
[box type=”bio”] Learning Point of the Article: [/box]
Chondroblastoma of carpal bones such as pisiform is a rare entity and requires high index of suspicion and radiological and histopathological confirmation.
Case Report | Volume 10 | Issue 6 | JOCR September 2020 | Page 9-13 | Ashish Rustagi, Saumya Agarwal, Geetika Khanna, L G Krishna, Jatin Talwar, Shivank Prakash. DOI: 10.13107/jocr.2020.v10.i06.1854
Authors: Ashish Rustagi[1], Saumya Agarwal[1], Geetika Khanna[2], L G Krishna[1], Jatin Talwar[1], Shivank Prakash[1]
[1]Department of Orthopaedics, Central Institute of Orthopaedics, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. [2]Department of Pathology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Address of Correspondence:
Dr. Saumya Agarwal,
Department of Orthopaedics, Central Institute of Orthopaedics, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
E-mail: saumyathecalyx.agarwal@gmail.com
Abstract
Introduction: Chondroblastoma is a rare primary benign tumor of bone with male predominance and is typically seen in an epiphyseal location. The pisiform is a carpal bone and chondroblastoma of the pisiform has not been reported in the literature to the best of our knowledge.
Case Presentation: An 18-year-old male presented with painful swelling over his right wrist with restriction of ulnar deviation. Based on magnetic resonance imaging findings, two diagnostic possibilities were entertained, namely, giant cell tumor of bone and chondroblastoma. Wide local excision was performed, and histopathology confirmed the diagnosis of chondroblastoma of the pisiform. After 2 years of follow-up, the patient has gained pain-free wrist movements post excision, and there are no signs of recurrence. The Modified Mayo Wrist Score of 75 (fair) improved to 100 (excellent).
Conclusion: Surgeon should always keep in mind the possibility of the tumor at the rare site and accurately diagnose the tumor with the help of imaging modalities and biopsy.
Keywords: Chondroblastoma, epiphyseal tumor, pisiform, wide local excision, neoplasm.
Introduction
