
[box type=”bio”] Learning Point for the Article: [/box]
A high index of clinical suspicion for lipofibromatous hamartoma is crucial in patients presenting with painless masses combined with acute compression
neuropathy.
Case Report | Volume 8 | Issue 4 | JOCR July – August 2018 | Page 57-60| Dimitrios Kitridis, Panagiotis Dionellis, Konstantinos Xarchas, Panagiotis Givissis. DOI: 10.13107/jocr.2250-0685.1160
Authors: Dimitrios Kitridis[1], Panagiotis Dionellis[2], Konstantinos Xarchas[3], Panagiotis Givissis[4]
[1]Department of Orthopaedics, 424 General Military Hospital, Thessaloniki. Greece.
[2]Department of Orthopaedics, Hippokration Hospital, Thessaloniki. Greece.
[3]Department of Orthopaedics, General Hospital Georgios Gennimatas, Athens.Greece.
[4]Department of Orthopaedics, Aristotle University of Thessaloniki, George Papanikolaou Hospital, Thessaloniki. Greece.
Address of Correspondence:
Dr. Dimitrios Kitridis,
Department ofOrthopaedic, 424 General Military Hospital, 1st Thessaloniki, Greece.
E-mail: dkitridis@gmail.com
Abstract
Introduction: Lipofibromatous hamartoma (LFH) is a very rare, benign, slow-growing peripheral nerve tumor.
Case Report: We present a case of LFH of the median nerve, which caused enlargement of the median nerve and the digital branches in a young male, and was treated surgically. Our treatment choice was resection of large portions of the fibrofatty tissue and decompression of the carpal tunnel.
Conclusion: A high index of suspicion for LFH is crucial in patients presenting with painless masses combined with acute compression neuropathy.
Keywords: Acute compression neuropathy, fibrolipomatous hamartoma, median nerve.
Introduction
Lipofibromatous hamartoma (LFH) is a very rare, benign, slow-growing peripheral nerve tumor first reported by Mason, in 1953 [1, 2, 3, 4, 5]. Fewer than 100 cases have been reported for this rare condition [1]. The cause of LFH remains obscure; however, commonly proposed etiologies are congenital malformation and chronic micro trauma [1, 2]. LFH preferentially affects the median nerve(about 80% of the cases), especially in the carpal tunnel segment [1, 2, 4]. Macrodactyly is present in about one-third of the cases [1, 2]. Involvement of the brachial plexus, radial, and ulnar nerves, as well as their branches in the upper extremity, and sciatic, peroneal, and plantar nerves in the lower extremity has also been described [2, 6]. Due to the rarity of the cases, many modalities exist for treating LFH, with no clear consensus. In this case report, we present a rare case of LFH of the median nerve, which caused enlargement to the median nerve and the digital branches in a young male, and was treated surgically.
