
[box type=”bio”] Learning Points for this Article: [/box]
Clavicle fractures with intrapleural displacement resulting in pneumothorax should be managed operatively in order to achieve bony union as well as treat the pneumothorax.
Case Report | Volume 7 | Issue 4 | JOCR July – August 2017 | Page 17-20| Ryan D DeAngelis, Kenneth W Graf Jr, Rakesh P Mashru. DOI: 10.13107/jocr.2250-0685.830
Authors: Ryan D DeAngelis[1], Kenneth W Graf Jr[1], Rakesh P Mashru[1]
[1] Department of Orthopaedics, Cooper Medical School of Rowan University, 401 S. Broadway Camden, New Jersey 08103, United States of America.
Address of Correspondence
Dr. Ryan D DeAngelis,
Department of Orthopaedics,
Cooper Medical School of Rowan University, 401 S. Broadway, Camden, New Jersey 08103, United States of America.
E-mail: deangelir2@rowan.edu
Abstract
Introduction: Clavicle fractures are common injuries treated by orthopedic surgeons, with most injuries managed nonoperatively. Operative fixation of clavicle fractures is indicated in specific clinical scenarios such as open injuries, ipsilateral shoulder trauma, or fractures with associated neurovasculature compromise. Operative fixation is not widely accepted for closed injuries and is typically reserved for instances of failed closed treatment with resultant nonunion or delayed union. Among the complications associated with clavicle fractures, pneumothorax has not been commonly reported. We report a case of a severely displaced clavicle fracture requiring operative repair through plate fixation to achieve union of the fracture as well as resolve the pneumothorax.
Case Report: A 22-year-old intoxicated male with no past medical history was admitted to the trauma bay in stable condition after being involved in a motor vehicle accident. On the primary survey, the patient was noted to be tachypneic with decreased breath sounds over his right hemithorax. Radiographic studies of his chest demonstrated a right proximal third clavicle fracture with inferior displacement with associated partial pneumothorax; the patient was also noted to have a right femoral shaft fracture. Neurovascular examinations of his extremities were normal. A chest thoracostomy tube was inserted and placed under suction. Computerized tomography studies later revealed that the fractured clavicle had penetrated the pleura and caused the partial lung collapse. The patient was initially placed in a sling and underwent intramedullary nailing of his femur on the day of presentation. Given the severe displacement of his clavicle fracture into the lung tissue resulting in pneumothorax, there was significant concern for nonunion and lack of resolution of the pneumothorax. 2 days after stabilization of his right femur fracture, the patient underwent open reduction with internal fixation of his right clavicle. Follow-up radiographs showed a healed clavicle fracture and resolved pneumothorax.
Conclusion: Closed clavicle fractures typically heal uneventfully. Low energy, minimally displaced clavicle fractures can be managed nonoperatively, but high energy, significantly displaced injuries may require operative repair. Specifically, if these injuries result in pneumothorax, physicians shoulder consider operative repair for both treatment of the bony defect as well resulting pneumothorax.
Keywords: clavicle fracture, intrapleural penetration, open reduction internal fixation, pneumothorax.
Introduction
Fractures of the clavicle are common injuries treated by orthopedic surgeons. Various reports have established that clavicle fractures account for nearly 5% of musculoskeletal trauma and approximately 35% of shoulder fractures [1, 2, 3, 4]. Until recently, most clinicians have agreed to treat closed fractures nonoperatively with a sling or a figure-of-eight shoulder immobilizer for 4-6 weeks. Operative management of these injuries has been traditionally reserved for specific clinical scenarios including vascular or neurologic compromise, ipsilateral shoulder trauma, and open fracture [5, 6]. While open reduction and internal fixation of open clavicle fractures is generally accepted, this is not true of closed injuries. Despite the high union rates of closed treatment, there have been recent reports of success with operative management of closed clavicle fractures. Most of these series have been in individuals with clavicular nonunions and delayed unions [7, 8]. Among the various complications associated with clavicle fractures, pneumothorax has not been widely reported. There have been few reports in the literature of clavicle fractures complicated by pneumothoraces, but to the best of our knowledge, only one has been managed operatively [9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19]. None of these reports describe intrapleural invasion of the fracture fragment, and therefore, a chest thoracostomy tube was sufficient in the management of the lung collapse for significant pneumothoraces. The method of treatment for the clavicle fracture was either a sling or a figure-of-eight swathe. Steenvoorde et al. reported a case of an isolated clavicle fracture complicated by a pneumothorax in a person involved in a bicycle accident [13]. Both the clavicle fracture and pneumothorax were managed conservatively. Others have published their results with closed management of the clavicle fracture and a chest tube for the pneumothorax. We report a case of a closed proximal third clavicle fracture causing a pneumothorax from intrapleural penetration of the lateral fracture fragment treated with an open reduction and internal fixation to achieve both union of the fracture as well as resolve the pneumothorax. The displacement of the lateral segment prompted the insertion of a chest thoracostomy tube.
