
[box type=”bio”] Learning Point of the Article: [/box]
Traumatic tears of the infraspinatus in young athletes can be managed successfully with return to sport after arthroscopic repair.
Case Report | Volume 9 | Issue 3 | JOCR May-June 2019 | Page 7-10 | Sean Fitzpatrick, Alan W Reynolds, Gregory Purnell. DOI: 10.13107/jocr.2250-0685.1394
Authors: Sean Fitzpatrick[1], Alan W Reynolds[1], Gregory Purnell[1]
[1]Department of Orthopaedics, Allegheny General Hospital, Pittsburgh, Pennsylvania, United States.
Address of Correspondence:
Dr. Gregory Purnell,
Federal North Building, 1307 Federal St, Pittsburgh, Pennsylvania, 15212, United States.
E-mail: Gregory.Purnell@AHN.org
Abstract
Introduction: Young, athletic patients who suffer a traumatic rotator cuff tear often have high expectations for returning to their pre-injury level of physical ability. Rotator cuff injuries in adolescent and young adults are rare injuries. Isolated tears of the infraspinatus tendon are ever more rare with only one other case being previously reported in literature.
Case Report: We present the case of a full-thickness rotator cuff tear isolated to the infraspinatus tendon in an 18-year-old quarterback. The patient underwent arthroscopic fixation and has returned to pre-injury level of function.
Conclusion: This case presents the rare injury of an isolated infraspinatus tear and demonstrates that with subsequent treatment the patient was able to return to pre-injury level of function. General arthroscopic techniques and rehabilitation protocols used for rotator cuff tears in young patients can be applied to successfully manage traumatic tears of the infraspinatus.
Keywords: Rotator cuff, Infraspinatus, Shoulder, Arthroscopy.
Introduction
Full-thickness rotator cuff tears in young patients are uncommon injuries, usually resulting from an acute traumatic event. These injuries require prompt diagnosis and appropriate management to prevent long-term shoulder dysfunction and disability. In addition, the population of young patients who suffer these injuries often have high expectations regarding their post-injury outcomes and place high physical demands on their repaired tendons [1]. Although outcomes in these patients have been reported, most injury patterns described involve the supraspinatus tendon [1, 2, 3]. Isolated injuries of the infraspinatus are very uncommon and to our knowledge have only been previously reported on once [4]. This report details successful repair and rehabilitation of such an injury to a football quarterback, allowing return to unrestricted high demand physical activities.
Case Report
