
[box type=”bio”] Learning Point for the Article: [/box]
In isolated symptomatic cysticercosis, surgical excision is best treatment.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 89-91| Manesh Kumar Jain, Surendra Umesh Kamath, Flora Lobo. DOI: 10.13107/jocr.2250-0685.1126
Authors: Manesh Kumar Jain[1], Surendra Umesh Kamath[1], Flora Lobo[2]
[1]Department of Orthopaedics, Kasturba Medical College, Mangalore. Manipal Academy Of Higher Education, Manipal, Karnataka, India.
[2]Department of Pathology, Kasturba Medical College, Mangalore. Manipal Academy Of Higher Education Manipal, Karnataka, India.
Address of Correspondence:
Dr. Surendra Umesh Kamath,
Department of Orthopaedics, Kasturba Medical College, Mangalore, Manipal Academy Of Higher Education Manipal ,Karnataka, India.
E-mail: skamath3@hotmail.com
Abstract
Introduction: Cysticercosis is more commonly seen in developing countries like India caused by larval stage of Taenia solium. Neurocysticercosis is more commonly seen than isolated muscle involvement. There are very few sporadic cases of isolated biceps muscle involvement, but most of them are managed medically. We are reporting an isolated case of cysticercosis of biceps muscle managed surgically.
Case Report: A 32-year-old male, security personnel by occupation, comes with complaints of painful swelling of the right arm for past 1 week. There was no trauma to the limb and no similar swellings elsewhere in the body. On examination, there was an anteromedial tender swelling of mid-third of arm. X-ray was normal with soft tissue shadow on the anterior aspect. Ultrasound showed cystic lesion with central hyperechoic lesion. Magnetic resonance imaging of arm showed 7.7 mm × 4.8 mm lesion in anteromedial aspect of arm with surrounding edema s/o granuloma. The patient underwent excision of the cyst and biopsy was suggestive of cysticercosis and surrounding granuloma.
Conclusion: Isolated cysticercosis of muscle is very rare, but when it is symptomatic and hindering in daily activities, surgical excision can be done for faster relief and early return to normal day-to-day activities.
Keywords: Biceps muscle, Cysticercosis.
Introduction
Cysticercosis is mostly seen in developing countries like India. It is caused by the larval stage of Taenia solium [1]. Man is both definitive and intermediate host [1]. Cysticercosis is mostly common in people who consume undercooked pork and live in poor sanitary conditions [2]. Neurocysticercosis is most common disease caused by this parasite and involvement of skeletal muscles is rare [3]. Due to immigration of people from endemic countries carrying Taenia solium, cases are reported in developed countries [4]. There have been cases reported in various skeletal muscles in literature but it is always a diagnostic challenge for the treating doctor due to its varied presentations and with few cases even reported among vegetarians [5].
Case Report
Cysticercosis in developing countries like India is not an uncommon condition. It is caused by larval stage of T. solium [1]. Man is both definitive and intermediate host [1]. Neurocysticercosis is the most common disease caused by this parasite and involvement of skeletal muscles is rare [2]. Cysticercosis is common in people eating undercooked pork and living in poor sanitary conditions [3]. Due to immigration of people from endemic countries carrying T. solium, cases are reported in developed countries [4]. There have been cases reported in various skeletal muscles in literature, but it is always a diagnostic challenge for the treating doctor due to its varied presentations and with few cases even reported among vegetarians [5]. A 32-year-old male, security personnel by occupation, comes to the outpatient department with complaints of painful swelling of the right arm for past 1 week. It was insidious in onset and non-progressive swelling (Fig. 1).