Case Report
A 22-year-old intoxicated male without any medical comorbidity was involved in a motor vehicle accident when he lost control of his automobile in a residential area and ultimately collided into a house. The patient was unrestrained and did not lose consciousness in the accident. Emergency medical personnel at the scene did report the deployment of the airbags with the patient displaying a Glasgow Coma Scale score of 15. He was emergently brought to the trauma center in stable condition. His primary survey revealed diminished breath sounds over his right hemithorax in conjunction with an increased respiratory rate. On further examination, he did appear to have crepitus over his right clavicle and gross deformity in his right thigh. Neurologic and vascular examinations of his extremities were normal.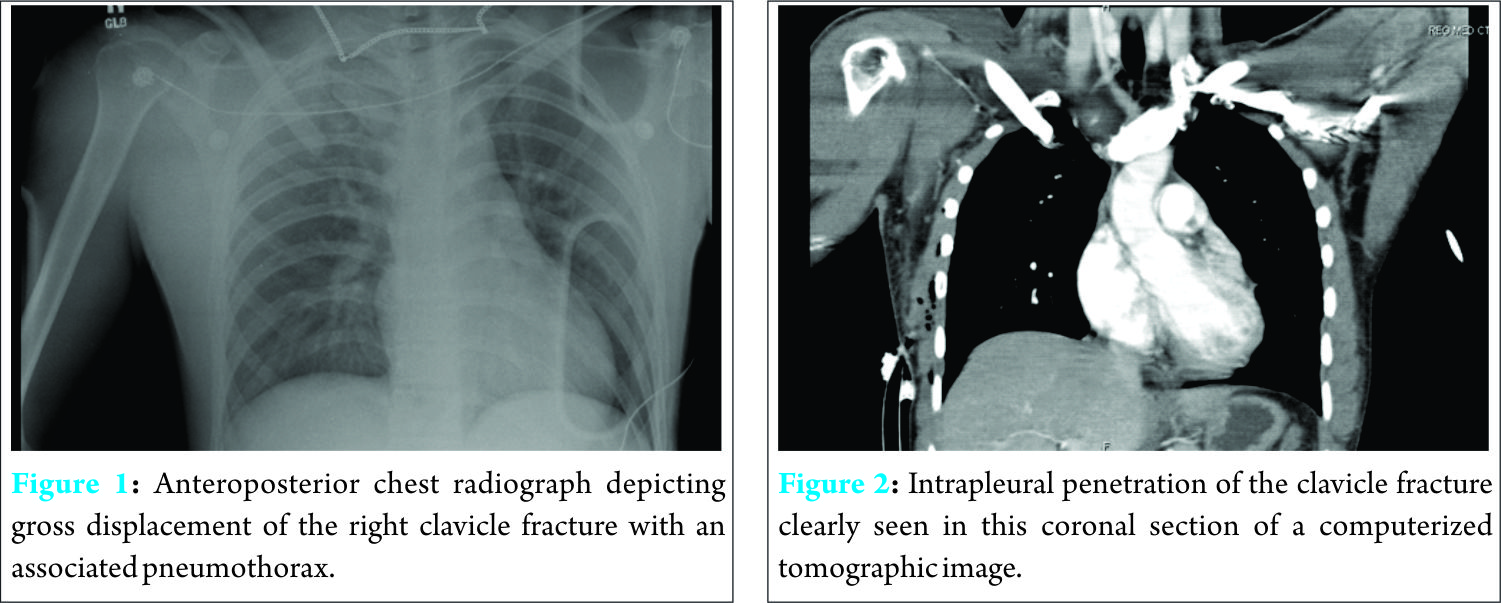
Radiographic analysis of his chest revealed a right proximal third clavicle fracture with inferior displacement complicated by a partial pneumothorax (Fig. 1). He had also sustained a displaced femoral shaft fracture. A chest thoracostomy tube was inserted emergently into the right pleural cavity and placed under suction to inflate the lung. Further radiographic studies including computerized tomography images confirmed that the fractured clavicle had penetrated the pleural cavity and caused a partial lung collapse (Fig. 2). The patient was initially placed in a sling for the clavicle fracture to allow access to the thoracostomy site.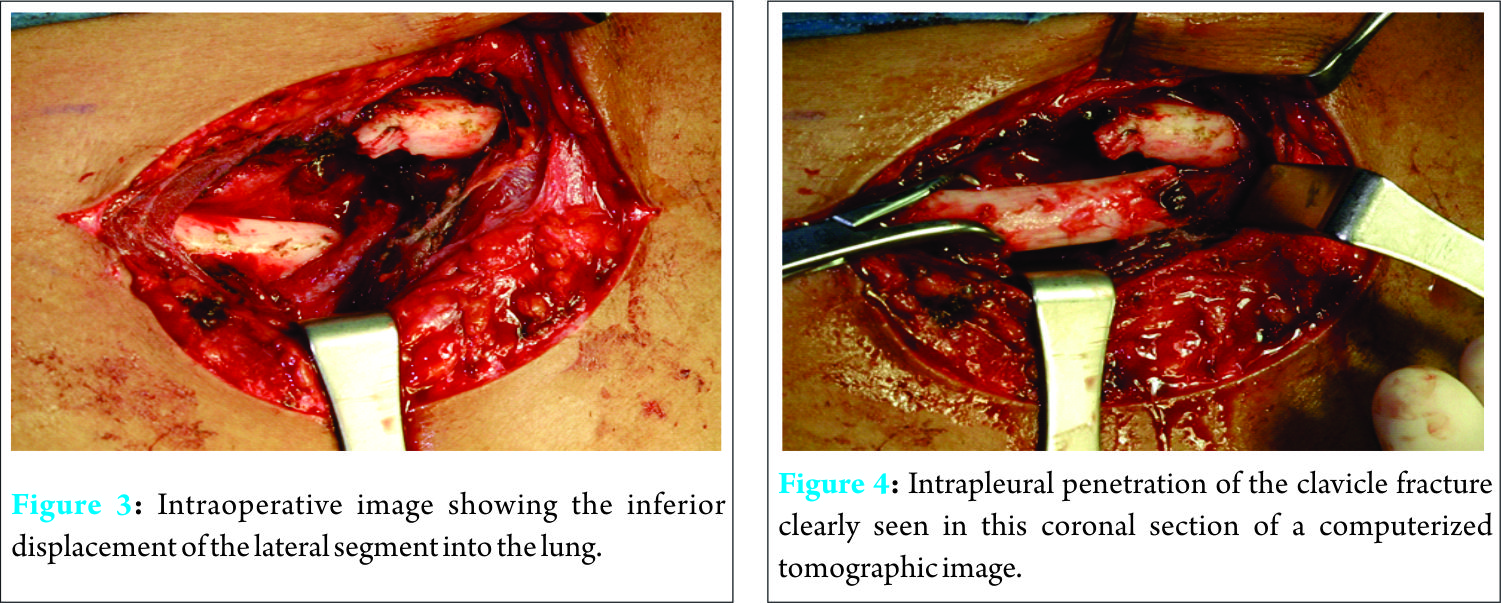
The patient underwent intramedullary nailing of his femur with a centromedullary device without complication the day of his injury. Due to the magnitude of displacement of the clavicle fracture, it was thought that achieving union with nonoperative modalities would be problematic. Pulmonary alveolar tissue seemed