
[box type=”bio”] Learning Points for this Article: [/box]
After wide resection of rare spindle cell hemangioma of the midfoot, a curved construct of iliac bone graft could be appropriately used to create the dome of the foot.
Case Report | Volume 7 | Issue 5 | JOCR Sep – Oct 2017 | Page 75-79 | Tanawat Vaseenon, Jirawat Saengsin, Nuttaya Pattamapaspong, Jongkolnee Settakorn, Dumnoensun Pruksakorn. DOI: 10.13107/jocr.2250-0685.904
Authors: Tanawat Vaseenon [1], Jirawat Saengsin [1], Nuttaya Pattamapaspong [2], Jongkolnee Settakorn [3], Dumnoensun Pruksakorn [1].
[1] Department of Orthopaedics, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
[2] Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
[3] Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Address of Correspondence
Dr. Tanawat Vaseenon,
Department of Orthopaedics, Faculty of Medicine, Chiang Mai University,
110 Intawaroros Road, Sriphum, Muang – 50200, Chiang Mai, Thailand.
E-mail: tvaseenon@yahoo.com
Abstract
Introduction: Spindle cell hemangioma (SCH) of the bone (mid-foot) is a rare disease, but it can cause symptomatic pain and invade surrounding tissues lead to limb deformities and functional loss.
Case Report: We report the case of a 35-year-old woman who experienced a firm mass over the left midfoot for 5 years causing pain and numbness in the foot. Radiographs showed a geographic osteolytic lesion involving calcification of the base of the 2nd and 3rd metatarsals, cuneiforms bones and surrounding soft tissue. Magnetic resonance imaging revealed a lobulated mass in the mid-foot containing tangles of tortuous blood vessels and dark foci characteristic of phleboliths. Wide resection of the 2nd and 3rd cuneiforms, metatarsal bones and surrounding tissues with a curved iliac bone graft reconstruction were performed. Histological assessment revealed a lesion composed of a vascular channel containing endothelial cells with smooth muscle but without cellular atypia. The definite diagnosis was spinal cell hemangioma. The pain resolved within 4 months. The foot was stable, and no recurrence was found at the 48 months follow-up.
Conclusion: This unusual disease, SCH of the mid-foot responded favorably to wide resection and curved iliac bone grafting. It is suggested that this approach will provide a satisfactory functional result.
Keywords: Foot, iliac bone graft, reconstruction, hemangioma, wide resection, tumor.
Introduction
Spindle cell hemangioma (SCH), also known as spindle cell hemangioendothelioma, is an uncommon benign vascular tumor that was first described in 1986 by Weiss and Enzinger, as a rare type of hemangioma [1]. This tumor is commonly detected in superficial soft tissue of the distal parts of the extremities and usually occurs in young adults. SCH differs from other histologic types of hemangioma in that it does not frequently present in the bone [2]. To the best of our knowledge, there have been only four cases previously reported in English in the published literature [2, 3, 4, 5]. Moreover, there have been no reported cases of SCH arising in the long bones of the hands or feet such as the metatarsal bones. Although SCH was initially described as a type of hemangioendothelioma of intermediate or low-grade malignancy, it has since been demonstrated that the tumor is benign [6]. Hence, the main treatment of SCH is surgery, commonly wide excision. In this paper, we report an extremely rare case of SCH in the metatarsal bones that were treated with wide resection of the 2nd and 3rd metatarsal bones and surgical reconstruction with an iliac bone graft.
Case Report
A 35-year-old Thai woman presented with a history of pain and swelling at the dorsum of the left foot in November 2012. She noticed that the pain occurred when walking or standing. The pain was relieved when sitting or lying down. The symptoms were severe when she walked a long distance or engaged in strenuous exercise. She had been suffering from recurrent pain for 5 years. Her symptoms did not improve with medication and got worse in a month period. Musculoskeletal evaluation showed mild swelling and a tender mass located at the 2nd and 3rd metatarsal bones of the left foot. Results of vascular, neurologic, and dermatologic examinations of the lower extremities were normal (Fig. 1).