Case Report
A 15-year-old boy presented with a 10-year history of pain, deteriorating sensory and motor deficits at the right median nerve distribution. Clinically, a soft, non-tender, 6 cm (proximally to distally) – 3 cm (medially to laterally) fusiform subcutaneous mass was apparent over the right thenar eminence (Fig. 1). The thenar intrinsic muscles innervated by the median nerve were weak; abductor pollicis brevis, opponens pollicis, and flexor pollicis brevis muscle power using the Medical Research Council scale were 3/5. Tinel’s sign and Phalen’s test were both positive. Nerve conduction studies showed dramatically diminished amplitude and motor latency prolongation in the median nerve. The ulnar nerve was unaffected. Radiographs of the hand and wrist did not show bony abnormalities (Fig. 2).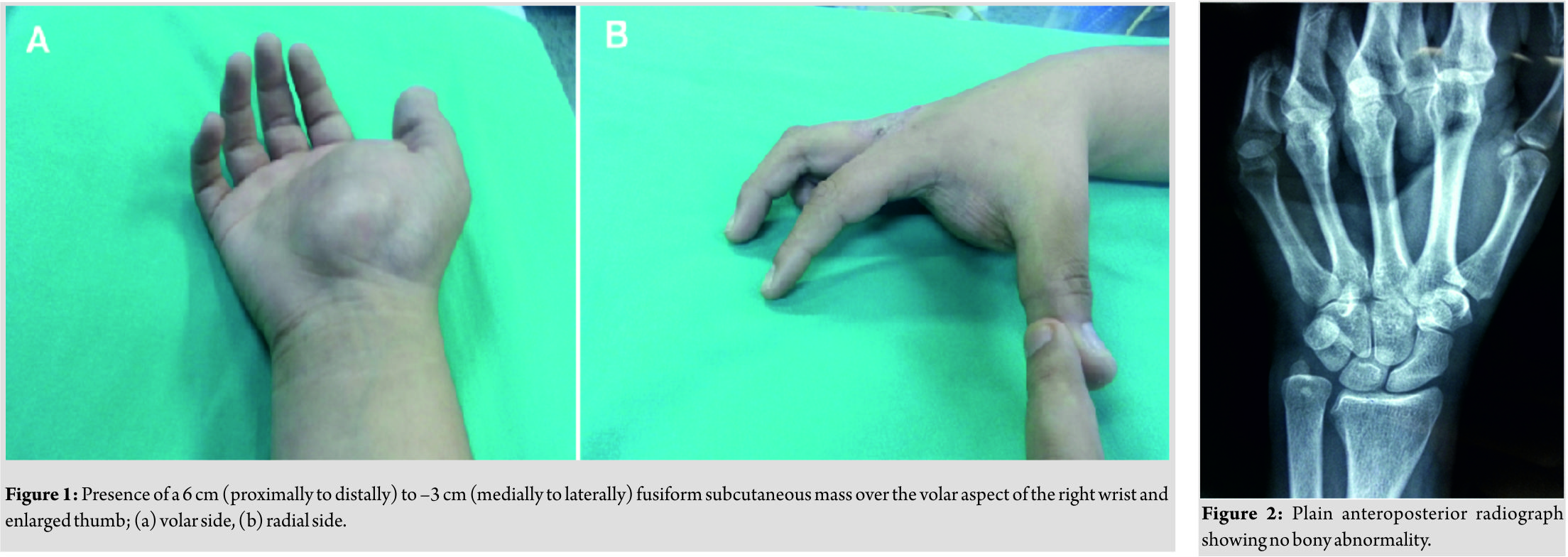 The ultrasound and magnetic resonance imaging (MRI) scan revealed excessive median nerve enlargement, with a “coaxial cable-like” appearance in the axial plane, and a “spaghetti-like” appearance with lipofibromatous tissue interspersed between the bundles of the nerve in the coronal plane (Fig. 3).After an open biopsy, histopathology reported non-neoplastic fibrofatty elements infiltrating the perineurium with mature fibrous and adipose tissue separating nerve fascicles, creating an “onion bulb-like appearance,” and the diagnosis of LFH was made (Fig. 4).
The ultrasound and magnetic resonance imaging (MRI) scan revealed excessive median nerve enlargement, with a “coaxial cable-like” appearance in the axial plane, and a “spaghetti-like” appearance with lipofibromatous tissue interspersed between the bundles of the nerve in the coronal plane (Fig. 3).After an open biopsy, histopathology reported non-neoplastic fibrofatty elements infiltrating the perineurium with mature fibrous and adipose tissue separating nerve fascicles, creating an “onion bulb-like appearance,” and the diagnosis of LFH was made (Fig. 4).