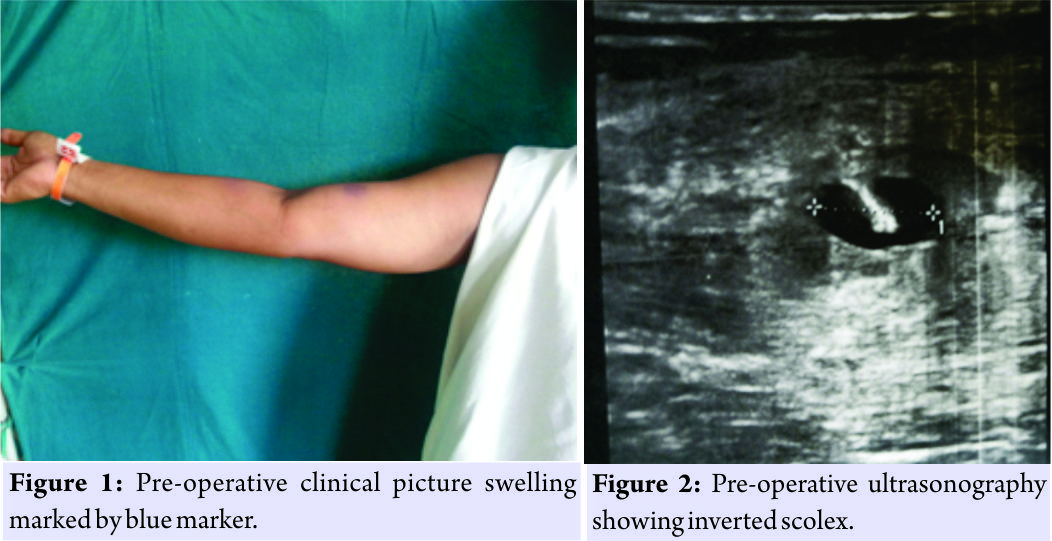 There was no trauma to the limb and no similar swellings elsewhere in the body. Pain increased whenever he use to lift heavy weights or did twisting movements of the arm. Relieved by rest and analgesics. He was a young patient with no comorbidities. He was a non-vegetarian occasional smoker and alcoholic. No similar complaints in the family. On examination, there was an anteromedial swelling of mid-third of arm. No local raise of temperature. Tenderness present. Swelling does not become prominent on contraction of muscle. Skin over the swelling is pinchable. X-ray was normal with soft tissue shadow on the anterior aspect. Ultrasound showed cystic lesion with central hyperechoic lesion suggestive of either granuloma or cysticercosis (Fig. 2). Physician opinion was sought who advised for a magnetic resonance imaging (MRI) scan of brain and fundus examination along with stool examination to r/o cysticercosis elsewhere in the body. All the above-mentioned tests were negative and MRI of arm showed 7.7 mm × 4.8 mm lesion in anteromedial aspect of arm with surrounding edema s/o granuloma (Fig. 3). In view of severe pain, hindrance to his daily activities and as the pathology was localized to only one part of the body it was decided to excise the mass and medical management deferred till biopsy. After taking a written informed consent excision of the cyst was done. Intraoperatively, cyst was found embedded between the muscle fibers (Fig. 4), and it was dissected on table which showed scolex (Fig. 5) and then the cut specimen was sent for histopathological examination. Biopsy showed cysticercus larva lined by palisading histiocytic aggregates and foreign body granuloma. Surrounding inflammatory infiltrate of lymphoplasmacytic cells with eosinophils and histiocytes (Fig. 6). The patient was started on albendazole after biopsy report by physicians to treat if there were any dormant cysts. Family members of the patient were also advised albendazole to eliminate carrier state and prevent recurrence. At 6-month follow-up, the patient is completely asymptomatic and doing all his activities normally as before.
There was no trauma to the limb and no similar swellings elsewhere in the body. Pain increased whenever he use to lift heavy weights or did twisting movements of the arm. Relieved by rest and analgesics. He was a young patient with no comorbidities. He was a non-vegetarian occasional smoker and alcoholic. No similar complaints in the family. On examination, there was an anteromedial swelling of mid-third of arm. No local raise of temperature. Tenderness present. Swelling does not become prominent on contraction of muscle. Skin over the swelling is pinchable. X-ray was normal with soft tissue shadow on the anterior aspect. Ultrasound showed cystic lesion with central hyperechoic lesion suggestive of either granuloma or cysticercosis (Fig. 2). Physician opinion was sought who advised for a magnetic resonance imaging (MRI) scan of brain and fundus examination along with stool examination to r/o cysticercosis elsewhere in the body. All the above-mentioned tests were negative and MRI of arm showed 7.7 mm × 4.8 mm lesion in anteromedial aspect of arm with surrounding edema s/o granuloma (Fig. 3). In view of severe pain, hindrance to his daily activities and as the pathology was localized to only one part of the body it was decided to excise the mass and medical management deferred till biopsy. After taking a written informed consent excision of the cyst was done. Intraoperatively, cyst was found embedded between the muscle fibers (Fig. 4), and it was dissected on table which showed scolex (Fig. 5) and then the cut specimen was sent for histopathological examination. Biopsy showed cysticercus larva lined by palisading histiocytic aggregates and foreign body granuloma. Surrounding inflammatory infiltrate of lymphoplasmacytic cells with eosinophils and histiocytes (Fig. 6). The patient was started on albendazole after biopsy report by physicians to treat if there were any dormant cysts. Family members of the patient were also advised albendazole to eliminate carrier state and prevent recurrence. At 6-month follow-up, the patient is completely asymptomatic and doing all his activities normally as before.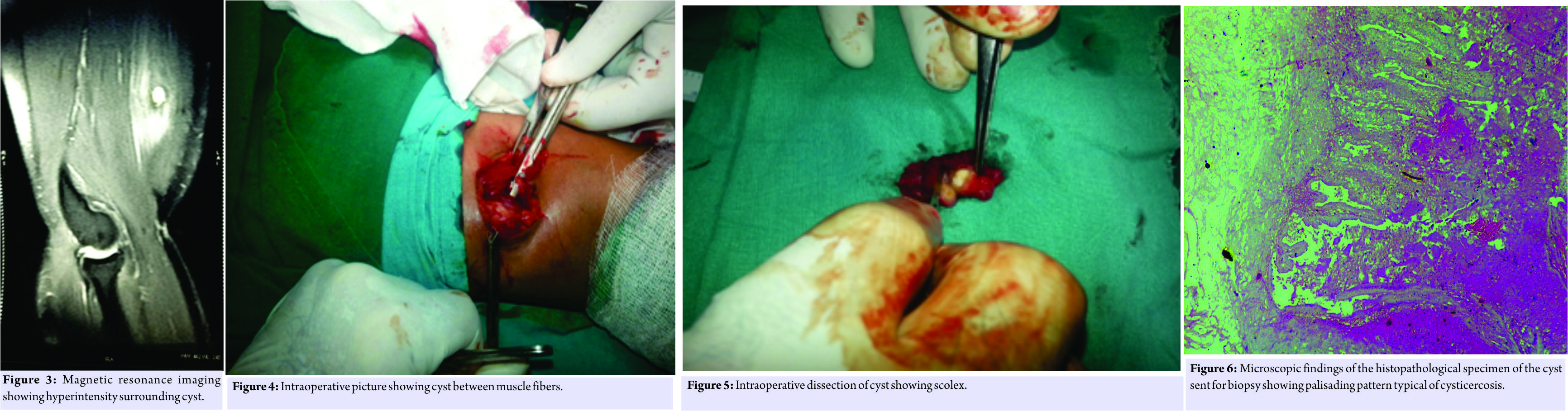