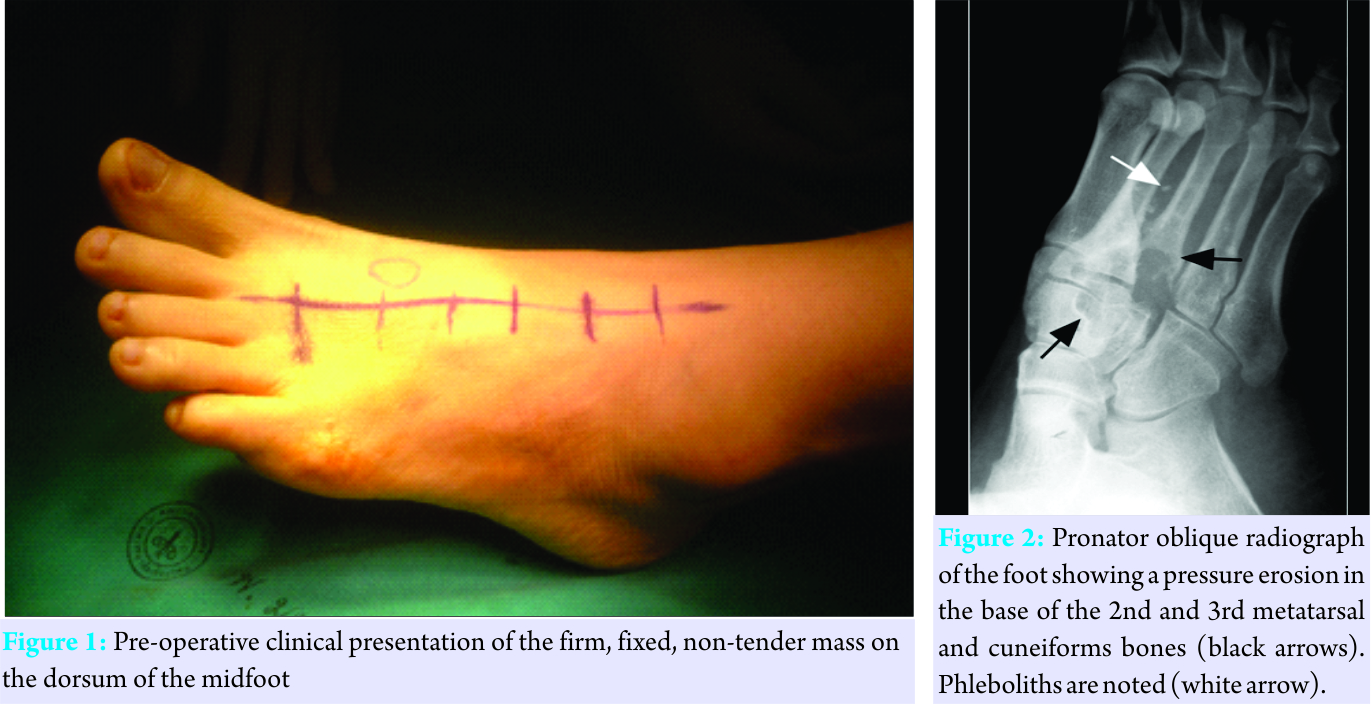
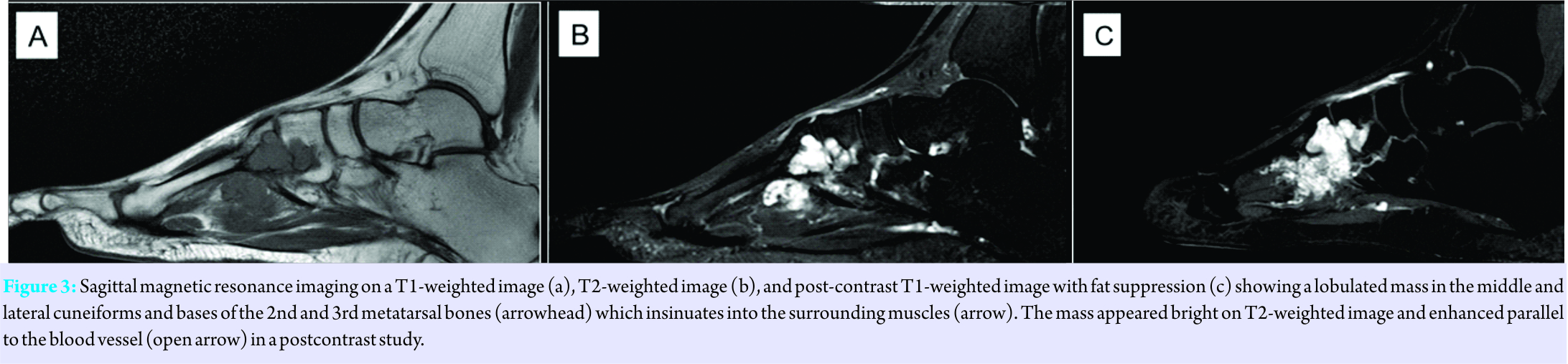
A plain radiograph showed bone destruction in the base of the 2nd and 3rd metatarsal and cuneiforms bones surrounded by soft tissue calcification (Fig. 2). Magnetic resonance imaging (MRI) revealed a lobulated mass in the midfoot, measuring 4 × 3 × 3 cm and containing tangles of tortuous blood vessels and dark foci characteristic of phleboliths. The mass appeared bright on T2-weighted images and was enhanced parallel to blood vessels in a postcontrast study. The mass involved the middle and lateral cuneiforms and the base of the 2nd and 3rd metatarsal bones as well as insinuates in the surrounding muscle. Based on the imaging feature, the diagnosis was cavernous hemangioma (Fig. 3).

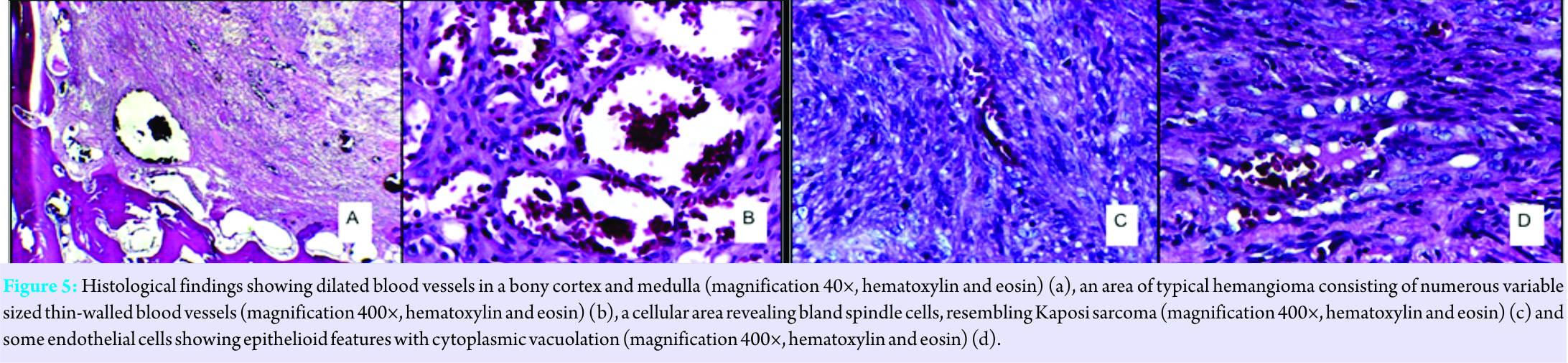
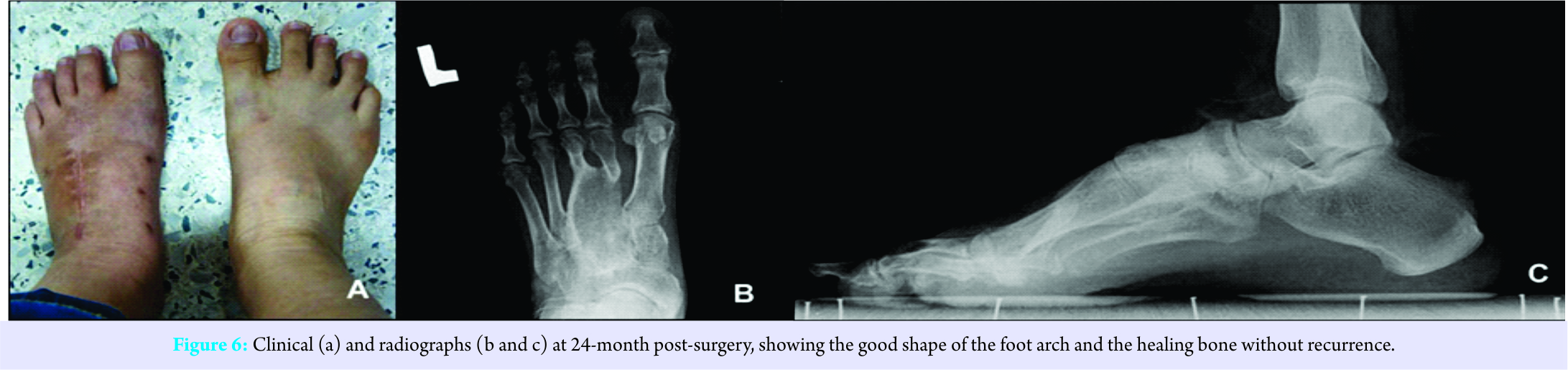
Regular laboratory data showed no abnormalities. The surgical operation was performed in February 2013. After longitudinal skin incision, a wide resection of the tumor including the 2nd and 3rd metatarsals and the intrinsic and extrinsic muscles of the toes was performed. A curved iliac bone graft was harvested and fitted into the resection space of the midfoot. Multiple Kirschner wire fixation to the adjacent bones was accomplished. Subcutaneous tissue and skin were closed with a redivac drain. A short leg cast was applied for 2 months, allowing non-weight bearing ambulation (Fig. 4). The pathology report revealed a mass of lobulated hemorrhagic lesions. The tumor involved soft tissue, cortical bone, and medullary bone. Histologically, there were variable sized blood-filled vessels, some of which were dilated and thrombosed. In the spaces between the blood vessels, there were cellular areas consisting of bland spindle cells. Epithelioid endothelial cells containing cytoplasmic lumens were observed (Fig. 5). At 4 months after the reconstruction, the patient could walk without pain but could not bear full weight. At 48 months after surgery, the patient could ambulate well without limitations during daily activities. The plain radiographs showed no evidence of recurrence or metastasis (Fig. 6).
Discussion