Surgical exploration and decompression of the carpal tunnel were decided. After a combined anterior distal forearm and palmar approach, both median nerve trunk and digital branches were found gigantic, infiltrated by fatty tissue (Fig. 5 and 6).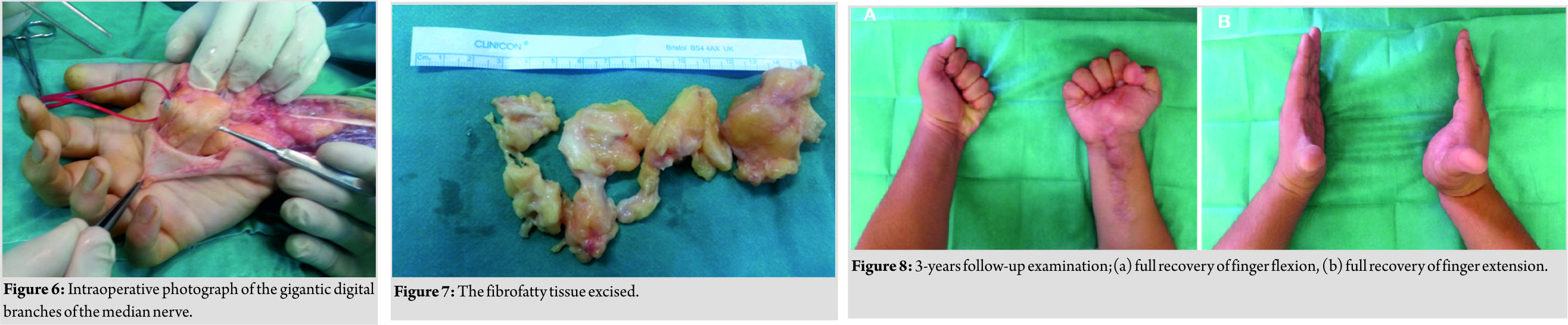 A careful excision of fatty tissue was performed under magnification, preserving the median nerve (Fig. 7). The final biopsy confirmed the diagnosis. The post-operative period was uneventful and the patient had a complete resolution of his symptoms. At the 3-year follow-up, he remained asymptomatic (Fig. 8). The hand strength measurements and the disabilities of the arm, shoulder and hand score are presented in (Tab. 1).
A careful excision of fatty tissue was performed under magnification, preserving the median nerve (Fig. 7). The final biopsy confirmed the diagnosis. The post-operative period was uneventful and the patient had a complete resolution of his symptoms. At the 3-year follow-up, he remained asymptomatic (Fig. 8). The hand strength measurements and the disabilities of the arm, shoulder and hand score are presented in (Tab. 1).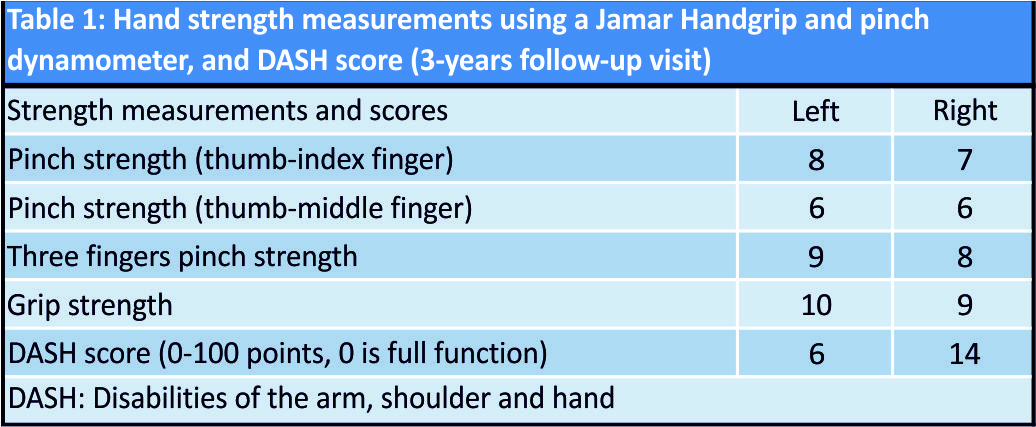
LFH was first described by Mason, in 1953 [5], and then reported by Emmett as hamartoma in 1965 [7]. The term LFH was established in 1969 by Johnson and Bonfiglio[4]. This rare condition is characterized by infiltration of peripheral nerves by fibrous and adipose tissues. Several names have been used to describe it including fibrolipomatous hamartoma, fibrolipoma, lipofibroma, fibrofatty proliferation, macrodystrophialipomatosa, and intraneural lipoma[1]. The lack of a single name, along with its rarity, has complicated the diagnosis and the treatment of this condition[2]. LFH is most commonly found in the median nerve (about 80% of the cases), especially in the carpal tunnel segment, although it is unknown why this predilection occurs[4]. LFH is the most common condition associated with macrodactyly of the upper extremity; in one-third of the cases reported, macrodactyly is noted in the distal distribution of the involved nerve [1, 2]. Male and female patients appear to be equally affected with a mean age of 21 years old [2]. Although the cause of LFH remains unknown, the early age onset has led several physicians to support that LFH is a congenital tumor[1, 2]. Other authors support that a history of trauma before on set or chronic microtrauma due to repetitive pressure to the median nerve from the carpal ligament or from an abnormally developing flexor retinaculum contribute to LFH development [8-10]. Our case did not have a history of trauma before onset. LFH of the median nerve most commonly presents as an enlarging, minimally tender, soft, and non-fluctuant mass, which is located on the course of the nerve. Signs and symptoms of carpal tunnel syndrome are often noted. Sensory and motor deficit are also reported, especially on chronic cases [4, 8, 9].The clinical differential diagnosis includes neurofibroma, neurilemoma, neuroma, ganglion, lipoma, or vascular malformation, among