
[box type=”bio”] Learning Point of the Article: [/box]
From this rare case the reader learns from our experience.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 70-73 | Konstantinos N. Mastrantonakis, Charalampos A. Christogiannis, Themistoklis V. Tragaris, Anastasia K. Garmpi, Emmanouil I. Daskalogiannakis. DOI: 10.13107/jocr.2019.v09.i06.1594
Authors: Konstantinos N. Mastrantonakis[1], Charalampos A. Christogiannis[1], Themistoklis V. Tragaris[1], Anastasia K. Garmpi[1], Emmanouil I. Daskalogiannakis[1]
[1]Department of Orthopaedic Surgery, General Hospital of Rethymnon, 17 Trandalidou Street, Rethymnon P.C. 74100, Greece.
Address of Correspondence:
Dr. Konstantinos N Mastrantonakis,
Department of Orthopaedics Surgery, General Hospital of Rethymnon, 17 Trandalidou Street, Rethymnon P.C. 74100, Greece.
E-mail: mastrantonakis.k@gmail.com
Abstract
Introduction: Open fractures in children are uncommon and usually the result of a high-energy trauma. Open distal radius fractures are even more uncommon. In our clinic, we managed a pediatric open fracture separation of the distal radius due to hyper extension and axial load, with low-energy movement of the wrist. To the best of our knowledge, no other similar case or case series is published in literature.
Case Report: Our case involved a 14-year-old male who had been pushing a heavy object during a basketball match. The patient presented at our emergency department with metaphysis of the distal radius protruding through a transverse volar laceration in the wrist. The patient was immediately taken to the operating room and underwent debridement and internal stabilization of the fractures. The wrist was observed for 18 months and no complication occurred.
Conclusion: Through this case report, we present an unusual type of injury that has never been described before; also, we show that the principles of treatment that stand for open fracture in adult patients can be used for children as well.
Keywords: Open fracture, distal radius, pediatric, epiphysiolysis, case report.
Introduction
An open fracture of any bone represents a surgical emergency, with non-predictable results and possible complications. The goal of treatment of an open fracture is to prevent complications, achieve union (but not fusion of the epiphysis when it occurs in children), and restore function of the underlying articulation [1, 2]. In 1976, Gustilo [1, 2] classified open fractures in three stages; type III was further modified into three subcategories in 1984. Gustilo [2] reported the four important features that need to be taken into account when dealing with these types of fractures. First, as these injuries are most often a result of a high-energy trauma, it is important to stabilize the patient before treating the fracture. Second, soft tissue lesions can determine the treatment plan and the prognosis. Third, all open fractures are considered to be contaminated with bacteria. Fourth, open fractures are an orthopedic emergency and should be stabilized within 8 h from the time of injury. There are differences in the healing processes of these injuries for children and adults, the most important being the presence of growth plates and the thicker periosteum in pediatric bones. Fractures involving the growth plate can result in partial or complete physeal arrest. The thicker and more active periosteum provides fracture stability and faster fracture healing compared with that in older children and adults [3]. Moreover, the rates of infection in open fractures have been shown to be lower in children than in adults [4]. Early fracture stabilization is decisive for soft tissue healing and preservation of neurovascular status, as well as to decrease the possibility of infection. Rigid fixation is not always as important in children, as it is in adults in certain settings. Surgical treatment options for distal unstable fracture of the distal radius mainly consist of K-wire fixation [5, 6, 7, 8]. Percutaneous K-wire fixation provides adequate stability and can be removed easily after fracture healing, thereby not affecting bone growth in young individuals. This technique was first described by Kapandji, in 1976, for adult patients [9].