In the present case, the chief complaint was swelling of the midfoot, along with a 5 years history of gradual progression of swelling. The plain radiograph pointed toward a benign bone tumor of the metatarsal as one of the differential diagnosis alternatives. Other alternatives included post-traumatic cyst, eosinophilic granuloma, aneurysmal bone cyst, enchondroma, giant cell tumor, vascular bone tumor, or possibly chondroblastoma as previously reported in the literature [7]. MRI and histopathologic examination established the definitive diagnosis. Weiss and Enzinger in 1986 described a new type of vascular tumor that combines the features of both cavernous hemangioma and Kaposi’s sarcoma [1]. This vascular tumor designated “spindle cell hemangioendothelioma” or SCH, has limited malignant potential. Males and females are equally affected, with a median age of 34 years (range, 8–78 years) [6]. Patients with SCH typically present with slow-growing, infiltrative, uninodular, or multinodular dermal or subcutaneous masses originating most commonly in the distal extremities, with a tendency to cluster in one region [6, 8]. The head, neck, chest, and abdomen have also been reported as primary sites of origin in a minority of cases [6]. These masses often cause little or no discoloration of the overlying skin, which precludes identification as a vascular lesion [9]. However, SCH that originates from bone is very rare. Only four cases have been reported of SCH arising from bone in different locations including frontal bone, spine, calcaneus, and fibula [2, 3, 4, 5]. As noted above, SCH was originally categorized as a low-grade malignancy and was named “spindle cell hemangioendothelioma” because the tumor was thought to have limited malignant potential and to have frequent local recurrence [2]. It has now been demonstrated that this lesion behaves in an indolent fashion. In spite of the lack of metastasis, approximately 60% of SCH recur. There is no evidence that these local recurrences represent either a contiguous spread of neoplasm along affected vessels or multifocal neoplastic involvement of a vessel [4]. Several therapeutic approaches, including surgery, systemic