
[box type=”bio”] Learning Point of the Article: [/box]
A metabolic disorder like gout can masquerade as a tumor and it is important that one is clinically aware of its varied presentations.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 17-19 | Amit kumar Bagdia, Prateek Hegde, Amit Janu, Kavita Khirwal, Ajay Puri, Ashish Gulia. DOI: 10.13107/jocr.2020.v10.i04.1782
Authors: Amitkumar Bagdia[1], Prateek Hegde[1], Amit Janu[2], Kavita Khirwal[3], Ajay Puri[1], Ashish Gulia[1]
[1]Department of Surgical Oncology, Tata Memorial Centre, Homi Bhabha National Institute, Mumbai, Maharashtra, India,
[2]Department of Radiodiagnosis, Tata Memorial Centre, Homi Bhabha National Institute, Mumbai, Maharashtra, India,
[3]Department of Pathology, Tata Memorial Centre, Homi Bhabha National Institute, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Ashish Gulia,
Professor, Orthopaedic Oncology, Department of Surgical Oncology, Tata Memorial Centre, Homi Bhabha National Institute, Dr. E Borges Road, Parel, Mumbai – 400 012, Maharashtra, India.
E-mail: aashishgulia@gmail.com
Abstract
Introduction: Gout is a metabolic disorder known to mimic other disorders. Here is a case report of a patient in which gout was mimicking giant cell tumour of bone.
Case Report: A 48-year-old lady presented with gradually progressive pain and swelling in the right foot. After evaluation with imaging and biopsy, she was counseled that she had giant cell tumor (GCT) of bone and planned for curettage. She chose to have a second opinion, and the biopsy slides were reviewed and the diagnosis of GCT was said to be unlikely based on the appearance under microscope. Gout was suggested as the most probable diagnosis after re-discussion in the tumor board meeting by corroborating clinical, radiological, and pathological findings. The patient was then referred to a rheumatologist, where she responded to medical management.
