
[box type=”bio”] What to Learn from this Article?[/box]
Meticulous clinical and radiological evaluation is essential in management of cervical spine osteochondromas.
Case Report | Volume 6 | Issue 5 | JOCR November-December 2016 | Page 89-91 | Vijay Shankar, Kumar Amerendra Singh, Simanchal P Mohanty. DOI: 10.13107/jocr.2250-0685.648
Authors: Vijay Shankar[1], Kumar Amerendra Singh[1], Simanchal P Mohanty[1]
[1]Department of Orthopaedics, Kasturba Medical College, Manipal, Karnataka, India.
Address of Correspondence:
Dr. Kumar Amerendra Singh,
Department of Orthopaedics, Kasturba Medical College, Manipal, Karnataka – 576 104, India.
E-mail: amerendra2@gmail.com
Abstract
Introduction: Cervical spine osteochondromas are rare tumors that usually involve the posterior spinal elements. Osteochondromas of the cervical spine presenting anteriorly as a mass over the supraclavicular region has not been reported in the literature.
Case Report: A 12-year-old boy presented with right sided supraclavicular swelling. Plain radiographs revealed a bony mass. Computerized tomography (CT) and magnetic resonance imaging scans of the cervical region showed a bony mass arising from pedicle and encroaching onto lamina of C6 vertebra. He underwent excision biopsy of the mass through an anterior approach. The histopathological diagnosis was osteochondroma. At 4-year follow-up, he was asymptomatic and CT scan revealed no recurrence.
Conclusion: Tumors arising from the posterior elements are difficult to diagnose by plain radiographs alone and require special imaging modalities to show their exact location, nature, and extent.
Keywords: Osteochondroma, supraclavicular, pedicle, anterior approach.
Introduction