to be interposed in the fracture site further complicating the probability of union as well pneumothorax resolution with conservative treatment. The patient was counseled regarding both the orthopedic and cardiopulmonary risks of the surgery. If a closed reduction was unsuccessful, he was informed that an open reduction would be indicated. He understood the possible complications and wished to proceed. 2 days after stabilization of his femur fracture, the patient had an open reduction with internal fixation of his right clavicle. The patient was positioned supine on a radiolucent table. After multiple unsuccessful attempts at closed reduction, a traditional anterior approach was employed to gain access to the fracture (Fig. 3). Once the fracture was exposed and the chest tube under suction, a pointed reduction clamp was used to retract the lateral fragment from the pleural cavity (Fig. 4). There was noted to be some comminution at the fracture site. A general trauma surgeon was available in the operating room in case of any cardiopulmonary compromise. The patient’s vital signs and oxygenation remained stable throughout the operative procedure. After debridement of the fracture ends, the fracture was reduced and provisionally fixed with a bone holding reduction clamp. A six-hole locking 3.5 mm dynamic compression plate was affixed to the clavicle with hybrid screw technique to achieve stable fixation (Fig. 5). On the 2nd post-operative day, his chest thoracostomy tube was removed without incident. The patient was discharged from the hospital on the 3rd post-operative day. At 6-month follow-up, the patient did not complain of pulmonary symptoms. His wounds were well healed and he had regained full active range of motion of his shoulder. Repeat radiographs showed no residual pneumothorax and a healed clavicle fracture (Fig. 6).
