
[box type=”bio”] Learning Point of the Article: [/box]
Mandible locking plate becomes one of the treatment options for fractures or non-unions in patients with OI because this plate is easy to bend and suitable for the patient’s short bone transverse diameter, severe deformity, and fragility bone.
Case Report | Volume 9 | Issue 3 | JOCR May-June 2019 | Page 19-21 | Shohei Sano, Keisuke Oe, Tomoaki Fukui, Shinya Hayashi, Ryosuke Kuroda, Takahiro Niikura. DOI: 10.13107/jocr.2250-0685.1400
Authors: Shohei Sano[1], Keisuke Oe[1], Tomoaki Fukui[1], Shinya Hayashi[1], Ryosuke Kuroda[1], Takahiro Niikura[1]
[1]Department of Orthopaedic Surgery, Kobe University Graduate school of Medicine, 7-5-1 Kusunoki-Cho, Chuo-Ku, Kobe 650-0017, Japan.
Address of Correspondence:
Dr. Takahiro Niikura,
Department of Orthopaedic Surgery, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-Cho, Chuo-Ku, Kobe 650-0017, Japan.
E-mail: tniikura@med.kobe-u.ac.jp
Abstract
Introduction: Osteogenesis imperfecta (OI) is a heritable disorder of connective tissue. Due to poor bone quality, patients with OI develop bone fracture and subsequent non-union at high rates. We report the rare case of humeral shaft non-union successfully treated by a locking plate used for mandibular bone in a patient with OI.
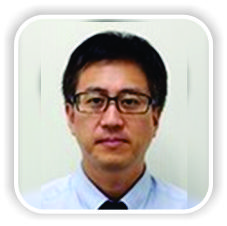
Case Report: A 26-year-old man with Type III OI and a history of corrective osteotomy with Kirschner wire fixation of his right humerus at the age of 8 years developed gradually increasing pain in his humerus. He sustained humeral shaft non-union due to a broken Kirschner wire used in the previous operation and was referred to our hospital. He underwent internal fixation using an elastic nail with an iliac bone graft. However, 2 years after the operation, bony union was not achieved due to elastic nail breakage, and he complained of pain and activity limitation. He underwent re-operation for the humeral non-union using a locking plate to achieve rigid fixation. Because his humeral shaft was extremely narrow with severe deformity, we used a locking plate for the mandibular bone, which was contoured to fit the medial side of the humeral shaft. Bony union was achieved, the pain was relieved, and the patient returned to his pre-injury activity with no symptoms. 4 years after the operation, a new fracture line was found in radiographs of the distal part of the non-union. Bony union was achieved by conservative treatment. At present, the function has recovered.
Conclusion: Humeral non-union in this patient with OI was successfully treated by a mandible locking plate. Although the optimal fixation device for fractures or non-unions in patients with OI has not yet been established, this plate could be a good treatment option for narrow and severely deformed bone.
Keywords: Humeral shaft non-union, osteogenesis imperfecta, mandible locking plate.
Introduction
Osteogenesis imperfecta (OI) is a heritable disorder caused by defective type I collagen synthesis. In 90% of affected patients, a dominant mutation in one of the two genes (COL1A1/2) encoding the α-chains of Type I collagen is responsible [1]. OI occurs in about 1 in 10,000–20,000 live births [2]. Using the Sillence classification, the type of OI can be determined based on clinical, radiographic, and genetic findings [3]. Due to poor bone quality, patients with OI experience high rates of bone fracture and non-union. The treatment of such fractures is difficult, and the treatment of non-union is even more challenging. When treating OI non-union, selection of the optimal material for fixation is difficult due to bone fragility and deformity. Here reports the rare case of humeral shaft non-union successfully treated by a locking plate in the mandibular bone in a patient with OI.