Chondroblastoma is a rare, cartilage-producing bone tumor that tends to occur in the long bones of skeletally immature individuals. It was originally described by Ewing in 1928 as a “calcifying giant cell tumor.” [1] It is typically seen in the epiphyseal location and is characterized histologically by the proliferation of immature/embryonic chondrocytes (or chondroblasts). Secondary elements, such as giant cells, calcification, and occasionally aneurysmal bone cyst formation, are often seen. The tumor is uncommon, accounting for <1% of all primary bone tumors. It mostly occurs in the second decade of life, with an average age of 19–23 years [2, 3, 4]. There is a male predominance with a male-to-female ratio of approximately 2:1. Long-standing bone pain is the most common presentation. The local examination may reveal tenderness, decreased range of motion in the affected joint, joint effusion, muscular atrophy, and a palpable mass which may be a common clinical presentation. Chondroblastoma is typically a solitary lesion, with the most common sites being the proximal tibia or femur, distal femur, and proximal humerus [5]. In older individuals, the location is much more variable, and tumors may involve non-tubular bones such as the craniofacial skeleton or bones of the hands and feet [3, 4]. Primary neoplasms of the carpal bones are rare. Murray and Berger [6] found 44 primary tumors of the carpal bones of 26,800 bone neoplasms (prevalence, 0.16%). About 86% were benign; 14% were malignant. The most common tumor was osteoid osteoma. Chondroblastoma of carpal bones such as triquetrum and capitate has been reported in the literature, but there is no case regarding chondroblastoma of the pisiform. Radiologically, the tumor is a well-demarcated, eccentric, and lytic lesion with peripheral sclerosis. The average size varies from 3 to 6 cm, although tumors exceeding 10 cm can occur [7]. Central “fluffy” calcifications are commonly radiodense. Extensive edema surrounding the lesion can typically be seen in magnetic resonance imaging (MRI). On gross