Conclusion: Gout can present with multiple deceptive symptoms, and the key is to correlate all the factors before coming to a diagnosis.
Keywords: Gout, giant cell tumor, foot, ankle.
Introduction
A diagnostic dilemma where it is necessary to differentiate neoplastic conditions from “neoplastic mimics” is not unusual in musculoskeletal oncology. Gout is one such metabolic disorder that has been known as “The Great Mimicker” since the times of Hippocrates [1]. We present a case report, where gout presented in a way similar to the giant cell tumor (GCT) of bone.
Case Report
A 48-year-old lady had gradually progressive pain and swelling in the right foot for 4 months. It was not associated with signs of infection such as fever, local inflammation, or any signs of chronic arthritis. She had significant comorbidities, including dilated cardiomyopathy with low ejection fraction (15–20%), diabetes mellitus, and chronic hepatitis-C infection. She was evaluated elsewhere with a radiograph and magnetic resonance imaging (MRI) of the foot. Imaging revealed a soft-tissue lesion eroding and involving navicular, calcaneum, and talus with a cystic/necrotic component. A computed tomography (CT)-guided biopsy from the soft-tissue component revealed a benign giant cell-rich lesion. She was counseled about the nature of the disease, that is, a GCT of bone and was planned for surgical curettage.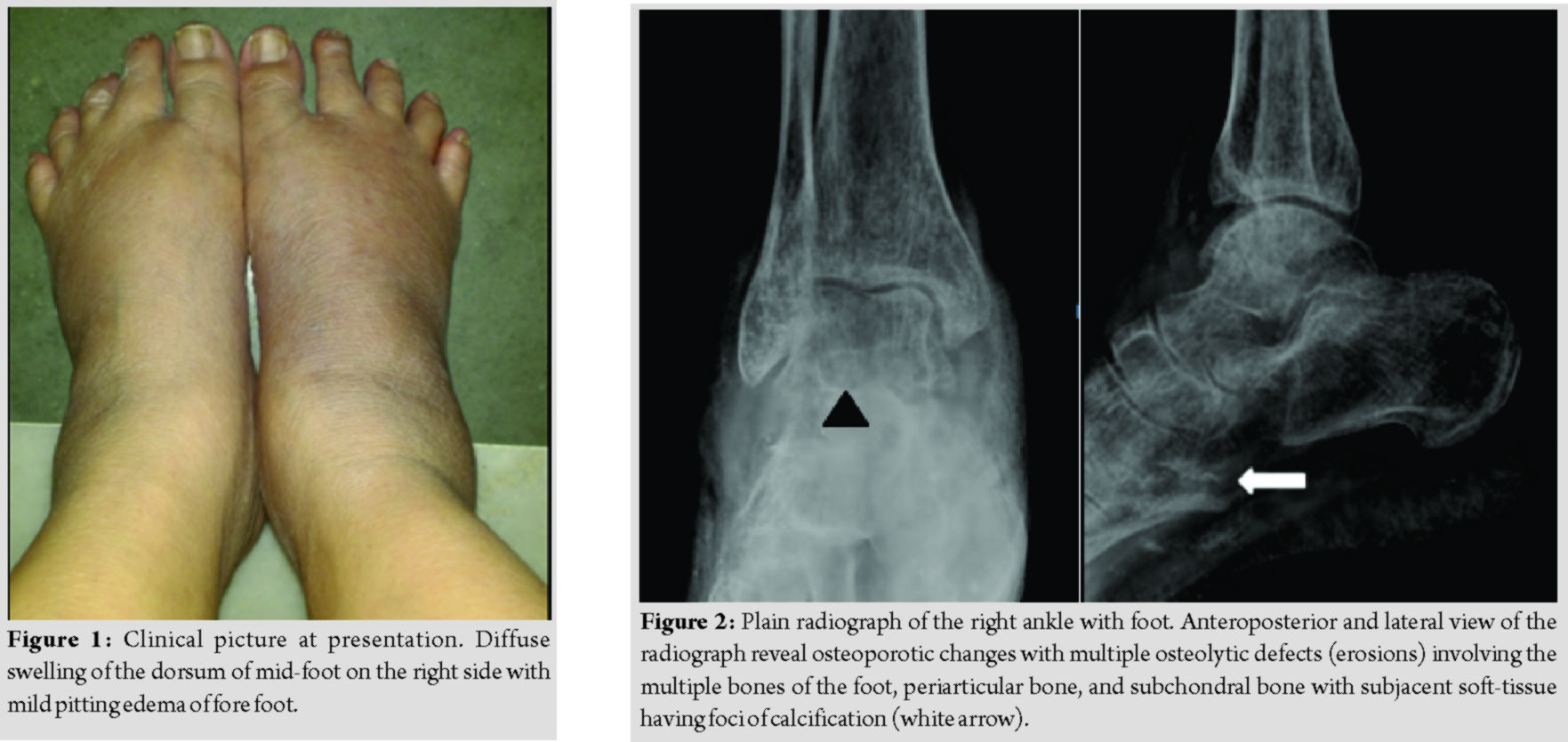
On presentation to our institute, there was diffuse swelling of the dorsum of mid-foot with mild pitting edema of forefoot without any associated pain (Fig. 1). All movements of the toes and ankle were a normal without any neurovascular deficits. She was evaluated further with blood investigations which revealed a normal hemogram and raised uric acid of 15.2 (normal range 3.5–7.2 mg/dL) and creatinine levels of 1.8 (normal range 0.7–1.3 mg/dL).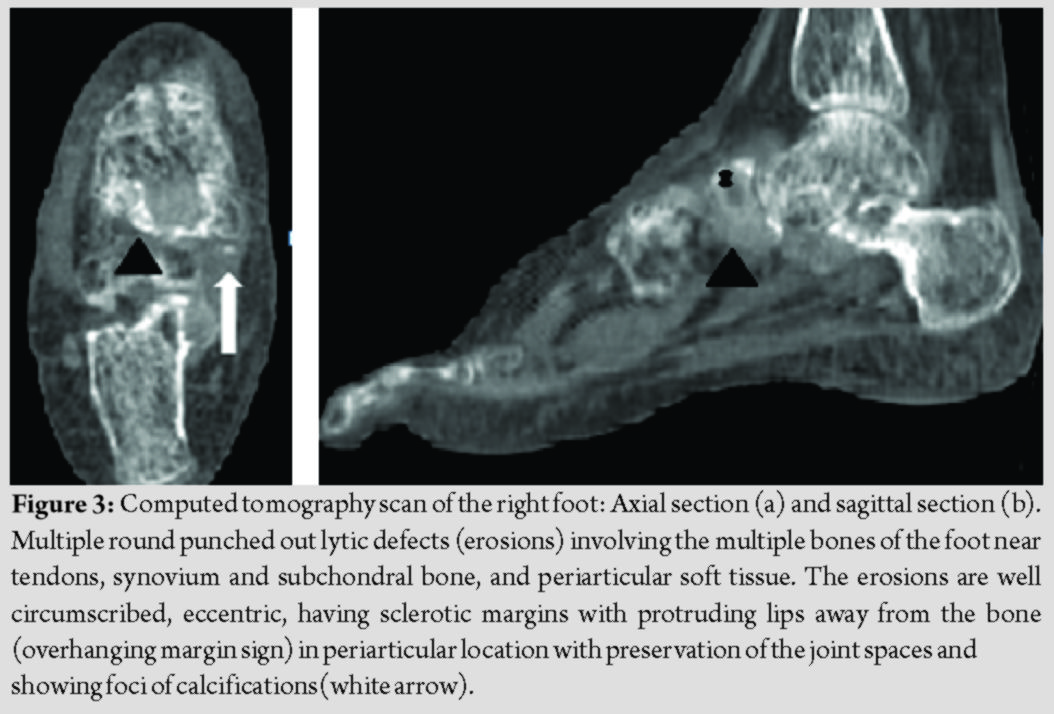
