13107/jocr.2250-0685.478
Authors: Shishir S.M[1], Abhay Harsh K[1], Kanagasabai.R[1], James J Gnanadoss[1]
[1]Department of Orthopaedics, Pondicherry Institute of Medical Sciences, Pondicherry-605014. India.
Address of Correspondence
Dr. Shishir SM,
Associate Professor, Department of Orthopaedics, Pondicherry Institute of Medical Sciences, Pondicherry-605014. India.
E-mail: shishir100@gmail.com
Abstract
Introduction: Various types of foreign bodies have been removed from the knee joint. We report an unusual case of partial anterior cruciate ligament (ACL) tear secondary to a glass foreign body in an adolescent knee joint.
Case Report: A 13-year-old boy presented with pain, swelling and deformity of the left knee since 4 days. X- Ray revealed a foreign body in the left knee joint. The glass foreign body remained in the subcutaneous tissue for few days and later migrated into the knee joint. Arthroscopy revealed partial tear in the ACL at the femoral attachment with about 10-20 % of fibres being involved. The glass piece was removed arthroscopically and the ACL fibres were trimmed.
Conclusion: Arthroscopic removal of foreign bodies from the knee is a very simple procedure and has the advantages of avoiding large incision, shorter stay in the hospital, faster recovery and reduced infection rates. Glass foreign bodies were previously implicated in cartilage damage and meniscal injuries but a foreign body resulting in ACL tear has not been reported in literature.
Keywords: Glass, Foreign body, knee arthroscopy, partial ACL tear.
Introduction
Intra-articular foreign bodies in the knee are rare presentations. They usually present with symptoms of recurrent pain and locking episodes of the knee. Various types of foreign bodies have been removed from the knee joint such as needle, glass, lead of pencil, mercury thermometer, blades, thorn, bullet, screws and sometimes arthroscopic instruments like tip of shaver [1-6]. We report an unusual case of partial anterior cruciate ligament (ACL) tear secondary to a glass foreign body in an adolescent knee joint.
Case Report
A 13-year-old boy presented with pain, swelling, deformity and inability to bear weight. He gave a history of a fall on glass pieces while playing 9 days ago. He was asymptomatic for the first 4 days after the fall. Later he developed pain and knee swelling. He was taken to a nearby hospital where X-rays of the knee were done; no abnormality was noticed and was prescribed analgesics.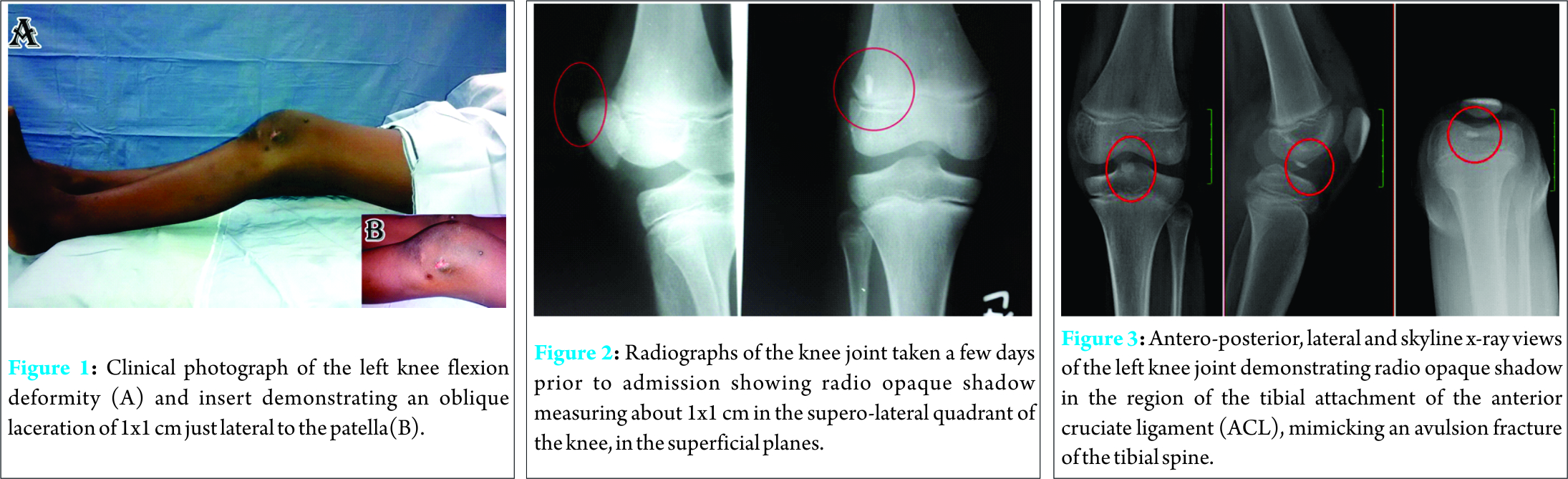
Symptoms worsened after 2 days when he developed deformity of knee and inability to bear weight on the affected side. He was then taken to a different hospital where he was diagnosed to have a foreign body in his knee and referred to our institution for further management. He gave no history of locking or giving away sensation. On examination, the left knee was in 30 degrees flexion, supra-patellar fullness and mild effusion was noted. An oblique skin laceration of 1×1 cm was noted lateral to the patella (Fig. 1). There was no active discharge from the wound or local raise