examination, the tumor appears distinct from the adjacent bone and contains a mixture of soft, friable, grey-yellow material, and hemorrhage. Small calcifications provide a gritty and chalky cut surface. Histologically, sheets of small to intermediate-sized round to polygonal cells are seen. The tumor cells demonstrate well-defined cytoplasmic margins and eosinophilic cytoplasm, although focally, clear cell change can be seen. The nucleus is centrally placed and relatively large, and often a central, longitudinal nuclear groove (“coffee bean” appearance) can be seen. Chondroid matrix formation usually confirms the diagnosis of chondroblastoma. Bluish or purple granular calcium deposits are seen in approximately one-third of cases, most commonly in long bone tumors. The calcifications may be seen in the cytoplasm or stroma, where they demonstrate a delicate pericellular lacelike or “chicken-wire” appearance [3]. Surgery remains the mainstay of the treatment and includes extended curettage with or without bone grafting, en bloc resection, or rarely, amputation. Chemical cauterization with phenol or cryosurgery can also be used as adjunctive therapy. For recurrent tumors, resection remains the treatment of choice, although select cases may also receive radiation therapy after repeated curettage fails to cure. We are presenting here a case presentation of chondroblastoma of the pisiform which is the first report of its kind.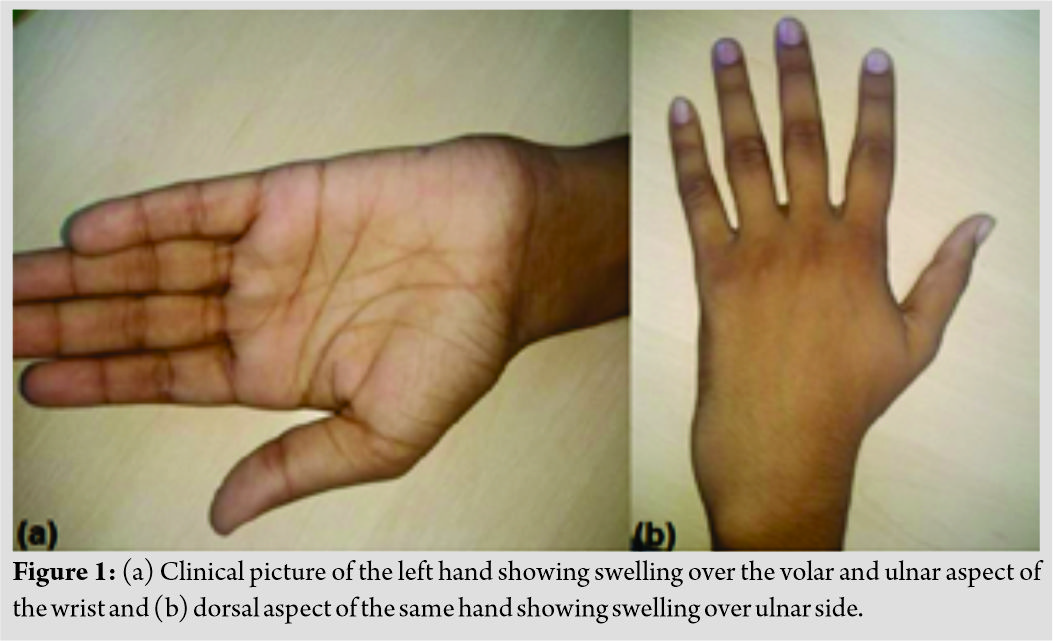
Case Report
An 18-year-old male came to the orthopedics OPD of Safdarjung Hospital, New Delhi, with complains of pain and swelling in the left wrist for 4 months. The pain was insidious in onset and progressive in nature. The swelling was bony hard and not adherent to the skin (Fig. 1). Ulnar deviation of the left wrist was found to be painful. X-ray (anteroposterior view) of the left wrist showed a lytic lesion around distal ulna and pisiform bone (Fig. 2). 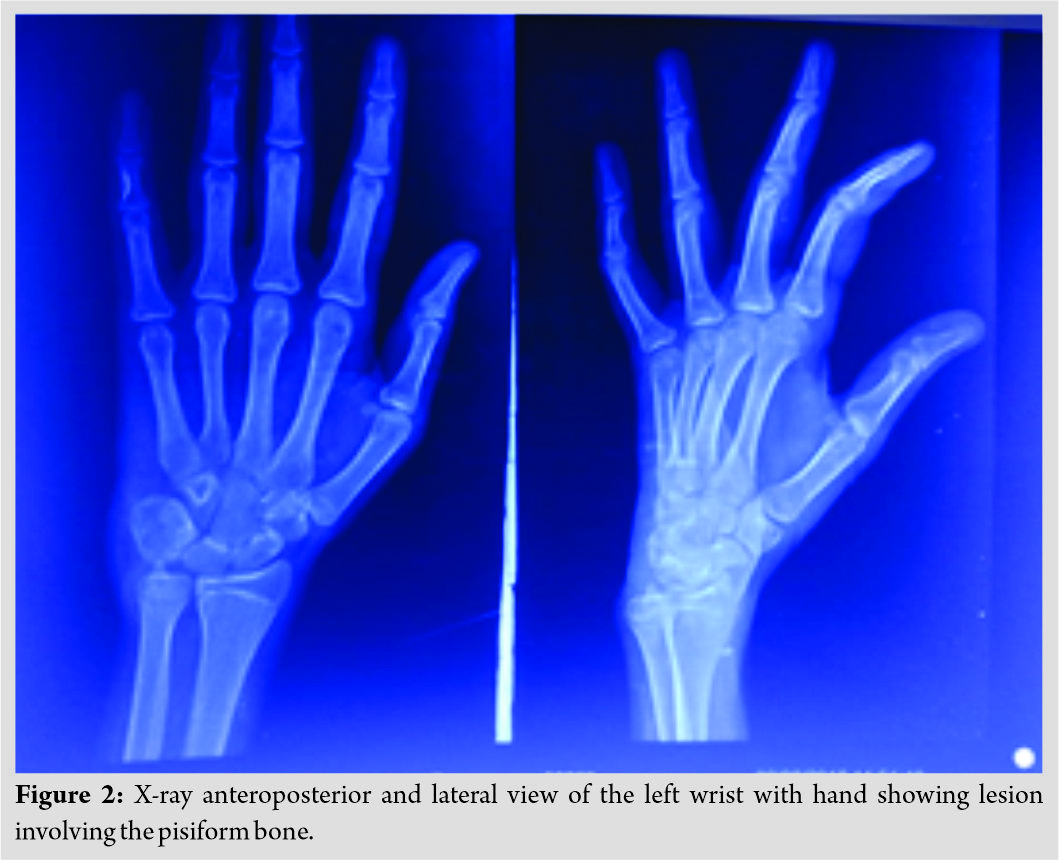 MRI revealed the expansion of the pisiform bone with altered marrow signal and morphology (Fig. 3).