Case Report
Case
A 14-year-old male presented to the emergency department 15 min after a hyperextend and axial load force injury. The boy was trying to push a heavy object during a basketball game, resulting in an open volar fracture epiphysiolysis of the distal radius and fracture on the distal one-third diaphysis of the ulna. The patient’s right hand was dressed with gauze and a bandage that had been applied by the physician of the sporting match. After removing the dressing, the distal radius metaphysis was found to be protruding through a transverse volar laceration in the wrist area, 5 cm in length. Immediately, the wound was irrigated with 4 L of isotonic sodium chloride solution and the fracture was reduced under local anesthesia. Care was taken not to harm the median nerve, the ulnar nerve, and the ulnar artery which were very close to the fracture. The wound was dressed after debridement and a short arm cast was applied. The patient’s neurovascular status was found to be intact. Intravenous cefazolin and an antitetanus serum were administered. An X-ray of the wrist was performed and the boy was taken to the operating room.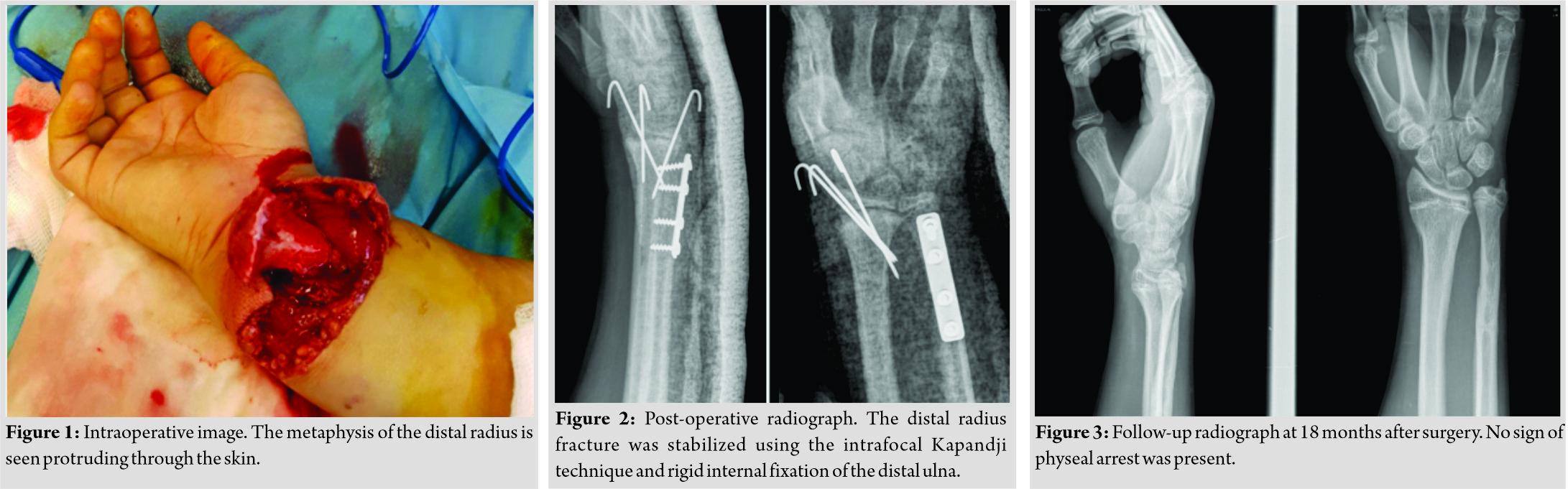
Treatment
The first step in the surgery was making of an extension longitudinal incision of 2 cm in the middle of the volar side of the wrist, after which the metaphysis of the radius was manually relocated (Fig. 1). The wound and the bone fragments were irrigated with 5 L of isotonic sodium chloride solution. Attention was taken to recognize all the important structures of the volar site of the wrist. The median and ulnar nerves, the radial and ulnar arteries, such as the flexor tendons, were found to be intact. The metaphysis was then manually reduced to its normal position and fixed with three percutaneous Kirschner wires (Fig. 2). Great care has been taken not to pass the K-wires through the growth plate so that it does not affect its healing. A standard ulnar approach was used and a 5 cm incision was made over the fracture site. Standard dissection principles were applied to expose the ulnar fracture. After adequate reduction, a four-hole plate was placed over the fracture line and stabilized with 3.5mm cortical screws. The incisions were irrigated with normal saline and the wounds were closed in a normal layered fashion. Sterile dressings and a below-elbow cast were applied to the right upper limb.