A healthy 18-year-old right-hand dominant male presented to clinic 5 days after injuring his left shoulder during a high school football game. The patient reported landing directly on his left shoulder after being tackled. He noted immediate pain and inability to move his left shoulder. On-site athletic training staff removed him from play and placed him into a sling. This was an injury to his non-throwing arm. At his initial evaluation 5 days after his injury, he continued to have severe pain and limited motion. He denied any previous shoulder injury. Examination was limited due to guarding. Clinically, he had significant ecchymosis about the upper arm and tenderness to palpation throughout the proximal shoulder. Active forward elevation was limited to 60°. He had weakness with posterior rotator cuff testing. There were no appreciable signs of instability on examination. Plain radiographs including anteroposterior, axillary lateral, and outlet views of the shoulder were obtained in office and demonstrated no evidence of acute fracture or dislocation. There was no evidence of Hill-Sachs deformity. The patient was sent for magnetic resonance arthrogram (MRA) to further evaluate his injury. 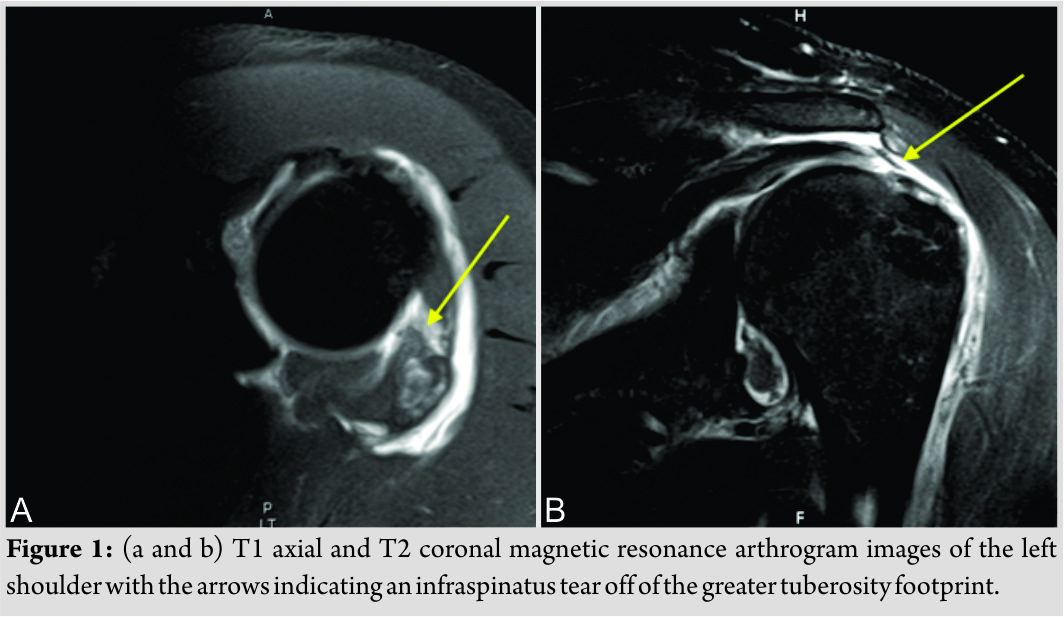 MRA (Fig. 1 A and B) demonstrated a full-thickness tear of the infraspinatus with minimal retraction. The supraspinatus and subscapularis were intact. No biceps or labral pathology was identified. After discussing options with the patient and his family, the decision was made to proceed with arthroscopic rotator cuff repair. Ten days after sustaining his injury, the patient was taken to the operating room. Preoperatively, the patient received an interscalene block and general endotracheal anesthesia was administered. The patient was then placed in the lateral decubitus position with 10 pounds of traction applied to the shoulder. A standard posterior portal was created and a 30° arthroscope was inserted into the glenohumeral joint. Copious hemarthrosis was evacuated from the joint. The anterior labrum, superior labrum, biceps, and subscapularis showed no evidence of injury. A full-thickness tear of the infraspinatus was confirmed while viewing from the articular side. Visualization from the lateral portal confirmed the massive mid substance “L”-shaped tear of the entire infraspinatus tendon (Fig. 2). A knotless, speed bridge double-row construct was performed to repair the tendons after debridement of the free tendon edges and tendon footprint. Two 4.75 mm SwiveLock anchors loaded with Fiber Tape (Arthrex, Naples, Florida [FL]) were placed just lateral to the articular margin, one anterior and one posterior on the footprint. The tape-type sutures were passed in a horizontal mattress fashion through the tendon. An additional Fiber Link (Arthrex, Naples, FL) was passed through the most posterior aspect of the infraspinatus tendon. The lateral row was then created with two additional 4.75 mm SwiveLock anchors (Arthrex, Naples, FL). Visualization from the lateral portal confirmed an excellent restoration of the tendon to the footprint following repair (Fig. 3).
