
[box type=”bio”] Learning Point for this Article: [/box]
Masson’s tumor is rare and it’s diagnosis can be challenging. Although resection is considered the treatment of choice, embolization of the vascular supply of the tumor can be a viable option.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 23-25| Ippokratis Pountos, Asim Siddiqui. DOI: 10.13107/jocr.2250-0685.1032
Authors: Ippokratis Pountos[1], Asim Siddiqui[2]
[1]Department of Trauma and Orthopaedics, University of Leeds, UK.
[2]Department of Trauma and Orthopaedic, Calderdale and Huddersfield NHS Trust, UK.
Address of Correspondence:
Dr. Ippokratis Pountos,
Department of Trauma and Orthopaedic Surgery, Academic Department of Trauma and Orthopaedics, 9.83 Worsley Building, University of Leeds, UK.
E-mail: pountos@doctors.org.uk
Abstract
Introduction: Intravascular papillary endothelial hyperplasia or Masson’s tumor is a rare benign lesion of vascular origin characterized by abnormal proliferation of endothelial cells.
Case Report: We present a case of this lesion involving the knee joint of a Caucasian woman who was referred to our institution for the evaluation of recurrent right knee pain. Her symptoms have started insidiously 5 years earlier following minor trauma. Recurrent symptomatic knee effusion was the cardinal symptom. Following the surgical excision of the lesion, recurrence occurred 2 years later. The tumor was successfully treated with embolization of its vascular supply.
Conclusion: Masson’s tumor involving the synovium is an uncommon condition. The intermittent symptomatology and normal appearance of biopsies taken arthroscopically during asymptomatic periods can make the diagnosis challenging. Although resection is proposed to prevent recurrence, embolization of the vascular supply of the tumor can be a viable alternative.
Keywords: Masson’s tumor, intravascular papillary endothelial hyperplasia.
Introduction
Intravascular papillary endothelial hyperplasia (IPEH) is a rare benign lesion of vascular origin characterized by abnormal proliferation of endothelial cells. In 1923 Masson first described the lesion as a “vegetant intravascular hemangioendothelioma” in a patient with an unreducible ulcerated hemorrhoid [1]. Subsequently, several names have been proposed with the most dominant to be IPEH [2]. IPEH is most commonly located in the skin and subcutaneous tissue. However, it may occur in any location in the body [2]. In the herein manuscript, we report a case of IPEH involving the knee synovium.