others. However, there are no physical findings that are pathognomonic for distinguishing LFH from other lesions [11]. MRI scan is considered the best diagnostic tool [1]. On the axial plane, the nerve is enlarged and has a “coaxial cable-like” appearance, while a “spaghetti-like” appearance is found on coronal and sagittal planes. Low-intensity signal nerve bundles are embedded in high-intensity fat on both T1-weighted and T2-weighted images. These features are pathognomonic for LFH [12, 13]. Similar features were found in the MRI scan of our patient (Fig. 4). However, the only definite mean of the diagnosis remains the histopathological examination [2]. Macroscopically, the tumor has the appearance of a yellow or tan mass composed of the nerve with fibrofatty strands which are inserted in the epineurium. Microscopically, fibrofatty elements of the tumor invade the peri- and endoneurium, separating the individual nerve fibers or group of fibers. An “onion bulb-like appearance” is seen due to increased perineurial cells and perineurial fibrosis [9, 14]. In our case, non-neoplastic fibrofatty elements infiltrated the perineurium with mature fibrous and adipose tissue separating nerve fascicles, creating this “onion bulb-like appearance” (Fig. 5). Electromyogram and nerve conduction studies are abnormal, often showing decreased conduction and findings of compression neuropathy [2]. There is no consensus regarding the appropriate treatment, as the rarity of the tumor precludes high-quality studies identifying optimal treatment protocols[2]. Conservative treatment is reserved for asymptomatic patients, with follow-up observation [11]. When surgical treatment is chosen, the insertion of fibrofatty tissue within the nerve fascicles makes the complete excision of the tumor very challenging. One option of surgical treatment is the complete excision of the tumor, which can be achieved only at the cost of sacrificing the nerve. It is not commonly performed, because it has the disadvantage of various degrees of neural deficit[2, 9, 14, 15]. Another option is the excision of the transverse carpal ligament to treat carpal tunnel syndrome, with satisfactory results[1, 2, 3]. This approach may not only alleviate the pain but also decrease the size of the mass and demonstrate improvement in the strength of opponens pollicis. Finally, the resection of large portions of the fibrofatty tissue and decompression of the median nerve, with careful preservation of the median nerve using microsurgical techniques, has even more positive results[4]. Due to the rarity of the entity, the treatment of LFH is guided by the severity of the symptoms on a case-by-case basis. Clinicians must have a high index of suspicion for LFH in patients presenting with painless masses combined with acute compression neuropathy. The diagnosis is guided by pathognomonic MRI and histopathological images. The hand surgeon must be aware of the treatment options, choosing conservative management in asymptomatic patients, and microsurgical exploration in the case of neurological deficits.