MRA (Fig. 1 A and B) demonstrated a full-thickness tear of the infraspinatus with minimal retraction. The supraspinatus and subscapularis were intact. No biceps or labral pathology was identified. After discussing options with the patient and his family, the decision was made to proceed with arthroscopic rotator cuff repair. Ten days after sustaining his injury, the patient was taken to the operating room. Preoperatively, the patient received an interscalene block and general endotracheal anesthesia was administered. The patient was then placed in the lateral decubitus position with 10 pounds of traction applied to the shoulder. A standard posterior portal was created and a 30° arthroscope was inserted into the glenohumeral joint. Copious hemarthrosis was evacuated from the joint. The anterior labrum, superior labrum, biceps, and subscapularis showed no evidence of injury. A full-thickness tear of the infraspinatus was confirmed while viewing from the articular side. Visualization from the lateral portal confirmed the massive mid substance “L”-shaped tear of the entire infraspinatus tendon (Fig. 2). A knotless, speed bridge double-row construct was performed to repair the tendons after debridement of the free tendon edges and tendon footprint. Two 4.75 mm SwiveLock anchors loaded with Fiber Tape (Arthrex, Naples, Florida [FL]) were placed just lateral to the articular margin, one anterior and one posterior on the footprint. The tape-type sutures were passed in a horizontal mattress fashion through the tendon. An additional Fiber Link (Arthrex, Naples, FL) was passed through the most posterior aspect of the infraspinatus tendon. The lateral row was then created with two additional 4.75 mm SwiveLock anchors (Arthrex, Naples, FL). Visualization from the lateral portal confirmed an excellent restoration of the tendon to the footprint following repair (Fig. 3).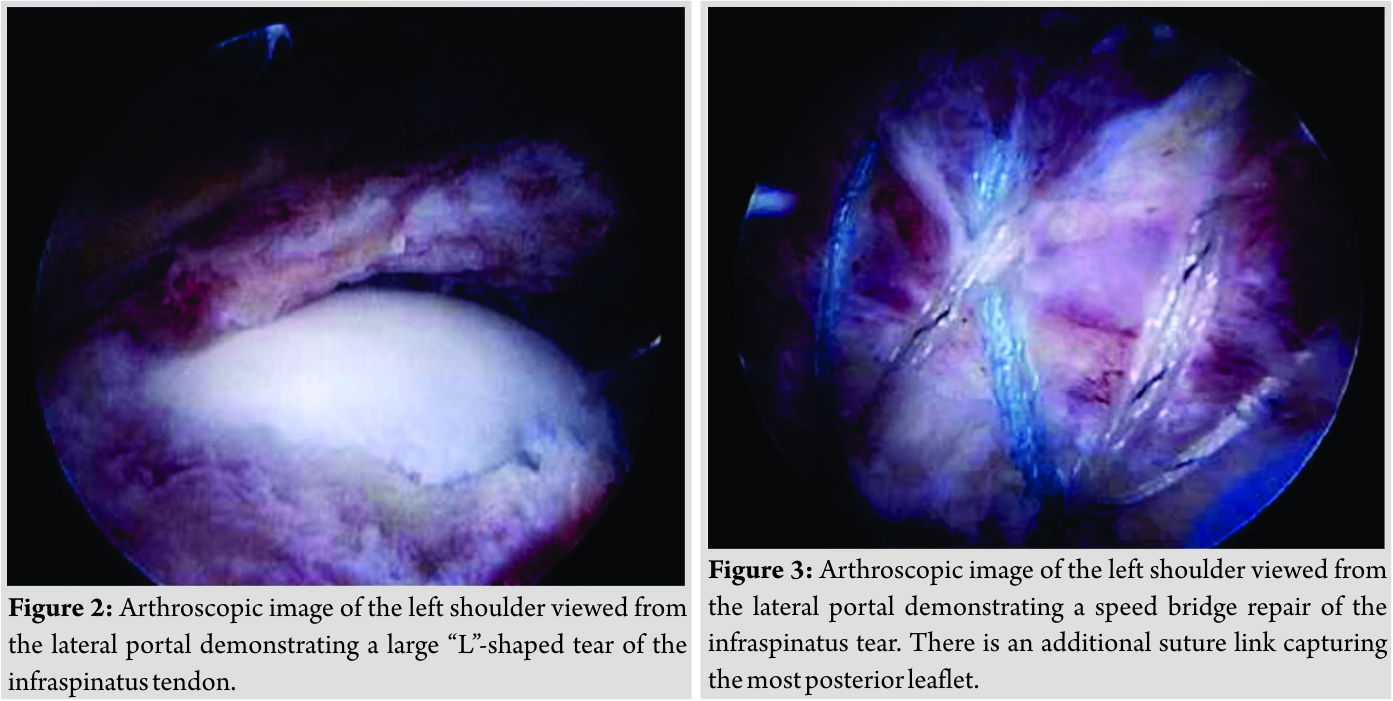 Skin closure was performed in a normal fashion, and the patient was then placed in an abduction sling following the arthroscopic repair. Routine care was provided postoperatively. Physical therapy was initiated at 1 week postoperatively. The sling was discontinued 6 weeks after surgery. At 5 months following his repair, his range of motion was normalized. He demonstrated forward elevation of 180°, lateral abduction of 180°, and external rotation at neutral of 70°. Strength assessment with Jobe’s testing and external rotation testing at neutral revealed no clinical difference compared to the uninjured shoulder. At the final 18-month follow-up, clinical strength and motion testing were equal to his uninjured shoulder. While the patient had no intentions of playing college football, he was able to return to weight training and playing recreational ice hockey.