Case Report
A 22-years-old Caucasian female was referred to our department, complaining of a 5-year history of intermittent pain in her right knee. She did not suffer from any medical condition, she was not on any medications and never smoked. Her symptoms started insidiously, following a minor soft tissue injury (no fracture).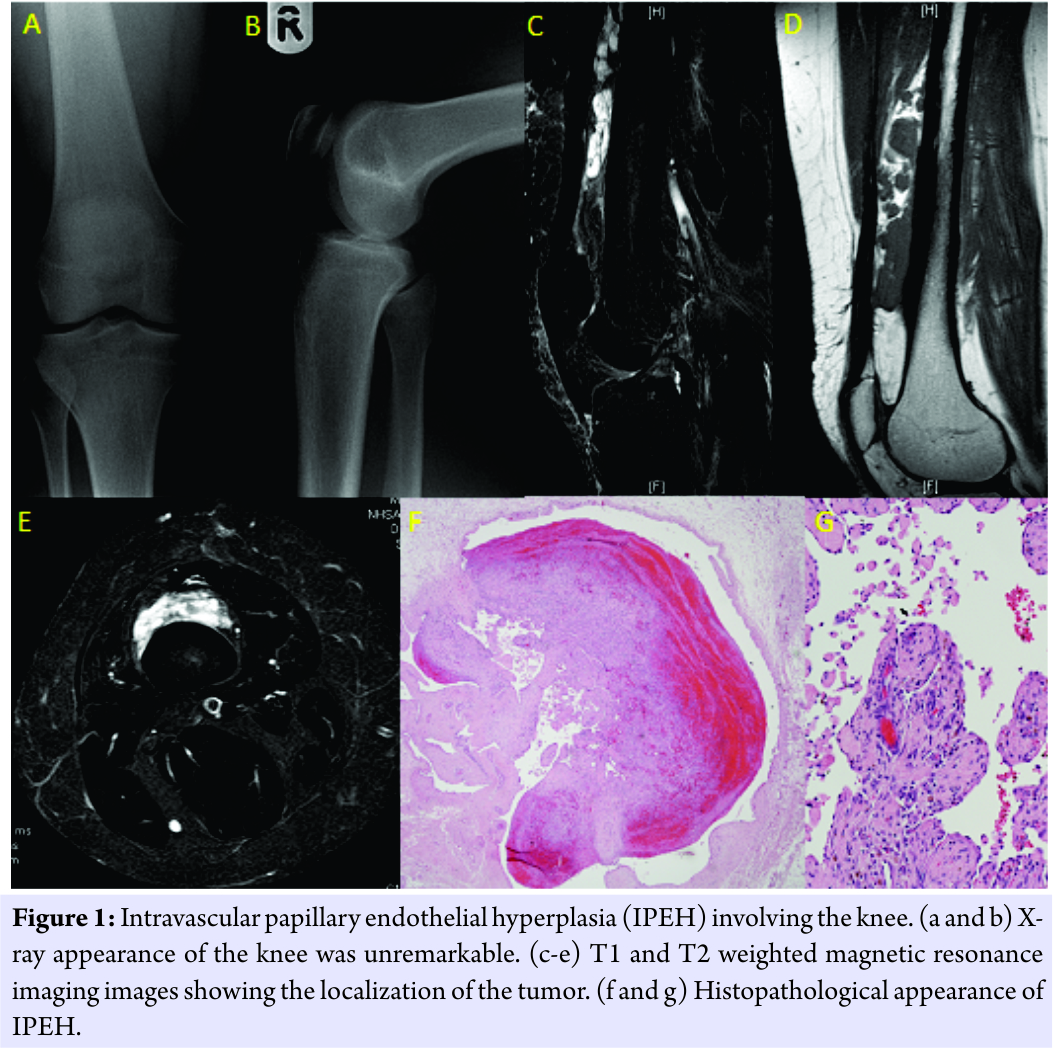 On clinical examination, she was found to have a right knee effusion and limitation of movement (ROM 10-90°). She had severe pain over her knee. She could weight bear with significant discomfort. Her blood tests were all normal, including the coagulation screen and all inflammatory markers. The X-rays performed were unremarkable (Fig. 1). An magnetic resonance imaging (MRI) scan was performed which suggested the presence of a suprapatellar fluid collection with cysts arising from the synovium. Following these results, an arthroscopy was performed. The cysts were excised and biopsied. The biopsies revealed normal synovium. Following the procedure, the patient remained asymptomatic for approximately 3 years. She then returned with similar symptomatology. A second MRI was performed showed the presence of a suprapatellar fluid collection measuring 4.7 × 2.1 cm at the suprapatellar area. No hemosiderin was noted within the collection and no local erosion. Surgical exploration was performed, and a poorly encapsulated vascular mass was encountered extending from the distal belly of the vastus intermedius to the knee. Excessive use of electrocautery and ligation of the numerous vessels were performed during resection. The histological examination of the mass revealed a dilated vascular space containing fibrous papillary projections and organized thrombus. It was suggestive of IPEH (Masson’s Tumor) (Fig. 1f and g). The patient’s symptoms recurred 2 years later. An MRI scan was repeated showing a 1 × 3 × 10 cm cystic lesion of the distal anterior thigh. The patient was then referred to the vascular department for embolization of the vascular supply of the tumor. Following this procedure, the patient has recovered fully, and she now remains asymptomatic to date (5½ years follow-up).
