
[box type=”bio”] What to Learn from this Article?[/box]
Tension band principle works well for transverse olecranon fractures even in the absence of radius.
Case Report | Volume 6 | Issue 4 | JOCR September-October 2016 | Page 66-68 | Ramanagouda Biradar, Arravind Pillai, Ullas Shetty. DOI: 10.13107/jocr.2250-0685.574
Authors: Ramanagouda Biradar[1], Arravind Pillai[1], Ullas Shetty[1]
[1]Department of Orthopaedics, BLDEU’s, Shri B. M. Patil Medical College, Vijayapur, Karnataka, India.
Address of Correspondence
Dr. Arravind Pillai,
Department of Orthopaedics, Shri B. M. Patil Medical College, Vijayapur – 586 103, Karnataka, India.
E-mail: pillai.arravind@gmail.com
Abstract
Introduction: Radial club hand is rare deformity, and many patients do not receive treatment due to lack of awareness. None of the treatment options available can restore normality. Fractures of the olecranon process in radial club hand are rare probably due to limited use of the limb.
Case Report: We report the case of a 35-year-old male with radial club hand who presented with a transverse fracture of the olecranon process. The patient underwent open reduction and tension band wiring for the fracture. At 6 months follow-up, the fracture had united and the patient had a complete functional recovery.
Conclusion: Tension band wiring is an excellent option for treating olecranon fractures in patients with radial club hand despite the deformity and the absence of radius.
Keywords: Olecranon process fracture, radial club hand, tension band wiring.
Introduction
Radial clubhand or Radial dysplasia (RD) is a deficiency along the preaxialor radial side of the extremity. Although the etiology of RD is not clear, several theories have been postulated as the cause of the disease, like maternal drug exposure, compression of the uterus and vascular injury, but the newer theory attributes it to a defect in the Apical Ectodermal Ridge1. Typical deformities include forearm shortening, radial deviation of the wrist and hypoplasia of the thumb2. Patients may also present with fixed extention deformities or absence of active motions which can cause severe disabilities. Various procedures have been mentioned, but surgery is aimed at comsmetic and functional improvement3. The Ulna also maybe deformed or bowed in RD, worsening the deformity. Fractures of the ulna in RD are rare. There are no guidelines for treatment of a deformed elbow and whether tension band wiring works in the absence of radius has not been studied. We present a case of RDof left limb who presented with a post traumatic fracture of the olecranon process which was successfully managed with tension band wiring.
Case Report
A 35 year old male patient presented with pain of acute onset of the left elbow following a fall. Examination revealed a short and atrophied forearm with a single bone and tenderness over the olecranon process. All movements at elbow and forearm were restricted.A provisional diagnosis of RD was made with a traumatic event. Plain radiography confirmed the diagnosis of RD with a displaced transverse olecranon fracture. The limb was immobilised with an above elbow splint and following routine investigations and pre anesthetic checkup, was posted for surgery under regional block.
Surgical Procedure:
The olecranon was approached posteriorly. The fracture was exposed and reduced with small reduction forceps. Using a 2 mm drill, a hole was drilled about 5 mm away from the posterior cortex of ulna,2 cm distal to the fracture site. A 20 gauge cerclage wire was passed through the hole to leave segments on either side of the holes. Two 2 mm k- wires were passed from the olecranon directed towards the anterior cortex .The cerclage wire was passed beneath the triceps tendon and the k- wires and tightened in a figure of eight configuration. The protruding ends of the k wires were cut before sinking them into the bone. Hardware position and reduction were confirmed under an image intensifier and fracture stability and movements were checked.
Post operatively, the limb was splinted with the elbow in flexion for 1 week and physical therapy was started as tolerated by the patient. During the 6 month follow up range of movement at elbow was 20- 130 degrees, which was comparable to the normal side.