Skin closure was performed in a normal fashion, and the patient was then placed in an abduction sling following the arthroscopic repair. Routine care was provided postoperatively. Physical therapy was initiated at 1 week postoperatively. The sling was discontinued 6 weeks after surgery. At 5 months following his repair, his range of motion was normalized. He demonstrated forward elevation of 180°, lateral abduction of 180°, and external rotation at neutral of 70°. Strength assessment with Jobe’s testing and external rotation testing at neutral revealed no clinical difference compared to the uninjured shoulder. At the final 18-month follow-up, clinical strength and motion testing were equal to his uninjured shoulder. While the patient had no intentions of playing college football, he was able to return to weight training and playing recreational ice hockey.
Discussion
To the best of our knowledge, there have only been two reported cases of full-thickness tears of the infraspinatus tendon following an acute traumatic event in the young athlete [4, 5]. Only one of these cases was an isolated injury to the infraspinatus tendon. Both patients had sustained injuries during contact football play and subsequently underwent arthroscopic repair. Cain et al. published a case of a 23-year-old male professional football player who sustained a full-thickness tear of the infraspinatus tendon and partial thickness tear of the teres minor tendon during football [4]. This injury occurred after the patient dove for a pass landing on an outstretched arm. Physical examination was positive for rotator cuff pathology. A full-thickness tear of the infraspinatus tendon and partial tear of the teres minor tendon were revealed on MRA study. Diagnostic arthroscopic evaluation confirmed the tear and repair of the rotator cuff tear was performed using a combination of arthroscopic and open techniques. Following 9 months of rehabilitation, the patient returned to playing professional football. Brown et al. published a case of an 18 years old high school quarterback who sustained a massive infraspinatus tear and reverse humeral avulsion of the glenohumeral ligament (RHAGL) [5]. The injury occurred after he was tackled from behind with his arm in the throwing position. Physical examination was positive for posterior shoulder instability and rotator cuff injury. A complete tear of the infraspinatus tendon and RHAGL lesion was demonstrated on MRA. Arthroscopic evaluation confirmed the injury and repair was performed. 12 months following repair, the patient had returned to pre-injury throwing velocity and endurance. There are two important factors that contribute to outcomes in young patients that must be considered when making treatment decisions regardless of which tendons are involved: The increased healing potential of young patients as well as the increased demand and expectations of younger patients. Numerous studies have demonstrated higher rates of healing in younger patients with a rotator cuff injury when compared to older patients [6, 7, 8]. This is believed to be due to the fact that younger patients have increased vascularity within the rotator cuff tendon compared to older patients [9]. Boileau et al. evaluated tendon healing following arthroscopic repair of supraspinatus tears with computed tomography arthrogram or MRI [10]. Their results demonstrated 95% healing rates for patients younger than 55 years while healing in patients older than 55 years was only 58%. It is also important to keep in mind that younger patients often have higher functional demands that can adversely affect their subjective and functional outcomes [1]. A retrospective review by Hawkins et al. demonstrated that only 50% of patients under the age of 40 who had undergone rotator cuff repair returned to sport [2]. However, Krishnan et al. published results that differed from those reported by Hawkins et al. They found that the majority of patients younger than 40 years of age who underwent arthroscopic fixation of acute full-thickness rotator cuff tears had excellent results [3]. Furthermore, they demonstrated that 90% of these patients were found to return to their previous level of function and 100% (3/3) of professional athletes returned to sport.