Cervical spine osteochondromas are uncommon and mostly involve the posterior elements [1, 2, 3, 4]. Apart from a bony swelling they are mostly asymptomatic. However, rarely they can cause nerve root compression, compressive myelopathy, and sometimes pressure over the trachea or esophagus [5, 6]. To the best of our knowledge, osteochondromas of the cervical spine presenting anteriorly as a mass over the supraclavicular region has not been reported in literature. Careful examination along with advanced imaging is essential to arrive at a definitive diagnosis and plan appropriate management.
Case Report
A 12-year-old boy presented with complains of swelling over the right side of neck for last 1 year. The swelling was insidious in onset, gradually progressive, and painless. On clinical examination, a solitary 3 cm × 3 cm × 2 cm spherical bony hard swelling with well-defined margins was palpable in the right supraclavicular region (Fig. 1). The swelling was nontender and immobile. Neck movements were terminally restricted. Adson’s test was positive. Roos and Wright’s tests were negative. There was no distal neurovascular deficit.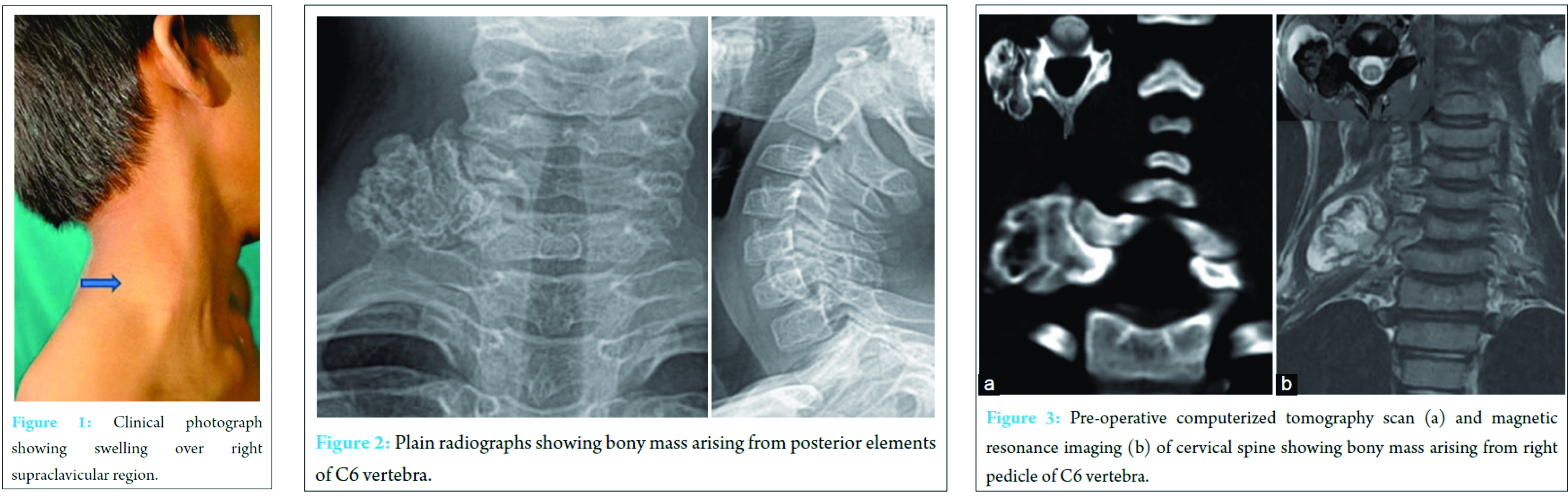
Plain radiographs of cervical spine revealed a bony mass over right side of neck (Fig. 2). Computerized tomographic (CT) scans showed a well-defined broad-based lobulated bony outgrowth measuring 2.8 cm × 2.4 cm arising from the right pedicle and encroaching onto lamina and transverse process of C6 vertebra. The cortex and medulla of the lesion was in continuity with the host bone (Fig. 3a). Magnetic resonance imaging (MRI) was done to evaluate the degree of soft tissue involvement. It revealed altered signal intensity of 11 mm thickness which was hyperintense on T2W and short tau inversion