MRI revealed the expansion of the pisiform bone with altered marrow signal and morphology (Fig. 3).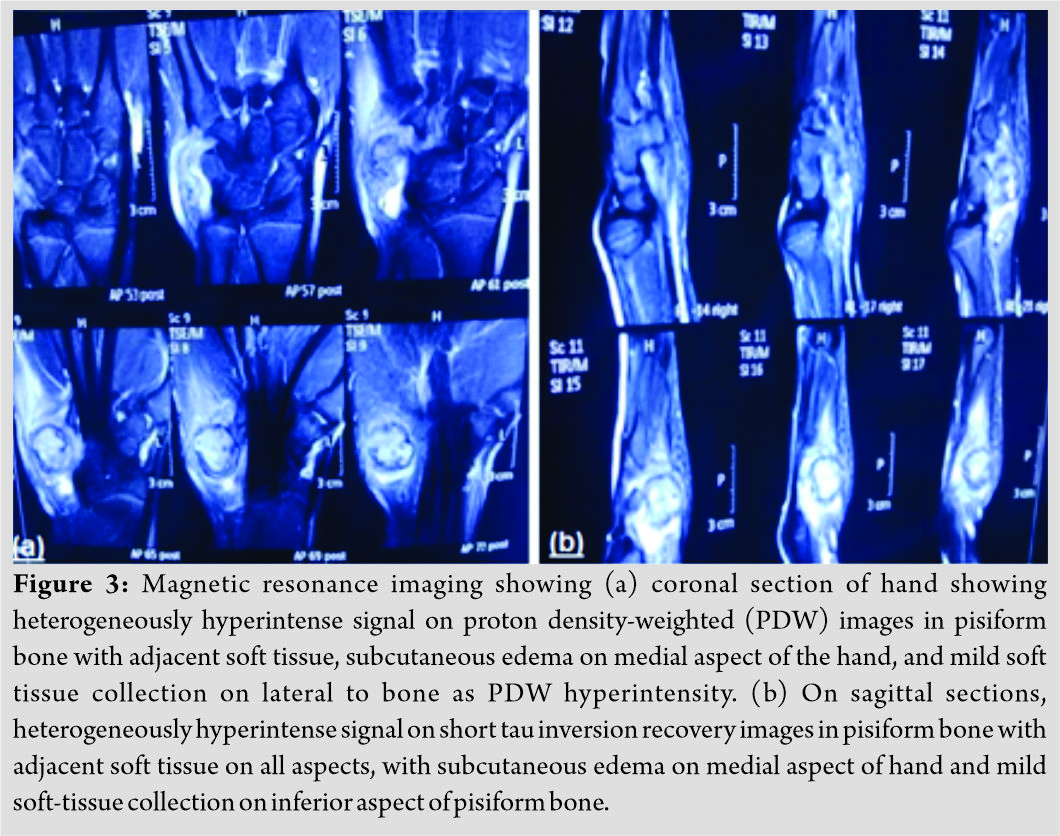 The pisiform bone showed an isointense signal on T1 and was hyperintense on T2 images. The involved bone shows an irregular cortical outline, and the internal matrix was lobulated suggesting differential diagnosis of giant cell tumor and aneurysmal bone cyst. Pre-anesthetic check-up was done, and consent was taken. The patient was kept in the supine position with palm facing upward, and then, a 5 cm curvilinear incision was made over the volar aspect of the left wrist. A thorough layer by layer dissection was performed taking care of all the adjacent vital structures, and the tumor was identified. A wide margin bony excision was then performed (Fig. 4) and closure was done in layers.
The pisiform bone showed an isointense signal on T1 and was hyperintense on T2 images. The involved bone shows an irregular cortical outline, and the internal matrix was lobulated suggesting differential diagnosis of giant cell tumor and aneurysmal bone cyst. Pre-anesthetic check-up was done, and consent was taken. The patient was kept in the supine position with palm facing upward, and then, a 5 cm curvilinear incision was made over