of temperature. Tenderness was noted around the knee. The skin overlying the knee joint appeared normal. Boy was unable to move his knee due to pain and did not allow us to examine him thoroughly. Antero-posterior and lateral radiographs of the knee done 5 days prior to admission showed a radio-opaque shadow measuring about 1×1 cm in the supero-lateral quadrant of the knee, residing in the superficial planes, perhaps in the subcutaneous tissues (Fig. 2). This explains the child not having symptoms for the first 4 days. At the time of presentation to our out-patient department freshly taken radiographs revealed radio-opaque shadow in the inter-condylar region of the knee in front of the tibial attachment of the anterior cruciate ligament (ACL) resembling an avulsion of the ACL from the tibial plateau (Fig. 3). With the working diagnosis of foreign body in the knee, the boy was taken up for emergency arthroscopy. MRI scan of the knee was not considered as the history and follow-up events suggested a foreign body in the knee and this would not have changed our management plan. Under general anaesthesia, the knee deformity was spontaneously corrected suggesting that it may have been due to muscle spasm. Arthroscopy was carried out with the standard lateral and medial portals. About 50 ml of normal looking synovial fluid was drained out. We found a glass piece measuring 1 cm x 1 cm (Fig. 4) lying in the inter-condylar notch in the space between the ACL and the lateral surface of the medial femoral condyle. The glass piece was removed (Fig. 5) arthroscopically with the help of a small artery forceps by increasing the size of medial portal. The synovium in the supra-patellar pouch, medial and lateral gutter was hyperaemic. There was no obvious damage to menisci or the articular surfaces of the femoral or tibial condyles except for some abrasions (video 1). A partial tear in the ACL at the femoral attachment with 10-20 % of fibres being involved was noted probably due to the sharp edges of the glass piece (Fig. 6). The cut fibres were trimmed and examined under anaesthesia (Fig. 7, video 2). Anterior drawer, Lachman, Pivot shift and posterior drawer tests were all normal. Varus and valgus stress tests for collateral ligaments were normal. Hence, it was decided not to reconstruct the ACL. The chondral abrasions were smoothened out using a shaver. Joint was thoroughly washed and portals sutured. There was a small tear of 1×1 cm in the lateral retinaculum below the skin laceration, which was repaired. The skin laceration was debrided and sutured.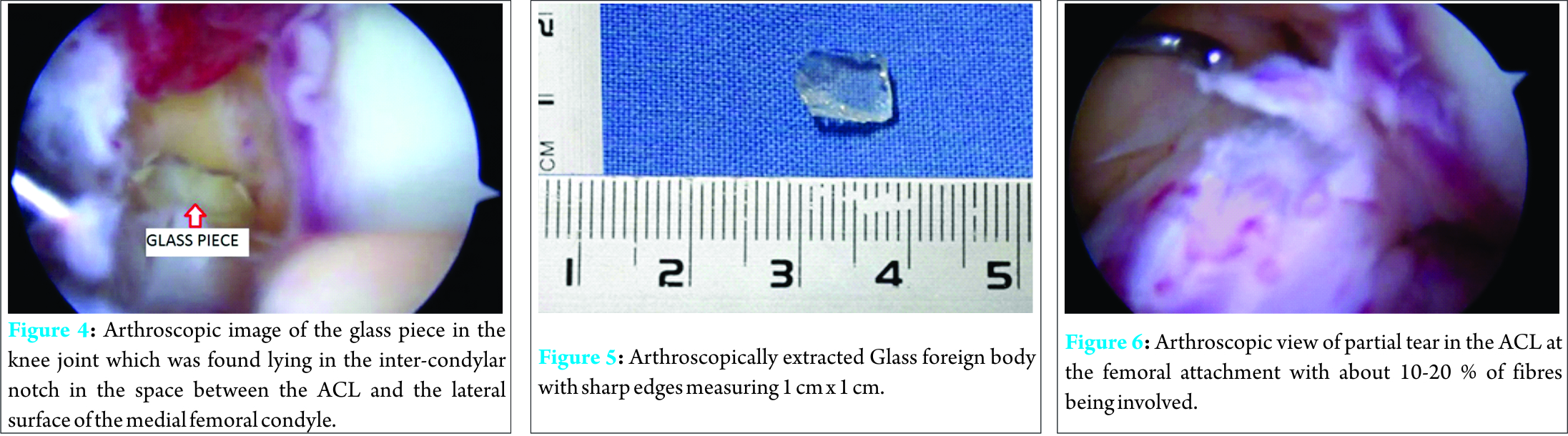
Wound healed subsequently without any infection. Post-operative radiographs revealed no foreign body in the knee. Post-operatively, the boy was allowed full weight-bearing and knee mobilisation exercises were started. No deformity was noted post-operatively. At the end of 1 year of follow-up, patient had full range of motion with no complaints of instability. He was involved actively in all sports activities. The parents were advised to review in case of any symptoms later.