Conclusion
We present a rare case of LFH, which caused an enlargement of the median nerve and the digital branches in a young male, and was treated surgically. Our treatment choice was resection of large portions of the fibrofatty tissue and decompression of the carpal tunnel. A high index of clinical suspicion for LFH is crucial in patients presenting with painless masses combined with acute compression neuropathy. Therefore, increased clinical awareness of this condition by clinicians, radiologists, and pathologists is vital for the best treatment management.
Clinical Message
Lipofibromatous Hamartoma is a rare benign peripheral nerve tumour, which can cause gigantism of the median nerve. A high index of clinical suspicion for hamartoma is crucial in patients presenting with painless masses combined with acute compression neuropathy.
References
1. Agarwal S, Haase SC. Lipofibromatous hamartoma of the median nerve. J Hand Surg Am2013;38:392-7.
2. Tahiri Y, Xu L, Kanevsky J, Luc M. Lipofibromatous hamartoma of the median nerve: A comprehensive review and systematic approach to evaluation, diagnosis, and treatment. J Hand Surg Am 2013;38:2055-67.
3. Al-Qattan MM. Lipofibromatous hamartoma of the median nerve and its associated conditions. J Hand Surg Br2001;26:368-72.
4. Johnson RJ, Bonfiglio M. Lipofibromatous hamartoma of the median nerve. J Bone Joint Surg Am1969;51:984-90.
5. Mason ML. Presentation of cases: Proceedings of the american society for surgery of the hand. J Bone Joint Surg Am1953;35A:273-4.
6. Steentoft J, Sollerman C. Lipofibromatous hamartoma of a digital nerve. A case report. Acta OrthopScand1990;61:181-2.
7. Emmett AJ. Lipomatous hamartoma of the median nerve in the palm. Br J Plast Surg 1965;18:208-13.
8. Kameh DS, Perez-Berenguer JL, Pearl GS. Lipofibromatous hamartoma and related peripheral nerve lesions. South Med J 2000;93:800-2.
9. Warhold LG, Urban MA, Bora FW, Jr., Brooks JS, Peters SB. Lipofibromatous hamartomas of the median nerve. J Hand Surg Am1993;18:1032-7.
10. Aslan A, Konya MN, Sargin S. Post-traumatic median nerve neuroma in wrist. A Case report and brief review of literature. J Orthop Case Rep 2013;3:38-41.
11. Senger JL, Classen D, Bruce G, Kanthan R. Fibrolipomatous hamartoma of the median nerve: A cause of acute bilateral carpal tunnel syndrome in a three-year-old child: A case report and comprehensive literature review. Plast Surg (Oakv) 2014;22:201-6.
12. Toms AP, Anastakis D, Bleakney RR, Marshall TJ. Lipofibromatous hamartoma of the upper extremity: A review of the radiologic findings for 15 patients. AJR Am J Roentgenol2006;186:805-11.
13. Marom EM, Helms CA. Fibrolipomatous hamartoma: Pathognomonic on MR imaging. Skeletal Radiol1999;28:260-4.
14. Silverman TA, Enzinger FM. Fibrolipomatous hamartoma of nerve. A clinicopathologic analysis of 26 cases. Am J Surg Pathol1985;9:7-14.
15. Patel ME, Silver JW, Lipton DE, Pearlman HS. Lipofibroma of the median nerve in the palm and digits of the hand. J Bone Joint Surg Am1979;61:393-7.
 |
 |
 |
 |
| Dr. Dimitrios Kitridis | Dr. Panagiotis Dionellis | Dr. Konstantinos Xarchas | Dr. Panagiotis Givissis |
| How to Cite This Article: KitridisD, DionellisP, XarchasK, GivissisP. Giant Median Nerve Due to Hamartoma Causing Severe Carpal Tunnel Syndrome. Journal of Orthopaedic Case Reports 2018 Jul-Aug; 8(4): 57-60. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