On clinical examination, she was found to have a right knee effusion and limitation of movement (ROM 10-90°). She had severe pain over her knee. She could weight bear with significant discomfort. Her blood tests were all normal, including the coagulation screen and all inflammatory markers. The X-rays performed were unremarkable (Fig. 1). An magnetic resonance imaging (MRI) scan was performed which suggested the presence of a suprapatellar fluid collection with cysts arising from the synovium. Following these results, an arthroscopy was performed. The cysts were excised and biopsied. The biopsies revealed normal synovium. Following the procedure, the patient remained asymptomatic for approximately 3 years. She then returned with similar symptomatology. A second MRI was performed showed the presence of a suprapatellar fluid collection measuring 4.7 × 2.1 cm at the suprapatellar area. No hemosiderin was noted within the collection and no local erosion. Surgical exploration was performed, and a poorly encapsulated vascular mass was encountered extending from the distal belly of the vastus intermedius to the knee. Excessive use of electrocautery and ligation of the numerous vessels were performed during resection. The histological examination of the mass revealed a dilated vascular space containing fibrous papillary projections and organized thrombus. It was suggestive of IPEH (Masson’s Tumor) (Fig. 1f and g). The patient’s symptoms recurred 2 years later. An MRI scan was repeated showing a 1 × 3 × 10 cm cystic lesion of the distal anterior thigh. The patient was then referred to the vascular department for embolization of the vascular supply of the tumor. Following this procedure, the patient has recovered fully, and she now remains asymptomatic to date (5½ years follow-up).
Discussion
IPEH or Masson’s Tumor is a benign lesion of vascular origin characterized by abnormal proliferation of endothelial cells. IPEH could be of three distinct types. These include the primary form (56%); involving an isolated dilated blood vessel, secondary (40%); in pre-existing vascular lesions and more rarely, an extravascular form (4%) associated with hematoma [3]. Trauma does not seem to be related to any of the above forms and has been reported in only a small fraction of the patients (approximately 4%) [4-6]. The primary IPEH form has a predilection for the deep dermis and subcutaneous soft tissue of head, neck, fingers, and trunk. In the subcutaneous tissues, it can appear as small, firm bluish nodule causing discoloration of the overlying skin. It is usually asymptomatic with no sex predilection. Multiple lesions are uncommon; only described following interferon-β treatment. In secondary form, the clinical findings are related to the primary tumor. Although it can be related to any vascular tumor, deep-seated hemangiomas of cavernous type are the most common association. The third form is of an extravascular location associated with a hematoma. It is the rarest and only reported on case report basis including the herein report. The exact pathophysiology of IPEH is currently unknown. It has been proposed that an unusual form of organizing thrombus could be the underlying cause. An association has been made with the β-fibroblast growth factor (β-FGF). Macrophages invading the tumor seem to produce β-FGF, which results in the upregulation of the proliferation of endothelial cells. In turn, endothelial cells seem to release more β-FGF leading to a vicious cycle. IPEH immunohistochemical studies have shown the presence of factor VIII-related antigen, CD34+ cells, and factors XIIIa [5, 6]. These findings together with the lack of spread, mitosis, necrosis, as well as the presence of cellular areas devoid of vascular differentiation, distinguish it from other tumors such as angiosarcoma, Kaposi’s sarcoma, and angiolymphoid hyperplasia [5, 6]. IPEH posses a diagnostic challenge, and our report highlights the difficulties in diagnosing this non-neoplastic lesion. The periodic nature of the symptomatology, lasting only for a limited amount of time with spontaneous resolution, has been the main challenge. Similar cases of recurrent bleeding have been previously reported [2]. The first MRI has highlighted synovial cysts with a significant suprapatellar fluid collection. These MR findings in our case are similar to previously reported cases where the low signal intensity on T2 sequences is identified suggesting thrombotic or hemorrhagic material with low signal internal septae. It should be mentioned that the vast majority of the IPEH never reach the attention of the radiology department; therefore, diagnosis of the IPEH using imaging has not been reported. In terms of the treatment of IPEH, surgical excision has been proposed to be the treatment of choice. Spontaneous resolution has been reported, but surgical excision seems to be the most commonly used treatment route. The majority of the available evidence reports good results following excision [2, 7, 8, 9]. However, recurrence is not uncommon, and aggressive forms occur in approximately 10% of the cases [10]. In such cases, radiation and chemotherapy have been successfully utilized in the management of this pathology [11, 12, 13]. Embolization of the feeding vessels has been successful in our case and could represent an alternative treatment modality for the management of these lesions.