Conclusion
Treatment of acute, full-thickness rotator cuff tears in a young population presents unique opportunities and challenges. While the healing potential of these patients is great, exceptional results must be achieved to meet the demands and expectations of these patients. In general, good-to-excellent results have been reported for such patients who suffer acute, traumatic tears of the supraspinatus tendon. This case report adds to the body of literature that details successful repair and return of high demand function for a young athlete with an isolated full-thickness tear of the infraspinatus.
Clinical Message
Isolated, full-thickness tears of the infraspinatus are very uncommon but can occur traumatically in young athletes. These patients have high demands and expectations for their recovery, which can be met successfully with prompt diagnosis and careful repair.
References
1. Lazarides AL, Alentorn-Geli E, Choi JH, Stuart JJ, Lo IK, Garrigues GE, et al. Rotator cuff tears in young patients: A different disease than rotator cuff tears in elderly patients. J Shoulder Elbow Surg 2015;24:1834-43.
2. Hawkins RJ, Morin WD, Bonutti PM. Surgical treatment of full-thickness rotator cuff tears in patients 40 years of age or younger. J Shoulder Elbow Surg 1999;8:259-65.
3. Krishnan S, Harkins D, Schiffern S, Pennington S, Burkhead W. Arthroscopic repair of full-thickness tears of the rotator cuff in patients younger than 40 years. Arthroscopy 2008;24:324-8.
4. Cain E, Andrachuk J, Wilk K. Traumatic full-thickness infraspinatus and teres minor tendon tears. J Orthop Sports Phys Ther 2013;43:583.
5. Brown T, Barton S, Savoie F. Reverse humeral avulsion glenohumeral ligament and infraspinatus rupture with arthroscopic repair. Am J Sports Med 2007;35:2135-9.
6. Moraiti C, Valle P, Maqdes A, Boughebri O, Dib C, Giakas G, et al. Comparison of functional gains after arthroscopic rotator cuff repair in patients over 70 years of age versus patients under 50 years of age: A prospective multicenter study. Arthroscopy 2015;31:184-90.
7. Fermont AJ, Wolterbeek N, Wessel RN, Baeyens JP, de Bie RA. Prognostic factors for successful recovery after arthroscopic rotator cuff repair: A systematic literature review. J Orthop Sports Phys Ther 2014;44:153-63.
8. Iyengar J, Porat S, Burnett K, Marrero-Perez L, Hernandez V, Nottage, W. Magnetic resonance imaging tendon integrity assessment after arthroscopic partial-thickness rotator cuff repair. Arthroscopy 2011;27:306-13.
9. Adler RS, Fealy S, Rudzki JR, Kadrmas W, Verma NN, Pearle A, et al. Rotator cuff in asymptomatic volunteers: Contrast-enhanced US depiction of intratendinous and peritendinous vascularity. Radiology 2008;248:954-61.
10. Boileau P, Brassart N, Watkinson DJ, Carles M, Hatzidakis AM, Krishnan SG. Arthroscopic repair of full-thickness tears of the supraspinatus: Does the tendon really heal? J Bone Joint Surg Am 2005;87:1229-40.
 |
 |
 |
| Dr. Sean Fitzpatrick | Dr. Alan W Reynolds | Dr. Gregory Purnell |
| How to Cite This Article: Fitzpatrick S, Reynolds AW, Purnell G. Arthroscopic Repair of an Isolated Infraspinatus Tear in a Contact Athlete: A Case Report. Journal of Orthopaedic Case Reports 2019 May-June; 9(3): 7-10. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