recovery (STIR) images. After gadolinium administration, there was peripheral enhancement surrounding the bony outgrowth which was suggestive of a cartilage cap. The scalene muscles showed no signs of infiltration; however, the roots and trunks of the brachial plexus were hyperintense on STIR which was suggestive of some compression (Fig. 3b).
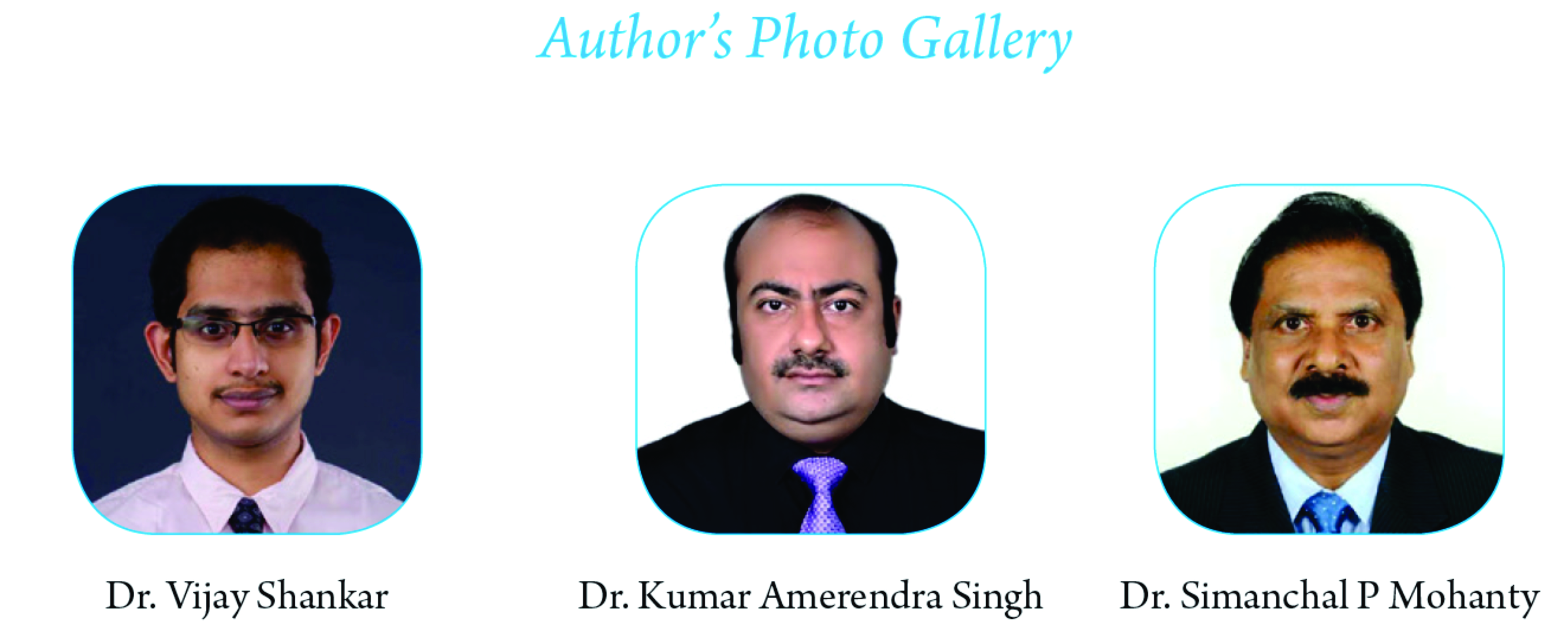
The bony swelling arising from the right pedicle and encroaching onto lamina and transverse process of C6 vertebra was excised extraperiosteally through an anterior spinal approach (Fig. 4).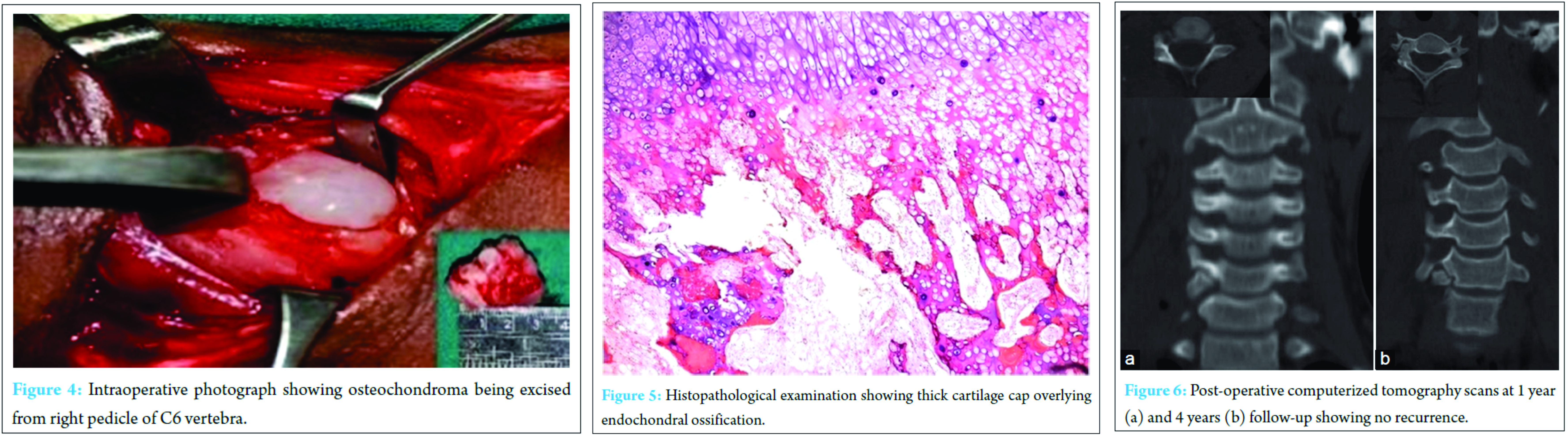
Histopathological examination showed thick cartilage cap overlying endochondral ossification and lamellar bony trabeculae encasing fatty and cellular marrow which was consistent with osteochondroma (Fig. 5). At 4-year follow-up, the patient was asymptomatic, and CT scan did not show recurrence (Fig. 6).
Discussion
Solitary osteochondromas of the spine are rare with an incidence of 1.3-4.1% [1, 2]. Cervical spine involvement is relatively more common with C2 vertebra most frequently affected [3]. It classically involves the posterior spinal elements especially the lamina and transverse processes [3, 4]. They are usually asymptomatic but can rarely cause compressive myelopathy, nerve root involvement or torticollis [5, 6, 7]. Cervical spine osteochondromas arising from the vertebral body can also cause dysphagia [8], sleep apnea [9], and hoarseness of voice [10]. They can present as a pharyngeal mass and even compress adjacent neurovascular structures like vertebral and carotid arteries [1, 11]. Osteochondromas arising from the spine are difficult to diagnose by plain radiography and clinical features alone [12].