Discussion
Club hand deformities may be classified as Radial and Ulnar. Radial club hand is more common with an incidence of 1:30,000 to 1:100,000 live births. 50% of cases are bilateral. About 40% of patients with unilateral club hand and 27% with bilateral club hand have associated with congenital anomalies involving cardiac, genitourinary, skeletal and hematopoietic system 2,4. The etiology of RD is unclear. Kumar and Sumar attributed the anomaly to a defect in Apical Ectodermal ridge1. They observed that removal of a portion of AER in chick embryos has produced anomalies which are similar to the radial club hand.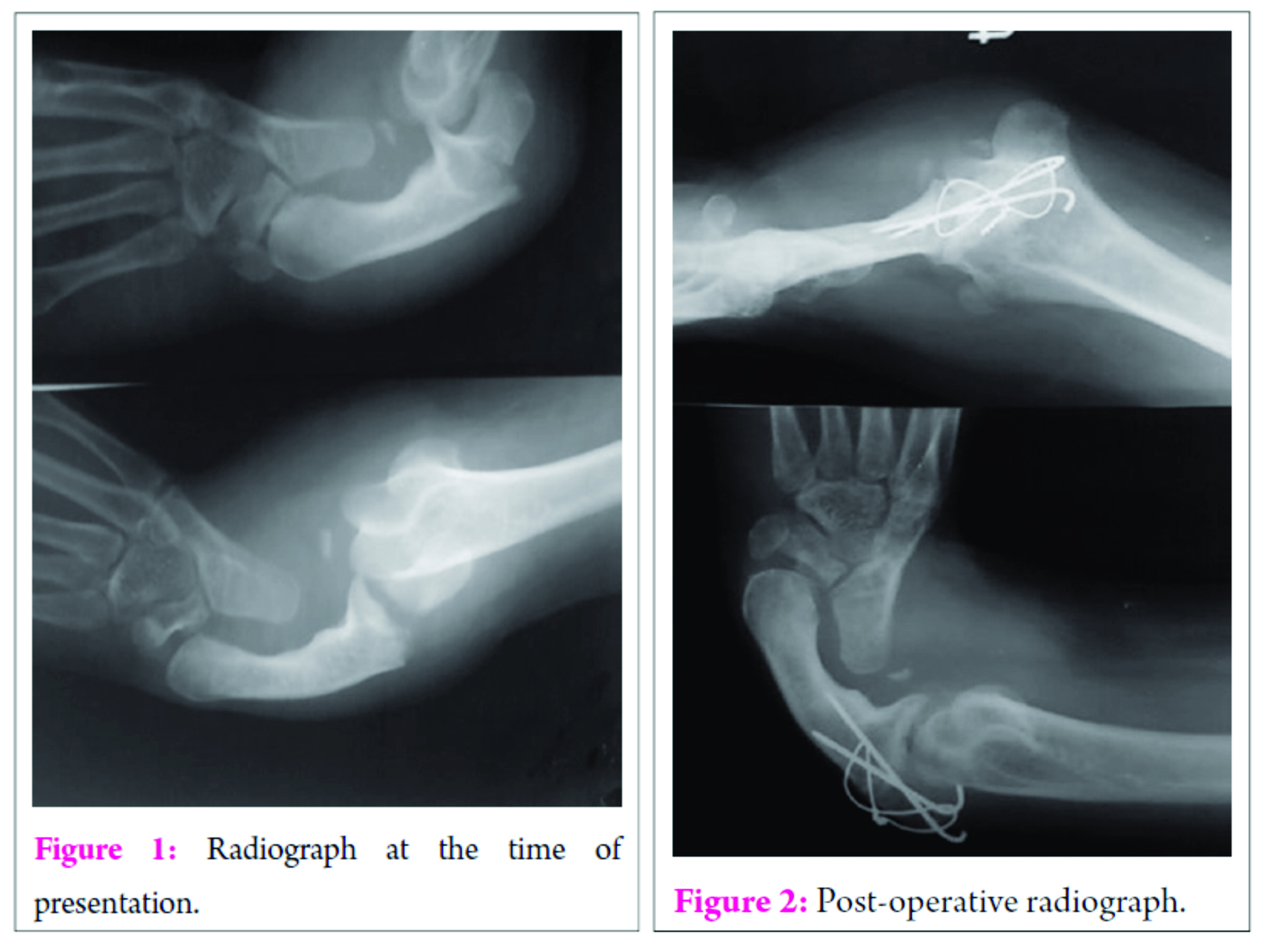
Clinical presentation of radial clubhand varies with the degree of radial deficiency and the presence of associated anomalies. Careful clinical examination is used to assess the degree of involvement.The deformity is usually noticed at birth. The neonate presents with a short forearm deviated radially with tight radial side soft tissue contractures. The