Discussion
Pneumothoraces can occur with high-energy chest trauma. They are more commonly associated with scapula and rib fractures [20, 21]. Clavicle fractures that cause lung collapse are rare. To the best of our knowledge, there have only been 11 reported cases in the literature. All but one of these fractures was managed nonoperatively with a sling or a shoulder immobilizer variant. Union was achieved in all of these cases and the pneumothoraces resolved. Operative treatment of closed clavicle fractures has received increased attention in recent reports. Plate fixation and intramedullary nailing of the clavicle have traditionally been reserved for open fractures, nonunions, malunions, and vascular compromise [22, 23, 24]. We report a case of a pneumothorax caused by violation of the pleural cavity by a fracture fragment. Despite multiple attempts at closed reduction, the fracture was immobile. There have been recent reports in the literature regarding estimating the risk of nonunion of clavicle fractures [25, 26]. In our case, nonoperative treatment of the fracture would not have been successful due to the gross displacement of the fracture fragment. Furthermore, there appeared to be pulmonary tissue interposed in the fracture site that would have inhibited bony union as well. In addition, resolution of the pneumothorax would not have been possible without operative repair of the fracture due to its displacement into the pleural cavity. Therefore, plate fixation of the clavicle served to treat both the fracture and pneumothorax. Functional outcome studies have also revealed that residual deficits do exist with closed treatment methods [27, 28, 29]. Given the patient’s young age and high functional demand, even the prospect of residual disability from a nonunion or malunion would have been unacceptable. These factors influenced the decision-making process to manage this patient with an open reduction and internal fixation. Different implants have been used in the management of operative clavicle fractures. The results of intramedullary fixation have not been as promising as plate fixation [30]. Most of the reports have studied midshaft clavicle fractures rather than ones that occur at the proximal third [31]. Given the fracture pattern, location, and displacement, plate fixation was thought to be the most reliable for definitive care. We recommend having a thoracic surgeon available during the reduction. If intrathoracic pathology or bleeding is encountered, a thoracic surgeon may need to extend the approach to address additional chest injuries. Statistically, most clavicle fractures heal uneventfully. While low-energy fractures with minimal displacement may be managed by closed methods, displaced high-energy fractures should prompt the possibility of open treatment. In our case, the clavicle fracture was also associated with a femur fracture. When clavicle fractures are found in a polytraumatized patient, clinicians should investigate the possibility of additional chest injuries. Traditionally, intrathoracic chest trauma has been associated with fractures of the ribs and scapula. Clinicians should now consider pneumothorax in patients with clavicle fractures and high-energy injury mechanisms.
Conclusion
Closed clavicle fractures typically heal uneventfully. Low energy, minimally displaced clavicle fractures can be managed nonoperatively, but high energy, significantly displaced injuries may require operative repair. Specifically, if these injuries result in pneumothorax, physicians shoulder consider operative repair for both treatment of the bony defect as well resulting pneumothorax.
Clinical Message
Pneumothorax is not a commonly described complication of clavicle fractures. Patients with high-energy mechanisms and severely displaced injuries are most at risk for this complication, and detailed evaluation is essential. Severely displaced injuries with penetration into the pleural space prevent fracture union as well as resolution of the pneumothorax, and therefore, operative repair of these fractures should be considered for treatment of the bony defect as well as pneumothorax.
References
1. Denard PJ, Koval KJ, Cantu RV, Weinstein JN. Management of midshaft clavicle fractures in adults. Am J Orthop (Belle Mead NJ) 2005;34(11):527-536.1. Denard PJ, Koval KJ, Cantu RV, Weinstein JN. Management of midshaft clavicle fractures in adults. Am J Orthop (Belle Mead NJ) 2005;34(11):527-536.
2. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res 1994;300:127-132.
3. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg 2002;11(5):452-456.
4. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80(3):476-484.
5. Graves ML, Geissler WB, Freeland AE. Midshaft clavicular fractures: The role of operative treatment. Orthopedics 2005;28(8):761-764.
6. Kitsis CK, Marino AJ, Krikler SJ, Birch R. Late complications following clavicular fractures and their operative management. Injury 2003;34(1):69-74.
7. Kloen P, Sorkin AT, Rubel IF, Helfet DL. Anteroinferior plating of midshaft clavicular nonunions. J Orthop Trauma 2002;16(6):425-430.