Discussion
There is very few differential diagnosis for an acute painful swelling of arm. Myositis is the most common diagnosis made. Other conditions such as granuloma, abscess, hematoma, hemangioma, and lipoma cannot be ruled out. In our case, as the patient did not had any trauma or fever, it was difficult to make a definitive diagnosis clinically. Only after ultrasonography and MRI differential diagnosis of cysticercosis were made. Review of literature showed sporadic cases of cysticercosis of biceps muscle reported and most of them managed medically. Solitary cyst involvement is more common in India [6]; in our case, since the patient had severe pain and tenderness and difficulty in carrying daily activities, it was decided to excise the mass after discussing with physicians. Skeletal muscle cysts are surgically removed only if painful [7]. Teniasis is associated with 25% of cases of cysticercosis. It should always be ruled out before the diagnosis of isolated cysticercosis is made [8]. Enzyme-linked immunoelectrotransfer blot for detecting specific antibodies is considered to be more specific diagnostic test [9]. Due to unavailability of this test at our center, it could not be done.
Conclusion
In countries like India where people live in places where pigs are reared and sanitary conditions are poor, cysticercosis should be in differential diagnosis of intramuscular swellings. Medical management will cure the disease but if the patient is having severe pain and tenderness with difficulty in carrying daily activities, it is always advisable to excise the cyst, especially when it is solitary. Surgery is one-time procedure with quick results and will give a specific diagnosis. Cysticercosis carries good prognosis if diagnosed and treated. It is important to screen family members if they are carriers and treat them as well. Always educate patient of good hygiene and to eat properly cooked meat.
Clinical Message
The aim of our presentation was to stress on surgical excision for painful swelling where drugs take time and sometimes cause inflammatory reaction which, in turn, can aggravate patient symptoms.
References
1. Garcia HH, Del Brutto OH. Taenia solium cysticercosis. Infect Dis Clin North Am 2000;14:97-119.
2. García HH, Gonzalez AE, Evans CA, Gilman RH, Cysticercosis Working Group in Peru. Taenia solium cysticercosis. Lancet 2003;362:547-56.
3. World Health Organization. Guidelines for Surveillance Prevention and Control of Taeniasis/Cysticercosis WHO Document VPH/83.49. Geneva: World Health Organization; 1983.
4. Schantz PM, Wilkins PP, Tsang VC. In: Scheld WM, Craig WA, Hughes JM, editors. Immigrants, Imaging and Immunoblots: The Emergence of Neurocysticercosis as a Significant Public Health Problem. Emerging Infections 2. Washington, DC: ASM Press; 1998. p. 213-41.
5. Abdelwahab IF, Klein MJ, Hermann G. Solitary cysticercosis of biceps brachii in a vegetarian: A rare and unusual pseudotumor. Skeletal Radiol 2003;32:424-8.
6. Prabhakaran V, Rajshekhar V, Murrell KD, Oommen A. Conformation sensitive immunoassays improve the serodiagnosis of solitary cysticercus granuloma in Indian patients. Trans R Soc Trop Med Hyg 2007;101:570-7.
7. Kraft R. Cysticercosis: An emerging parasitic disease. Am Fam Physician 2007;76:91-6.
8. Schantz PM. Larval cestodiases. In: Hoeprich JD, Jordan MC, Ronald AR, editors. Infectious Diseases. 5th ed. Philadelphia, PA: JB Lippincott; 1994. p. 850-60.
9. Richards FO Jr., Schantz PM. Laboratory diagnosis of cysticercosis. Clin Lab Med 1991;11:101-28.
 |
 |
 |
| Dr. Manesh Kumar Jain | Dr. Surendra Umesh Kamath | Dr. Flora Lobo |
| How to Cite This Article: Jain M K , Kamath S U , Lobo F. A Case Report of Isolated Cysticercosis of Biceps Muscle. Journal of Orthopaedic Case Reports 2018. May-June; 8(3): 89-91. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