A plain radiograph (Fig. 2) and CT scan (Fig. 3) were done. Plain radiograph of the foot revealed generalized osteoporosis, erosions, osteolytic defects, and calcifications. The so-called “overhanging margins sign” and preservation of joint spaces were evident on CT scan. Imaging features were not unequivocal for GCT. The MRI (Fig. 4) obtained elsewhere previously was reviewed in the multidisciplinary meeting of our institute.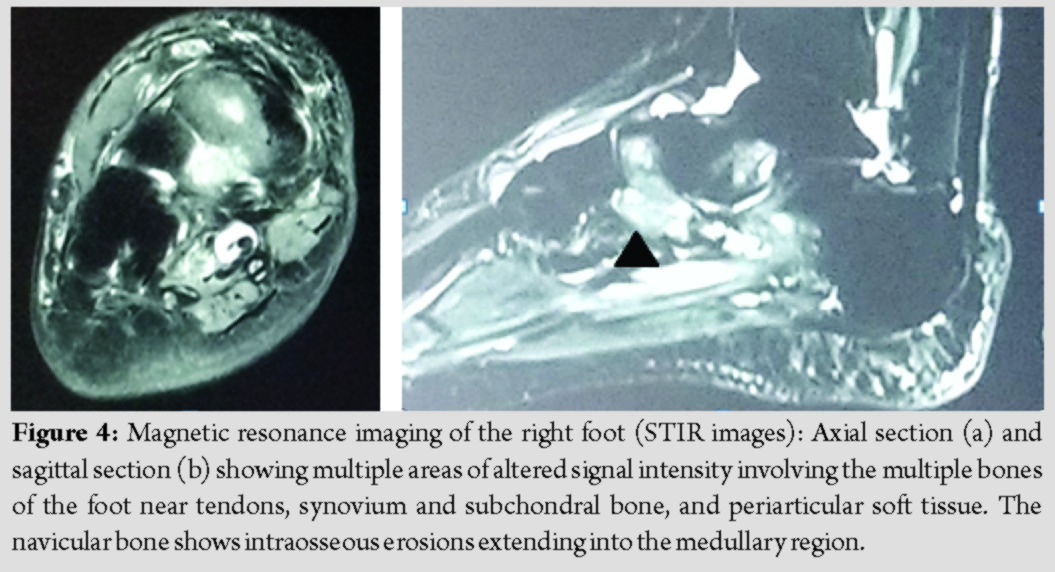
The biopsy slides were also reviewed. The earlier diagnosis of GCT was considered unlikely based on the appearance under the microscope (Fig. 5) which showed features such as organized granulomatous reaction, central acellular amorphous eosinophilic zone surrounded by corona zone composed of foreign body giant cell reaction, lymphoplasmacytic infiltrate, and histiocytes. Distinct foreign body giant cells were noted; however, no tumor giant cells were seen. There were no nuclear atypia and no mitosis. No native bone, cartilage, synovium, or calcification were seen in the biopsy.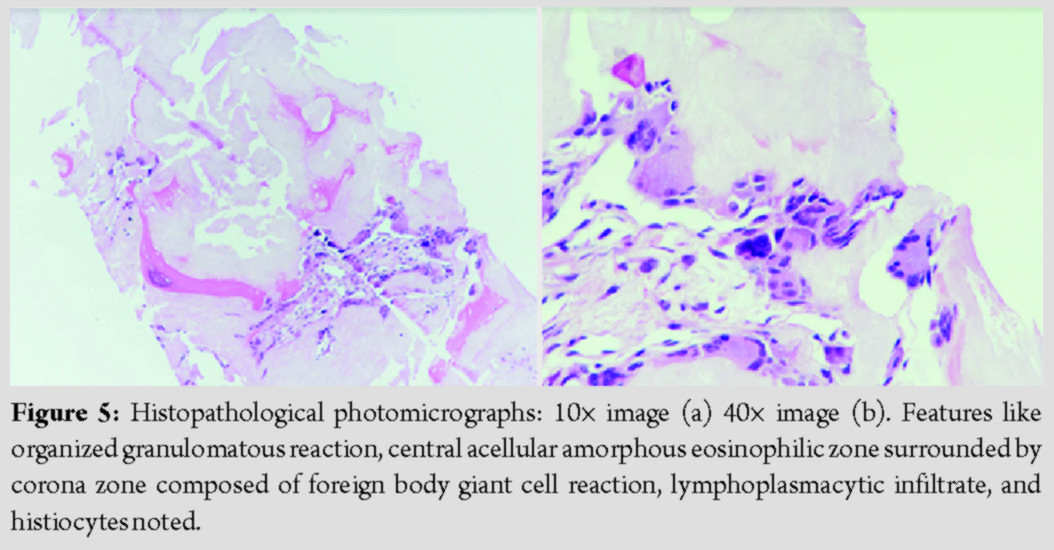
Gout was suggested as the most probable diagnosis after re-discussion in the tumor board meeting by corroborating the clinical, radiological, and pathological findings. The patient was then referred to a rheumatologist where she was started on the medical line of management to which she responded well.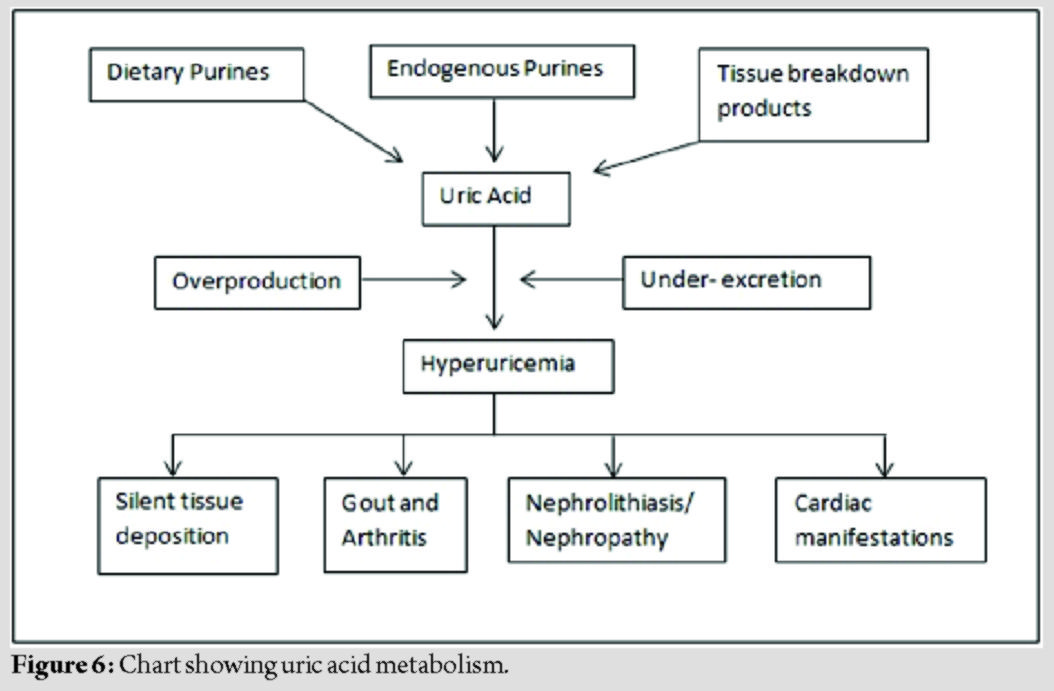
Discussion
Gout is a disorder of uric acid metabolism (Fig. 6), where the excess of uric acid crystallizes and gets deposited in form of monosodium urate in joints, periarticular tissues, and also in the kidney [2]. The symptoms include episodes of arthritis and chronic nephropathy. Symptom spectrum is known to overlap and mimics numerous diseases with etiologies as varied as infective (bacterial, fungal, and tubercular [3]), inflammatory, autoimmune, or malignant disorder [4, 5]. Typically, the first and most striking clinical manifestation of gout is the appearance of podagra, the association of which with