8. Kloen P, Werner CM, Stufkens SA, Helfet DL. Anteroinferior plating of midshaft clavicle nonunions and fractures. Oper Orthop Traumatol 2009;21(2):170-179.
9. Dath R, Nashi M, Sharma Y, Muddu BN. Pneumothorax complicating isolated clavicle fracture. Emerg Med J 2004;21(3):395-396.
10. Dugdale TW, Fulkerson JP. Pneumothorax complicating a closed fracture of the clavicle. A case report. Clin Orthop Relat Res 1987;221:212-214.
11. Malcolm BW, Ameli FM, Simmons EH. Pneumothorax complicating a fracture of the clavicle. Can J Surg 1979;22(1):84.
12. Meeks RJ, Riebel GD. Isolated clavicle fracture with associated pneumothorax: A case report. Am J Emerg Med 1991;9(6):555-556.
13. Steenvoorde P, van Lieshout AP, Oskam J. Conservative treatment of a closed fracture of the clavicle complicated by pneumothorax: A case report. Acta Orthop Belg 2005;71(4):481-483.
14. Williams RJ. Significant pneumothorax complicating a fractured clavicle. J Accid Emerg Med 1995;12(3):218-219.
15. Feriani N, Ben Ghezala H, Snouda S. Pneumothorax caused by an isolated midshaft clavicle fracture. Case Rep Emerg Med 2016;2016:2409894.
16. Hani R, Ennaciri B, Jeddi I, El Bardouni A, Mahfoud M, Berrada MS. Pneumothorax complicating isolated clavicle fracture. Pan Afr Med J 2015;21:202.
17. Lohse GR, Lee DH. Clavicle fracture with intrathoracic displacement. Orthopedics 2013;36(8):e1099-e1102.
18. Geraci G, Pisello F, Sciumè C, Sunseri A, Romeo M, Li Volsi F, et al. Clavicle fracture complicated by pneumothorax. Case report and literature review. G Chir 2007;28(8-9):330-333.
19. Taitsman LA, Nork SE, Coles CP, Barei DP, Agel J. Open clavicle fractures and associated injuries. J Orthop Trauma 2006;20(6):396-399.
20. McLennan JG, Ungersma J. Pneumothorax complicating fracture of the scapula. J Bone Joint Surg Am 1982;64(4):598-599.
21. Munshi IA, Becker EJ, Bean M. Pulmonary parenchymal and bronchial arterial injuries secondary to blunt trauma. J Trauma 2001;51(2):418.
22. Chen PY, Lin CC, Wang CC, Tsai CL. Closed reduction with intramedullary fixation for midclavicular fractures. Orthopedics 2004;27(5):459-462.
23. Coupe BD, Wimhurst JA, Indar R, Calder DA, Patel AD. A new approach for plate fixation of midshaft clavicular fractures. Injury 2005;36(10):1166-1171.
24. Shen WJ, Liu TJ, Shen YS. Plate fixation of fresh displaced midshaft clavicle fractures. Injury 1999;30(7):497-500.
25. Nowak J, Holgersson M, Larsson S. Can we predict long-term sequelae after fractures of the clavicle based on initial findings? A prospective study with nine to ten years of follow-up. J Shoulder Elbow Surg 2004;13(5):479-486.
26. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am 2004;86-A(7):1359-1365.
27. McKee MD, Pedersen EM, Jones C, Stephen DJ, Kreder HJ, Schemitsch EH, et al. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am 2006;88(1):35-40.
28. McKee MD, Wild LM, Schemitsch EH. Midshaft malunions of the clavicle. J Bone Joint Surg Am 2003;85-A(5):790-797.
29. Yates DW. Complications of fractures of the clavicle. Injury 1976;7(3):189-193.
30. Grassi FA, Tajana MS, D’Angelo F. Management of midclavicular fractures: Comparison between nonoperative treatment and open intramedullary fixation in 80 patients. J Trauma 2001;50(6):1096-1100.
31. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Evidence-Based orthopaedic trauma working treatment of acute midshaft clavicle fractures: Systematic review of 2144 fractures: On behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma 2005;19(7):504-507.
 |
 |
 |
| Dr. Ryan D DeAngelis | Dr. Kenneth W Graf Jr | Dr. Rakesh P Mashru |
| How to Cite This Article: DeAngelis RD, Graf KW Jr, Mashru RP. Intrapleural Penetration of a Clavicle Fracture: An Indication for Operative Fixation. Journal of Orthopaedic Case Reports 2017 Jul-Aug;7(4):17-20 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