steroids, cryotherapy, laser therapy, radiation therapy, cytotoxic drugs, and selective embolization, have been used [10]. Recombinant interleukin 2, a T-cell derived lymphokine with immunologic functions (e.g., induction of lymphokine-activated killer cells, augmentation of activities of cytotoxic T cells, and natural killer cells), has been tried with success. Radiation therapy should be discouraged due to the reported incidence of sarcomatous transformation with subsequent metastasis [6, 10]. The treatment for SCH of the bone, due to its benign behavior, has been simple surgical resection and wide local excision [6]. After resection of a tumor in the midfoot, the residual defect has typically been reconstructed with various autografts (such as radial, rib, scapular, iliac crest, or fibula), or allografts [11, 12, 13]. Other reconstructive options for mid-foot resection include the use of free vascularized musculocutaneous or septocutaneous flaps [14]. Successful use of fibular autograft reconstruction without vascularization has been reported following resection of a malignant metatarsal [14, 15, 16] and a benign tumor [7]. The purported advantages of this type of graft are the availability of a longer graft, higher resistance to infection, rapid graft incorporation, and osseous union [14]. In addition, reconstruction with a fibular graft has distinct advantages over the iliac crest for the reconstruction of large defects in the mid-foot because it is similar in shape and diameter to the metatarsals, is easily accessible, and has low donor-site morbidity. Furthermore, because the fibula is highly vascularized and composed primarily of cortical bone, it can thicken to withstand and adapt to the stresses of weight-bearing, and yet it is thin enough to accommodate regular shoe wear, thus providing a functional reconstruction [14]. On the other hand, the vascularized fibula graft is a complicated operation. It is difficult to reconstruct multiple concomitant bone defects, and meticulous microsurgical techniques are required. In addition, the graft should be cut and folded to create a ‘‘double-barreled’’ graft reconstruction of the two metatarsals, making