its location in a great toe is such that diagnosis of gout presenting with other atypical features is easy to miss, as was in this case. Our patient had corroborative classical features of uric acid overload, including cardiac failure and nephropathy, along with diabetes and symptoms of metabolic syndrome, but the diagnosis was elusive as the presentation was unusual. Gout may present with varied radiological findings such as an expansile bony lesion or an aggressive/destructive or cystic lesion. The plain radiograph may show a well-defined lytic, erosive, peri-articular lesion with an overhanging edge. Typically, the preservation of joint space is noted [6, 7]. In the literature, multiple cases of gout as a mimicker of various pathologies, including a few malignant, process, even soft-tissue sarcomas [4], have been described. There have also been reports of gout mimicking a GCT, but that of the tendon sheath, tendon, or soft tissues [8]. In most instances, the patients were known cases of gout, who had presented earlier with gouty arthritis or other classical features of gout and were already under treatment, so the index of suspicion for the lesion being gout was high. Gout masquerading as GCT of bone is rare and reports could not be found in the literature, this being perhaps the first such publication. Such cases where the incidence is rare, needs a highly experienced multidisciplinary musculoskeletal oncology team comprising of a surgeon, radiotherapist, medical oncologist, radiologist, and pathologist to decide conclusively that the lesion is a benign condition [9]. Misdiagnosing a malignancy or even a GCT can have far-reaching ramifications.
Conclusion
Gout can present with multiple deceptive symptoms and may be misdiagnosed as malignancies too. Many times, the treatment decisions have to be based on clinical judgment and acumen. This case report reiterates the indispensability of a meticulous examination, detailed workup, impeccable reading of imaging, and confident pathology reporting in the process of rational clinical management and decision making.