thumb may be deficient to varying degrees. The fingers are stiff and elbow movements may also be restricted. In our case the patient had a type 3 RD, according to classification of congenital radial dysplasia is by Heikel5with partial absence of radius (Table 1). The function of the hand may be related to the amount of contractures, range of motion and power of the upper limb. Patients with reduced range of motion may use the whole limb in order to support or carry objects.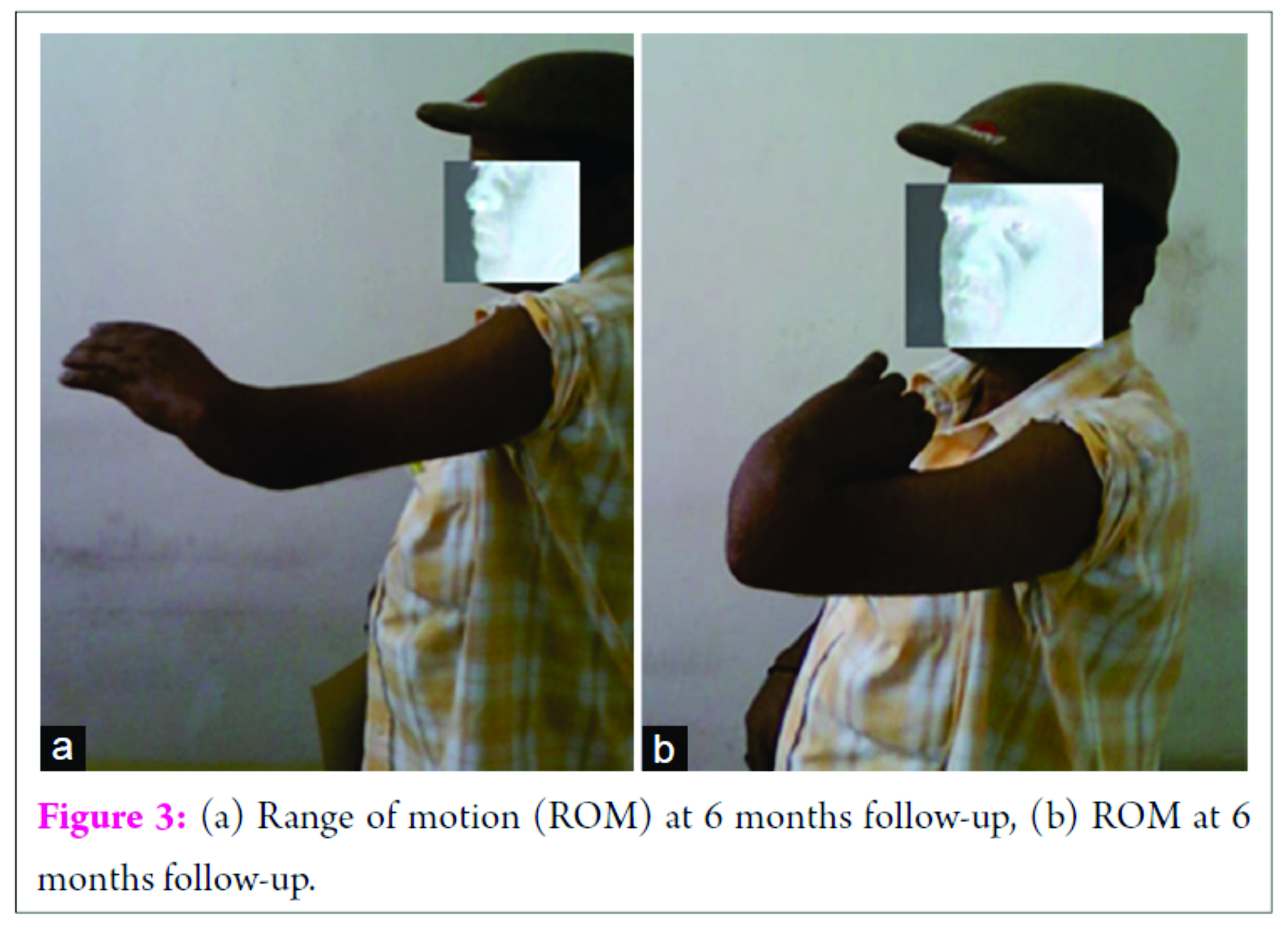
Treatment options
Surgical therapy is performed around the age of one year in these children. Centralization remains the principal procedure to realign the carpus onto the distal ulna and is indicated in types II, III, and IV radial deficiencies.In resistant cases and those presenting late, stretching the soft tissue with distracter techniques using illizarov or mini external fixator may be required 6,7. In our case the patient presented late and demanded treatment only for the fracture.