Conclusion
Masson’s tumor involving the synovium is uncommon, and its diagnosis remains challenging. Although literature suggests that surgical resection prevents recurrence, embolization of the vascular supply of the tumor can be a viable alternative.
Clinical Message
Masson’s tumor is a rare pathologic entity characterized by IPEH. It is a benign tumor that continues to grow and expand. Depending on the tissue involved, the tumor will result in different symptomatology. In our case, where the knee synovium was involved, recurrent knee pain and hemarthrosis followed by asymptomatic periods made the diagnosis challenging. Small biopsies taken arthroscopically in asymptomatic periods can reveal normal tissue. Although resection is proposed to prevent recurrence, embolization of the vascular supply of the tumor can be a viable alternative.
References
1. Masson P. Hemangioendotheliome vegetant intravasculaire. Bull Soc Anat Paris 1923;93:517-23.
2. Jung TY, Jung S, Lee MC, Kim IY, Kang SS, Kim SH, et al. Papillary endothelial hyperplasia associated with repeated bleeding. Br J Neurosurg 2005;19:428-31.
3. Pins MR, Rosenthal DI, Springfield DS, Rosenberg AE. Florid extravascular papillary endothelial hyperplasia (Masson’s pseudoangiosarcoma) presenting as a soft-tissue sarcoma. Arch Pathol Lab Med 1993;117:259-63.
4. Cerilli LA, Huffman HT, Anand A. Primary renal angiosarcoma: A case report with immunohistochemical, ultrastructural, and cytogenetic features and review of the literature. Arch Pathol Lab Med 1998;122:929-35.
5. Clearkin KP, Enzinger FM. Intravascular papillary endothelial hyperplasia. Arch Pathol Lab Med 1976;100:441-4.
6. Salyer WR, Salyer DC. Intravascular angiomatosis: Development and distinction from angiosarcoma. Cancer 1975;36:995-1001.
7. Erol O, Ozçakar L, Uygur F, Keçik A, Ozkaya O. Intravascular papillary endothelial hyperplasia in the finger: Not a premier diagnosis. J Cutan Pathol 2007;34:806-7.
8. Korkolis DP, Papaevangelou M, Koulaxouzidis G, Zirganos N, Psichogiou H, Vassilopoulos PP, et al. Intravascular papillary endothelial hyperplasia (Masson’s hemangioma) presenting as a soft-tissue sarcoma. Anticancer Res 2005;25:1409-12.
9. Pantanowitz L, Muc R, Spanger M, Sonnendecker H, McIntosh WA. Intravascular papillary endothelial hyperplasia (Masson’s tumor) manifesting as a lateral neck mass. Ear Nose Throat J 2000;79:806, 809-10, 812 passim.
10. Anthony SG, Mudgal CS, DeLaney TF, Shin RD, Raskin KA, Ring DC, et al. Recurrent intravascular papillary endothelial hyperplasia of the right middle finger treated with radiation therapy. J Bone Joint Surg Br 2008;90:95-7.
11. Avellino AM, Grant GA, Harris AB, Wallace SK, Shaw CM. Recurrent intracranial masson’s vegetant intravascular hemangioendothelioma. Case report and review of the literature. J Neurosurg 1999;91:308-12.
12. Kristof RA, Van Roost D, Wolf HK, Schramm J. Intravascular papillary endothelial hyperplasia of the sellar region. Report of three cases and review of the literature. J Neurosurg 1997;86:558-63.
13. Sickler GK, Langford LA. Intracranial tumor-forming papillary endothelial hyperplasia-A case report. Clin Neuropathol 1990;9:125-8.
 |
 |
| Dr. Ippokratis Pountos | Dr. Asim Siddiqui |
| How to Cite This Article: Pountos I, Siddiqui A. Intravascular Papillary Endothelial Hyperplasia (Masson’s Tumor) Involving the Knee Synovium. Journal of Orthopaedic Case Reports 2018. Mar- April; 8(2): 23-25 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