Case Report
A 26-year-old man with Type III OI and a history of correction osteotomy and intramedullary Kirschner wire fixation in his right humerus at the age of 8 years felt gradually increasing pain in his humerus. His left upper limb and both lower limbs were not functional, and he lived in an electric wheelchair. He was unable to manually operate the wheelchair and instead moved it with a switch using his right hand. His right upper limb was his only functional extremity. He had developed humeral shaft non-union due to a broken Kirschner wire used in the previous operation. He was referred to our hospital and underwent internal fixation using an intramedullary elastic nail with an autogenous iliac bone graft. However, 2 years after the operation, bony union was not achieved and elastic nail breakage had occurred, and he complained of pain and limitation of activity (Fig. 1). He underwent a re-operation for his humeral non-union using a locking plate to achieve rigid fixation. Since his humeral shaft was extremely narrow with severe deformity, we used a locking plate for the mandibular bone, which was contoured to fit the medial side of the humeral shaft (Fig. 2). Bony union was achieved, and he became free from pain and returned to his pre-injury activity with no symptoms. No implant failure or refracture of his humeral shaft had occurred 4 years later, but a new fracture line was found in radiographs of the distal part of the non-union (Fig. 3). We used a cast to fix the new fracture for 9 weeks and then a splint for 4 weeks.He recovered well, and at the time of this writing, he was maintaining normal function of the right upper limb and was able to perform activities of daily life without problems.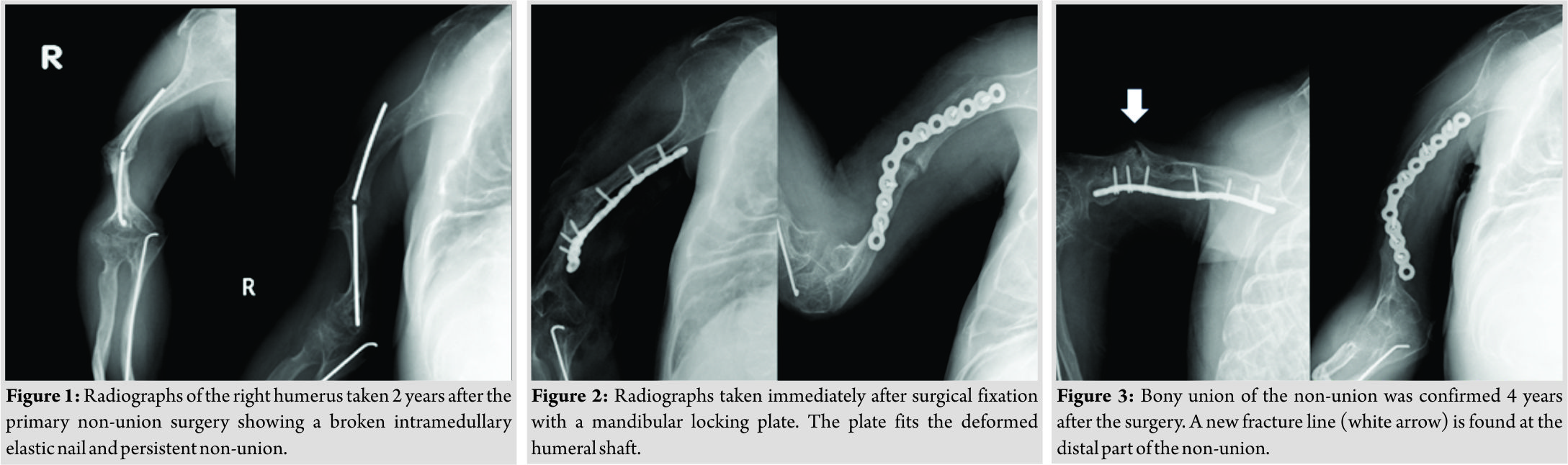
Discussion
Type III OI causes severe bone fragility, and multiple fractures are usually present at birth. These patients develop a severely shortened height and progressive deformity of the limbs and spine with age. Due to their poor bone quality, patients with OI are prone to fractures. These fractures are often difficult to manage because their narrow bone shafts provide limited surface area for contact of prostheses and because bowing adds mechanical stress. In addition, poor bone quality disturbs most treatment plans, especially surgical treatment. Although most low-energy fractures in patients with OI may heal uneventfully, some will fail to achieve bony union. Non-union is more common in patients with than without OI, and patients with Sillence Type III OI are at particularly high risk of non-union. Studies have estimated that approximately 20% of patients with OI develop non-union [4, 5, 6]. In one study, the rate of non-union was slightly lower in patients treated surgically than in those treated conservatively, but the difference was not statistically significant [7]. To obtain good bone fusion, fixation with intramedullary elastic nailing should be considered for femoral non-union complicated by OI [8]. The use of sandwich allograft struts is a durable, safe method for the stabilization and healing of persistent long bone non-union in patients with OI [9]. Intramedullary fixation with autogenous bone graft, combined with concomitant realignment if necessary, is the first-choice treatment for non-union without significant segmental bone loss. Similarly, shortening with an autogenous bone graft and intramedullary fixation is suggested for small gap non-union [10]. In the present case, we selected a locking plate for treatment due to the short diameter of the medullary cavity in the humeral shaft, the hard deformation, the hypertrophic non-union, and the poor bone quality. We used a matrixmandible reconstruction plate “DePuy Synthes, West Chester, PA, USA”. This plate was easy to bend and could be adapted to this case. In addition, this plate was suitable for the patient’s short bone transverse diameter because the screw diameter was also small. The patient’s humeral deformation was hardly a hindrance in his daily life before the development of the non-union. We attempted to fix the bone with a locking plate without correction osteotomy. Hanke et al. [11] reported that the locking plate technique was successful as a salvage procedure in a rare case of adult OI presenting with a femoral fracture. The advantage of using a locking plate is that screws with angular stability are evenly distributed throughout the load without concentrating at one contact point between the bone and the screw. If the fixing force of a conventional plate is lost, it usually starts with a single screw and spreads from there to other screws. The same phenomenon does not occur in a locking screw. Compared with conventional plate constructs, locking plates have mechanical advantages and are thus useful in patients with osteoporosis [12, 13]. Although the current patient was young, his condition was accompanied by bone fragility; locking plates are also useful in such cases. An asymptomatic slight fracture line developed during the 4 years follow-up period. No deterioration was observed by careful follow-up, and the patient attained a partial cure. Although fixation breakdown did not occur, slight screw loosening was observed on X-ray examination. This was not a problem at the time of the present writing, but careful follow-up is necessary.