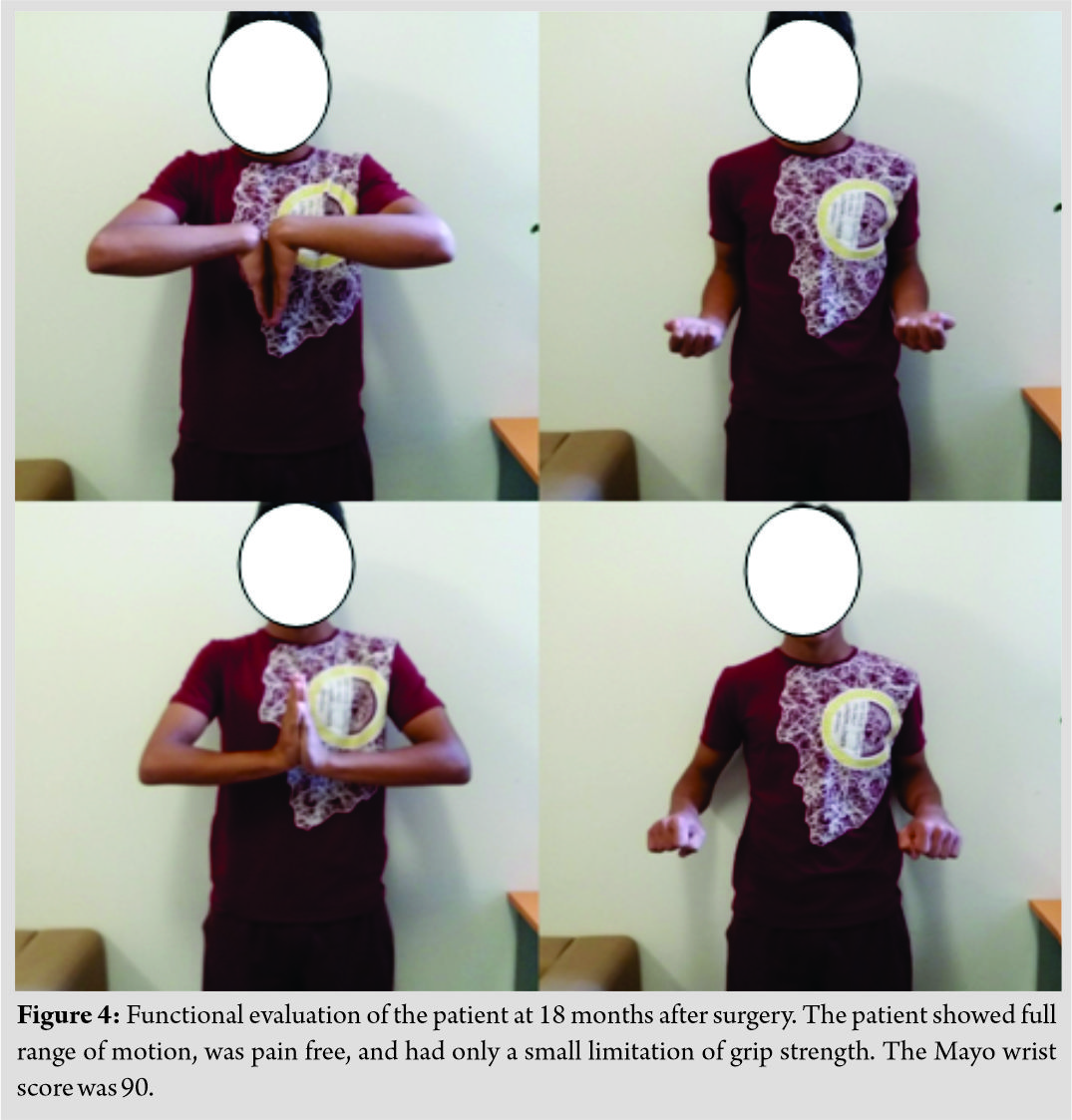
Outcome and follow-up
Postoperatively, the patient was followed up in the outpatient clinic for 6 weeks, with once-weekly changing of the dressing and X-ray. After removal of the K-wires and cast at the end of the 6-week period, the patient was recommended a routine of gentle range of motion exercises. The patient attended additional follow-up at 6 months, 1 year, and 18 months. He achieved full range of motion and full strength of the wrist, with no radiographic signs of physeal arrest (Fig. 3 and 4). After 12 months, the patient scheduled surgery for material removal.
Discussion
Open fractures in children are uncommon and usually the result of a high-energy trauma. Open distal radius fractures are even more uncommon. In our clinic, we managed an open fracture separation of the distal radius that was due to a hyper extension and axial load, with low-energy movement of the wrist. Our search of literature did not find any other similar case or case series. We treated this 14-year-old male immediately with proper debridement, with respect to the soft tissue and intravenous antibiotics on arrival at the emergency department. Proper debridement and antibiotic administration are associated with a fairly low incidence of complications [10]. For stabilization, we used the Kapandji method for the distal radius and rigid internal fixation for the ulnar fracture. Intrafocal Kapandji pinning for the treatment of unstable metaphyseal and Salter-Harris type II fractures of the distal radius is seldom used in children with lower complication rate than conventional pinning [11]. As a result, the patient experienced no early complications such as infection, malunion- or nonunion and no late complications such as physeal arrest of the distal radius.