Discussion
Penetrating injuries of the knee are relatively rare. Many of the times, penetrating wounds (i.e., after an accidental fall, road traffic accidents) remain the major cause of foreign body in the knee. Remaining injuries are sustained by missiles shot by machinery for civilian use (e.g., power-gun nails, needles, staples) or by weapons [1]. Rarely, the cause can be iatrogenic (e.g. arthroscopic instruments for e.g. tip of shaver blades, staples, suture materials, anchors, broken screws used for graft fixation) [2, 3]. Foreign bodies can be classified as radio-opaque and radiolucent. Metal, glass pieces, and lead objects are radio-opaque and can be identified on X-rays. Objects like thorns, stones, suture material, and bio-absorbable screws are radiolucent and can only be detected by an ultrasound or an MRI [4]. The presence of a local scar can give a clue to the underlying pathology, as in our case a glass piece had entered from the antero-lateral aspect of the knee joint. Whereas in some cases the cause of uncertain knee complaints especially in children can be due to foreign bodies which penetrated unnoticed into the joint cavity [4]. A foreign body in the knee joint is an absolute indication for operation [1]. Earlier the better, as the amount of intra-articular damage increases with time. A foreign body intruding the knee joint in childhood can go unnoticed initially and can cause symptoms for the first time in adult age [5]. Fragments can become adherent to the capsule or reside within synovial recesses or bursa without producing any symptoms for a very long time. Symptoms are usually caused by the foreign bodies which are mobile within the knee joint, resulting in meniscal damage or recurrent locking episodes [6]. In our case, the glass piece resided in the subcutaneous soft tissue for few days and later migrated into the knee joint to cause symptoms. Late migration of other foreign bodies like bullets, broken arthroscopy probe tips into the knee joint have been reported in literature [7, 8]. There is also a report of late migration of a glass piece of nearly 1.5 cm in size into the knee joint after remaining in the subcutaneous tissue for 7 years [9].
Conclusion
Arthroscopic removal of foreign bodies from the knee is a very simple procedure and has the advantages of avoiding large incision, shorter stay in the hospital, faster recovery and reduced infection rates. Glass foreign bodies were previously implicated in cartilage damage and meniscal injuries but a foreign body resulting in ACL tear has not been reported in literature.
Clinical Message
A foreign body in the knee joint is an absolute indication for emergency arthroscopic surgery.
| Video 1, Video 2 |
References
1. Carandell M, Roig D, BenascoC. Plant thorn synovitis. J Rheumatol 1980;7(4):567–569.
2. Palmers M, Dierickx C, Peene P, Bijnens E. An unusual metallic foreign body in the lateral tibio-femoral compartment. Arthroscopy 2002;8(3):325–328.
3. Kim SJ, Lee YT, Kim HJ. Arthroscopic extraction of a stainless steel foreign body imbedded in the tibial plateau. Arthroscopy 1998;14(1):103–105.
4. Muschol M, Drescher W, Petersen W, Hassenpflug J. Monoarthritis of the pediatric knee joint: differential diagnosis after a thorn injury. Arthroscopy 2004;20(8):865–868.
5. Schuz W, Mockwitz J. A foreign body in the knee joint—a very rare injury in children (in Germany). Unfallchirurgie 1987;13(1):45–47.
6. Haspl M, Bojanic I, Pecina M. Arthroscopic retrieval of metal foreign bodies from the knee joint after war wounds. Injury 1996;27(3):177–179.
7. Gutierrez V, Radice F. Late bullet migration into the knee joint. Arthroscopy 2003;19(3):E15.
8. Oztekin HH. An unusual complication of knee arthroscopy: an extra-articular migrated asymptomatic broken probe from the knee joint. Arch Orthop Trauma Surg. 2005;125(4):285–287.
9. Devgan A, Mudgal KC. An unusual case of foreign body knee that spontaneously migrated inside and out of the joint: arthroscopic removal. Knee Surg Sports Traumatol. Arthrosc. 2007;15(6):758–760.
| How to Cite This Article: Shishir S.M, Abhay Harsh K, Kanagasabai.R, James J Gnanadoss. An unusual case of partial Anterior Cruciate ligament (ACL) tear secondary to a glass foreign body in an adolescent knee joint. Journal of Orthopaedic Case Reports 2016 July-Aug;6(3):13-15. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-478-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