the technique even more demanding [13]. Two cases of a patient with a giant cell tumor involving the metatarsal bone were reported to have excellent foot function after resection and reconstruction by an autogenous iliac bone graft .For reasons of the simplicity of the surgical techniques involved and the compatibility of size and shape, that method is promoted for use with large defects of the midfoot following bone and soft tissue resection. That method also makes it possible to repair the dome shape of the arch of the foot and to ensure appropriate weight transfer [12, 13]. Fixation of the graft has been done with multiple techniques such as plates and screws or Steinmann pins. Plate and screw fixations seem to promote faster union and allow earlier weight bearing; however, the risk of nonunion has been mentioned in the literature [13]. The case presented here of iliac bone grafting to midfoot reconstruction after wide resection of SCH resulted in an excellent outcome with no recurrence. The patient can walk and run without pain. Her foot is stable and fits well in shoes. Union of the graft was achieved within 3 months of surgery plus multiple K-wire fixation and temporary casting. We feel that the advantages of this fixation and graft choice include the size and shape fit between the curve of the iliac bone and that of the midfoot, the strength of a tricortical iliac bone graft, and the simplicity and ability to design the graft before harvesting. The disadvantage was donor site morbidity. Good functional scores at short-term follow-up confirm that the iliac bone graft reconstruction after midfoot resection is a suitable surgical technique. When SCH is localized to a metatarsal, autologous structural iliac grafting after excision of the metatarsal is a treatment option which, based on our experience with this patient, we believe can be useful. As with all tumors, regular follow-up of the patient after surgical treatment is indicated.
Conclusion
Iliac bone grafting reconstruction of a wide resection in the midfoot area is an alternative treatment for a benign SCH bone tumor of the foot that required wide resection of the bone and soft tissue.