Tension band wiring was chosen as the treatment option after confirming with the patient about his functional range of movement before the fracture (20- 130 degrees), as the tension band wiring principle only exists during active extension in a range of 30-120° of flexion of the elbow8. Also, Post operatively, we were able to attain full range of motion which was comparable to the opposite side at6 month follow up. The tension band principle as applied to transverse olecranon fractures is based on the premise that distraction forces on the outer cortex of the ulna during elbow flexion are converted to compression forces on the articular surface of the olecranon at the fracture site. Hardware failure and secondary dislocations have been reported. Hardware failure was expected in this case due to the deformity and due to single bone articulating with the elbow, but we did not come across these complications. In our case tension band showed good results even when the bone in deformed and in the absence of the radius.
Conclusion
Neglected cases of RD are high due to lack of awareness and financial constraints. Olecranon fracture in a neglected case of RD is rare and can be managed well with tension band wiring with slight delay in exercise regimen.
Clinical message
Olecranon fractures in Radial club hand are not common. The deformity and absence of radius can increase the stress on the construct used for fixation during pronation and supination. Tension band wiring may be used in these cases with good outcome.
References
1. Kozin SH, Trumble TE. Congenital anomalies. Hand Surgery Update. Rosemont III: American Society for Surgery of the Hand; 2003. 599-624.
2. Salati SA, Rabah SM. Congenital isolated right radial club hand. Libyan Journal of Medicine 2010;5
3. Shariatzadeh H, Jafari D, Taheri H, Mazhar FN. Recurrence rate after radial club hand surgery in long term follow up. Journal of Research in Medical Sciences 2009; 14:179-186.
4. Lourie GM, Lins RE. Radial longitudinal deficiency. A review and update. Hand Clin. 1998;14(1):85–99.
5. Heikel HVA. Aplasia and hypoplasia of the radius. ActaOrthopScand 1988; 39 (Suppl) : 1
6. Kessler I. Centralisation of the radial club hand by gradual distraction. J Hand Surg 1989; 14 (B) : 37
7. Damore E, Kozin SH, Thoder JJ et al. The recurrence of deformity after surgical centralization for radial clubhand. J Hand Surg [Am]. 2000 Jul. 25(4):745-51.
8. Brink PR, Windolf M, de Boer P, Brianza S, Braunstein V, Schwieger K. Tension band wiring of the olecranon: is it really a dynamic principle of osteosynthesis? Injury. 2013 Apr;44(4):518-22
| How to Cite This Article: Biradar R, Pillai A, Shetty U. Olecranon Process Fracture in a Radial Club Hand Treated with Tension Band Wiring: A Case Report. Journal of Orthopaedic Case Reports 2016 Sep-Oct;6(4): 66-68. Available from: https://www.jocr.co.in/wp/2016/10/10/2250-0685-574-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