Clinical Message
This case report reiterates the importance of taking an holistic approach for the diagnosis and treatment of a patient and also the need to be aware of the possibility that a metabolic disorder like gout can masquerade as a tumor.
References
1. Copeman WC. A Short History of Gout. Berkeley, California: University of California Press; 1964.
2. Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet 2016;388:2039-52.
3. Asz-Sigall D, Arenas R, Domínguez-Cherit J, Vega-Memije ME. Gouty tophi: The great mimicker. Med Cutan Iber Lat Am 2005;33:76-9.
4. Hee LW, Singh VA, Jayalakshmi P. Can gout mimic a soft tissue tumour? BMJ Case Rep 2010;2010:2266.
5. Fleet MS, Raby N. Case report: An unusual presentation of gout. Clin Radiol 1997;52:156-8.
6. Girish G, Glazebrook KN, Jacobson JA. Advanced imaging in gout. Am J Roentgenol 2013;201:515-25.
7. Chowalloor PV, Siew TK, Keen HI. Imaging in gout: A review of the recent developments. Ther Adv Musculoskelet Dis 2014;6:131-43.
8. Gezmis E, Boya H, Öztürk FU, Yerli H, Izmir TR, Ankara TR. Unusual initial presentation of gout as intratendinous tophus mimicking giant cell tumor of tendon sheath : Report of two cases. ESSR Poster 2016;2016:0008.
9. Mulchandani N, Maheshwari E, Agarwal S, Maheshwari A. The role of tumor boards and referral centers. In: Henshaw RM, editor. Sarcoma: A Multidisciplinary Approach to Treatment. Switzerland: Springer; 2017. p. 11-5.
 |
 |
 |
 |
 |
 |
| Dr. Amitkumar Bagdia | Dr. Prateek Hegde | Dr. Amit Janu | Dr. Kavita Khirwal | Dr. Ajay Puri | Dr. Ashish Gulia |
| How to Cite This Article: Bagdia A, Hegde P, Janu A, Khirwal K, Puri A, Gulia A. Unusual presentation of gout as giant cell tumor of bone: A case report. Journal of Orthopaedic Case Reports 2020 July;10(4): 17-19. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