Conclusion
Through this case report, we present an unusual type of injury that has never been described before; also, we show that the principles of treatment that stand for open fracture in adult patients can be used for children as well.
Clinical Message
Compound fractures break the skin barrier and come into contact with bacteria. There are several parameters that have to be taken in consideration for not causing infection that can potentially damage the growth plate. Proper debridement, immediate placement of antibiotics, and early time of the surgery are mandatory for a favorable outcome.
References
1. Gustilo RB. Management of open fractures and complications. In: Frankel VH, editor. Instructional Course Lectures, American Academy of Orthopedic Surgeons. Vol. 31. St. Louis: CV Mosby; 1982. p. 61.
2. Gustilo RB. Current concepts in the management of open fractures. In: Frankel RH, editor. Instructional Course Lectures, American Academy of Orthopedic Surgeons. Vol. 36. St. Louis: CV Mosby; 1987. p. 359.
3. Rodríguez-Merchán EC. Pediatric skeletal trauma: A review and historical perspective. Clin Orthop Relat Res 2005;432:8-13.
4. Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracture wounds. Clin Orthop Relat Res 1989;243:36-40.
5. Ramoutar DN, Shivji FS, Rodrigues JN, Hunter JB. The outcomes of displaced paediatric distal radius fractures treated with percutaneous kirschner wire fixation: A review of 248 cases. Eur J Orthop Surg Traumatol 2015;25:471-6.
6. McLauchlan GJ, Cowan B, Annan IH, Robb JE. Management of completely displaced metaphyseal fractures of the distal radius in children. A prospective, randomised controlled trial. J Bone Joint Surg Br 2002;84:413-7.
7. Huang W, Zhang X, Zhu H, Wang X, Sun J, Shao X, et al. A percutaneous reduction technique for irreducible and difficult variant of paediatric distal radius and ulna fractures. Injury 2016;47:1229-35.
8. Rubin G, Orbach H, Chezar A, Rozen N. Treatment of physeal fractures of the distal radius by volar intrafocal kapandji method: Surgical technique. Arch Orthop Trauma Surg 2017;137:49-54.
9. Kapandji A. Internal fixation by double intrafocal plate. Functional treatment of non articular fractures of the lower end of the radius (author’s transl). Ann Chir 1976;30:903-8.
10. Greenbaum B, Zionts LE, Ebramzadeh E. Open fractures of the forearm in children. J Orthop Trauma 2001;15:111-8.
11. Valisena S, Gonzalez JG, Voumard NM, Hamitaga F, Ciritsis BD, Mendoza Sagaon M, et al. Treatment of paediatric unstable displaced distal radius fractures using Kapandji technique: A case series. Eur J Orthop Surg Traumatol 2019;29:413-20.
 |
 |
 |
 |
 |
| Dr. Konstantinos N. Mastrantonakis | Dr. Charalampos A. Christogiannis | Dr. Themistoklis V. Tragaris | Dr. Anastasia K. Garmpi | Dr. Emmanouil I. Daskalogiannakis |
| How to Cite This Article: Mastrantonakis K, Christogiannis C, Tragaris T, Garmpi A, Daskalogiannakis E. Management of an Open Distal Radius Epiphysiolysis in a 14-year-old Male: A Case Report. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 70-73. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2019 Hybrid Fixation in Pediatric Forearm Fractures, does it Predispose to Non-union? A Case Report and Literature Review
May 10, 2019 Hybrid Fixation in Pediatric Forearm Fractures, does it Predispose to Non-union? A Case Report and Literature Review July 1, 2025 A Large-diameter Corona Mortis Artery Encountered During Surgery for Acetabular Fracture: A Case Report and Review of Anatomical Significance
July 1, 2025 A Large-diameter Corona Mortis Artery Encountered During Surgery for Acetabular Fracture: A Case Report and Review of Anatomical Significance June 1, 2025 A Rare Case of Bilateral Congenital Radial Head Dislocation: A Case Report
June 1, 2025 A Rare Case of Bilateral Congenital Radial Head Dislocation: A Case Report April 1, 2025 Bilateral Anterior Shoulder Dislocations with Greater Tuberosity Fractures Study Design: A Case Report
April 1, 2025 Bilateral Anterior Shoulder Dislocations with Greater Tuberosity Fractures Study Design: A Case Report