Conclusion
In this case, humeral non-union in a patient with OI was successfully treated with a mandible locking plate. Locking plates have mechanical advantages and are useful in patients with OI. Although the optimal fixation device for fractures or non-unions in patients with OI has not yet been established, this plate could be a good treatment option for narrow and severely deformed bone.
Clinical Message
Type III OI causes severe bone fragility, and these patients are prone to fractures. These fractures are often difficult to manage how to treat. Mandible locking plate becomes one of the treatment options for fractures or non-unions in patients with OI because this plate is easy to bend and suitable for the patient’s short bone transverse diameter, severe deformity, and fragility bone.
References
1. Lindahl K, Langdahi B, Ljunggren Ö, Kindmark A. Treatment of osteogenesis imperfecta in adults. Eur J Endocrinol 2014;171:R79-90.
2. Monti E, Mottes M, Fraschini P, Brunelli P, Forlino A, Venturi G, et al. Current and emerging treatments for the management of osteogenesis imperfecta. Ther Clin Risk Manag 2010;6:367-81.
3. Sillence DO, Senn A, Danks DM. Genetic heterogeneity in osteogenesis imperfecta. J Med Genet 1979;16:101-16.
4. Vineet A, Benjamin J. Non-union in osteogenesis imperfecta. J Pediatr Orthop B 2005;14:451-5.
5. Gamble JG, Rinsky LA, Strudwick J, Bleck EE. Non-union of fractures in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1988;70:439-43.
6. Agarwal V, Joseph B. Non-union in osteogenesis imperfecta. J Pediatr Orthop B 2005;14:451-5.
7. Eugenio C, Davide D, Giuseppe T, Luca C, Tommaso F, Matteo C, et al. Conservative versus surgical treatment of osteogenesis imperfecta: A retrospective analysis of 29 patients. Clin Cases Miner Bone Metab 2012;9:191-4.
8. Noboru T, Masaru H, Yoshihiro R, Natsuko O. Clinical findings for untreated pseudoarthrosis of femur with osteogenesis imperfecta. Orthop Traumatol 2001;50:973-6.
9. Varun P, Shapiro JR, Sponseller PD. Sandwich allografts for long-bone nonunions in patients with osteogenesis imperfecta. J Bone Joint Surg Am 2015;97:318-25.
10. Shapiro JR, Byers PH, Glorieux FH, Sponseller PD. Osteogenesis Imperfecta. 1st ed. Cambridge, MA: Academic Press; 2013. p. 427-40.
11. Hanke HS, Keel MJ, Todorski IA, Bastian JD. The reversed less invasive stabilisation system-distal femur technique: Application in an adult patient with osteogenesis imperfecta sustaining a femoral fracture.J Orthop Case Rep 2017;7:71-5.
12. Miranda MA. Locking plate technology and its role in osteoporotic fractures. Injury 2007;38 Suppl 3:S35-9.
13. Cornell CN, Ayalon O. Evidence for success with locking plates for fragility fractures. HSS J 2011;7:164-9.
 |
 |
 |
 |
 |
| Dr. Shohei Sano | Dr. Keisuke Oe | Dr. Tomoaki Fukui | Dr. Ryosuke Kuroda | Dr. Takahiro Niikura |
| How to Cite This Article: Sano S, Oe K, Fukui T, Hayashi S, Kuroda R, Niikura T. Humeral Shaft Non-union in a Patient with Osteogenesis Imperfecta Treated with Mandible Locking Plate Fixation: A Case Report. Journal of Orthopaedic Case Reports 2019 May-June; 9(3): 19-21. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2024 Effects of Bisphosphonates on Osteotomy Healing in Osteogenesis Imperfecta: A Case Series
December 1, 2024 Effects of Bisphosphonates on Osteotomy Healing in Osteogenesis Imperfecta: A Case Series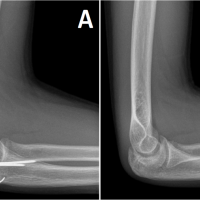 August 10, 2023 Bilateral Synchronous Olecranon Apophyseal Fracture in a Teenager: A Case Report
August 10, 2023 Bilateral Synchronous Olecranon Apophyseal Fracture in a Teenager: A Case Report May 10, 2017 Early Motor Delay: An Outstanding, Initial Sign of Osteogenesis Imperfecta Type 1
May 10, 2017 Early Motor Delay: An Outstanding, Initial Sign of Osteogenesis Imperfecta Type 1 May 10, 2023 Combined Posterior and Convergent Elbow Dislocation in Adult: A Rare Case Report
May 10, 2023 Combined Posterior and Convergent Elbow Dislocation in Adult: A Rare Case Report