Our patient presented with a painless mass in the supraclavicular region. Plain radiographs revealed a bony mass over the right side of neck. However, its exact origin was difficult to interpret. CT and MRI scans showed a bony mass arising from pedicle of C6 vertebra. To the best of our knowledge, an osteochondroma of the cervical spine involving posterior elements and presenting anteriorly in the supraclavicular region has not been reported in the literature.
Different approaches have been described in literature for excision of tumors arising from posterior elements [8]. In our case, we excised the mass through an anterior spinal approach even though it was arising from posterior elements of the spine. This is because of anterior extension of the mass. Careful surgical planning is essential for complete excision of the tumor and thereby prevents recurrence. Our patient was asymptomatic at 4-year follow-up without recurrence (Fig. 5).
Conclusion
Cervical spinal osteochondromas can present anteriorly as a supraclavivular swelling. Tumors arising from the posterior elements are difficult to diagnose by plain radiographs alone and require special imaging modalities to show their exact location, nature, and extent. Careful surgical planning in the form of choice of approach, knowing the size and origin of the lesion is required for safe and complete excision of the tumor.
Clinical message
Tumors arising from the posterior spinal elements usually require special imaging modalities like CT and MRI to better understand their exact location. This will aid in deciding the surgical approach. Osteochondroma can also present as a supraclavicular swelling.
References
1. Albrecht S, Crutchfield JS, SeGall GK. On spinal osteochondromas. J Neurosurg 1992;77(2):247-252.
2. Chooi YS, Siow YS, Chong CS. Cervical myelopathy caused by an exostosis of the posterior arch of C1. J Bone Joint Surg Br 2005;87(2):257-259.
3. Gille O, Pointillart V, Vital JM. Course of spinal solitary osteochondromas. Spine (Phila Pa 1976) 2005;30(1):E13-E19.
4. Gitelis S, Wilkins R, Conrad EU. Benign bone tumors. J Bone Joint Surg Am 1995;77(11):1756-1782.
5. Cherubino P, Benazzo F, Castelli C. Osteochondroma of the cervical spine. Ital J Orthop Traumatol 1991;17(1):131-134.
6. Cooke RS, Cumming WJ, Cowie RA. Osteochondroma of the cervical spine: case report and review of the literature. Br J Neurosurg 1994;8(3):359-363.
7. Akhaddar A, Boucetta M. Solitary osteochondroma of the cervical spine presenting as recurrent torticollis. Pan Afr Med J 2014;17:271.
8. Wong K, Bhagat S, Clibbon J, Rai AS. Globus symptoms: a rare case of giant osteochondroma of the axis treated with high cervical extrapharyngeal approach. Global Spine J 2013;3(2):115-118.
9. Wang V, Chou D. Anterior C1-2 osteochondroma presenting with dysphagia and sleep apnea. J Clin Neurosci 2009;16(4):581-582.
10. Certo F, Sciacca G, Caltabiano R, Albanese G, Borderi A, Albanese V, et al. Anterior, extracanalar, cervical spine osteochondroma associated with DISH: description of a very rare tumor causing bilateral vocal cord paralysis, laryngeal compression and dysphagia. Case report and review of the literature. Eur Rev Med Pharmacol Sci 2014;18 1 Suppl:34-40.
11. Nielsen OG, Gadegaard L, Fogh A. Osteochondroma of the cervical spine. J Laryngol Otol 1986;100(6):733-736.
12. Lotfinia I, Vahedi P, Tubbs RS, Ghavame M, Meshkini A. Neurological manifestations, imaging characteristics, and surgical outcome of intraspinal osteochondroma: Clinical article. J Neurosurg Spine 2010;12(5):474-489.
| How to Cite This Article: Shankar V, Singh KA, Mohanty SP. A Rare Presentation of Cervical Spine Osteochondroma. Journal of Orthopaedic Case Reports 2016 Nov-Dec;6(5):89-91. Available from: https://www.jocr.co.in/wp/2016/11/10/2250-0685-648-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