Clinical Message
A SCH of the bone is rare to occur in the midfoot area. Wide resection of the bone and soft tissue surrounding is necessary. A curve autologous iliac bone grafting with soft tissue reconstruction can be challenging. Stability and foot function are also need to be concerned.
References
1. Weiss SW, Enzinger FM. Spindle cell hemangioendothelioma. A low-grade angiosarcoma resembling a cavernous hemangioma and kaposi’s sarcoma. Am J Surg Pathol 1986;10:521-30.
2. Hakozaki M, Tajino T, Watanabe K, Yamada H, Kikuchi S, Hojo H, et al. Intraosseous spindle cell hemangioma of the calcaneus: A case report and review of the literature. Ann Diagn Pathol 2012;16:369-73.
3. Tsukamoto S, Honoki K, Shimada K, Fujii H, Kido A, Takano M, et al. Periosteal spindle cell hemangioma of the fibula: A case report. Skeletal Radiol 2013;42:1165-8.
4. Talan-Hranilović J, Vucić M, Sajko T, Bedek D, Tomić K, Lupret V, et al. Spinal spindle cell haemangioma: An atypical location. Acta Neurochir (Wien) 2007;149:325-8.
5. Cansiz H, Yener M, Dervisoglu S, Kalekoglu N. Hemangioendothelioma of the frontal bone in a child. J Craniofac Surg 2003;14:724-728.
6. Perkins P, Weiss SW. Spindle cell hemangioendothelioma. An analysis of 78 cases with reassessment of its pathogenesis and biologic behavior. Am J Surg Pathol 1996;20:1196-204.
7. Dhatt SS, Bhagwat KR, Kumar V, Dhillon MS. Chondroblastoma in a metatarsal treated with autogenous fibular graft: A case report. J Foot Ankle Surg 2012;51:356-61.
8. Nayler SJ, Rubin BP, Calonje E, Chan JK, Fletcher CD. Composite hemangioendothelioma: A complex, low-grade vascular lesion mimicking angiosarcoma. Am J Surg Pathol 2000;24:352-61.
9. Dhawan SS, Raza M. Spindle cell hemangioendothelioma. Cutis 2007;79:125-8.
10. Setoyama M, Shimada H, Miyazono N, Baba Y, Kanzaki T. Spindle cell hemangioendothelioma: Successful treatment with recombinant interleukin-2. Br J Dermatol 2000;142:1238-9.
11. Wang EH, Arbatin JJ. Allograft reconstruction of a large giant cell tumor of the first metatarsal: A case report. Foot Ankle Int 2008;29:97-100.
12. Szendröi M, Antal I, Perlaky G. Mid-foot reconstruction following involvement of five bones by giant cell tumor. Skeletal Radiol 2000;29:664-7.
13. Ahn JH, Choy WS, Kim HY, Kim HS. Midfoot reconstruction for a large, aggressive giant-cell tumor: A case report. J Bone Joint Surg Am 2011;93:e133(1-6).
14. Toma CD, Dominkus M, Pfeiffer M, Giovanoli P, Assadian O, Kotz R, et al. Metatarsal reconstruction with use of free vascularized osteomyocutaneous fibular grafts following resection of malignant tumors of the midfoot. A series of six cases. J Bone Joint Surg Am 2007;89:1553-64.
15. Toriyama K, Kamei Y, Yagi S, Uchibori M, Nishida Y, Torii S, et al. Reconstruction of the first and second metatarsals with free vascularised double-barrelled fibular graft after resection of a chondrosarcoma. J Plast Reconstr Aesthet Surg 2009;62:e580-3.
16. Ozger H, Akgül T, Eren I, Topalan M. Midfoot reconstruction with free vascularized fibular graft after wide resection: A case report. Acta Orthop Belg 2011;77:702-6.

| How to Cite This Article: Vaseenon T, Saengsin J, Pattamapaspong N, Settakorn J, Pruksakorn D. Spindle Cell Hemangioma of the Midfoot: A Case Report. Journal of Orthopaedic Case Reports 2017 Sep-Oct;7(5):75-79 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