the volar aspect of the left wrist. A thorough layer by layer dissection was performed taking care of all the adjacent vital structures, and the tumor was identified. A wide margin bony excision was then performed (Fig. 4) and closure was done in layers. 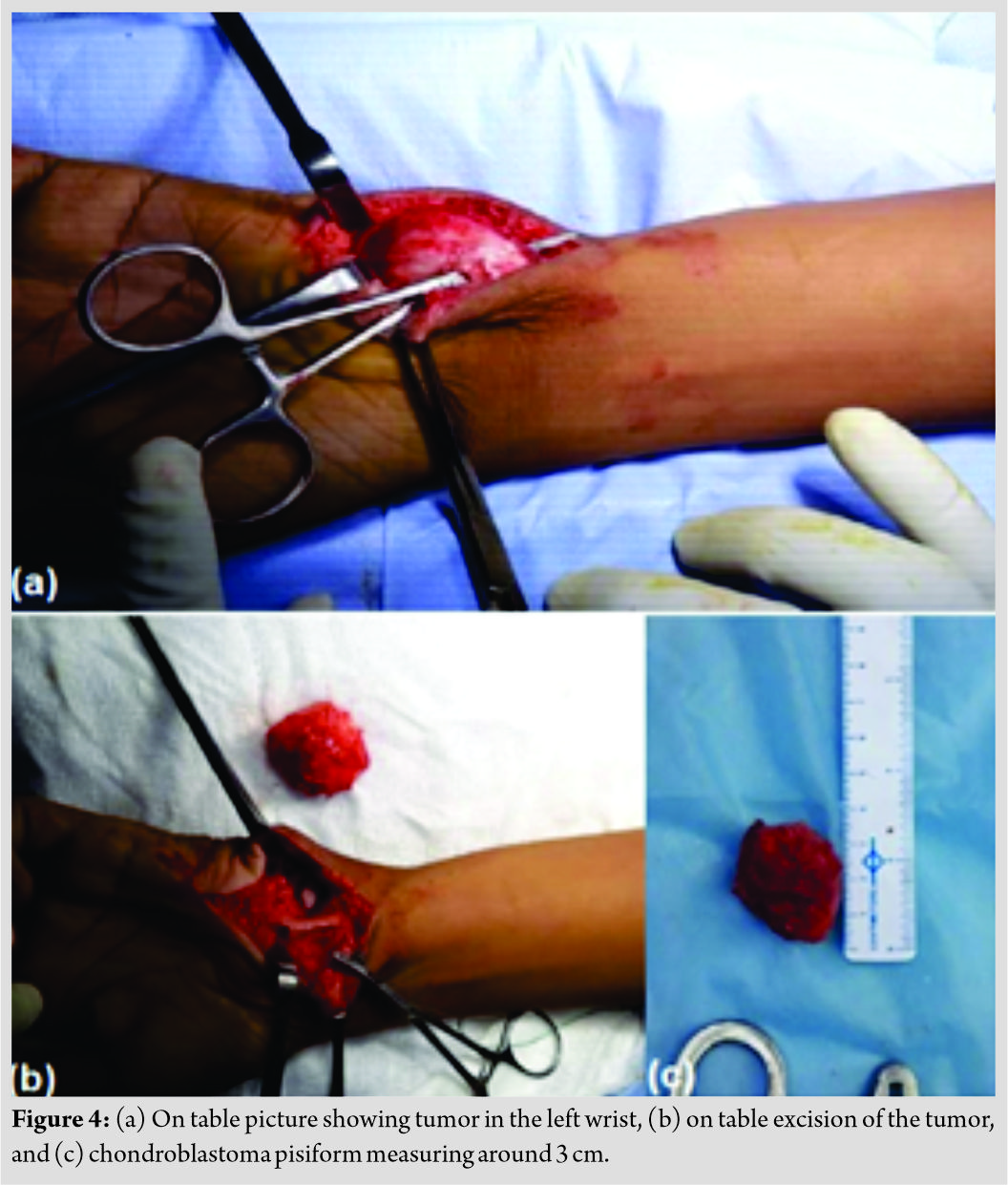 Suture removal was done after 14 days, and till then, the patient was kept on antibiotics. The sample obtained was sent for histopathological analysis which revealed it to be a chondroblastoma (Fig. 5).Active and active-assisted range of motion exercises were initiated after suture removal. Follow-up (Fig. 6) was done at 6 weeks, 3 months and 6 months, 1 year and 2 years, and thereafter. The lesion resolved with the resolution of pain and swelling. Wrist movements were not affected.
Suture removal was done after 14 days, and till then, the patient was kept on antibiotics. The sample obtained was sent for histopathological analysis which revealed it to be a chondroblastoma (Fig. 5).Active and active-assisted range of motion exercises were initiated after suture removal. Follow-up (Fig. 6) was done at 6 weeks, 3 months and 6 months, 1 year and 2 years, and thereafter. The lesion resolved with the resolution of pain and swelling. Wrist movements were not affected. 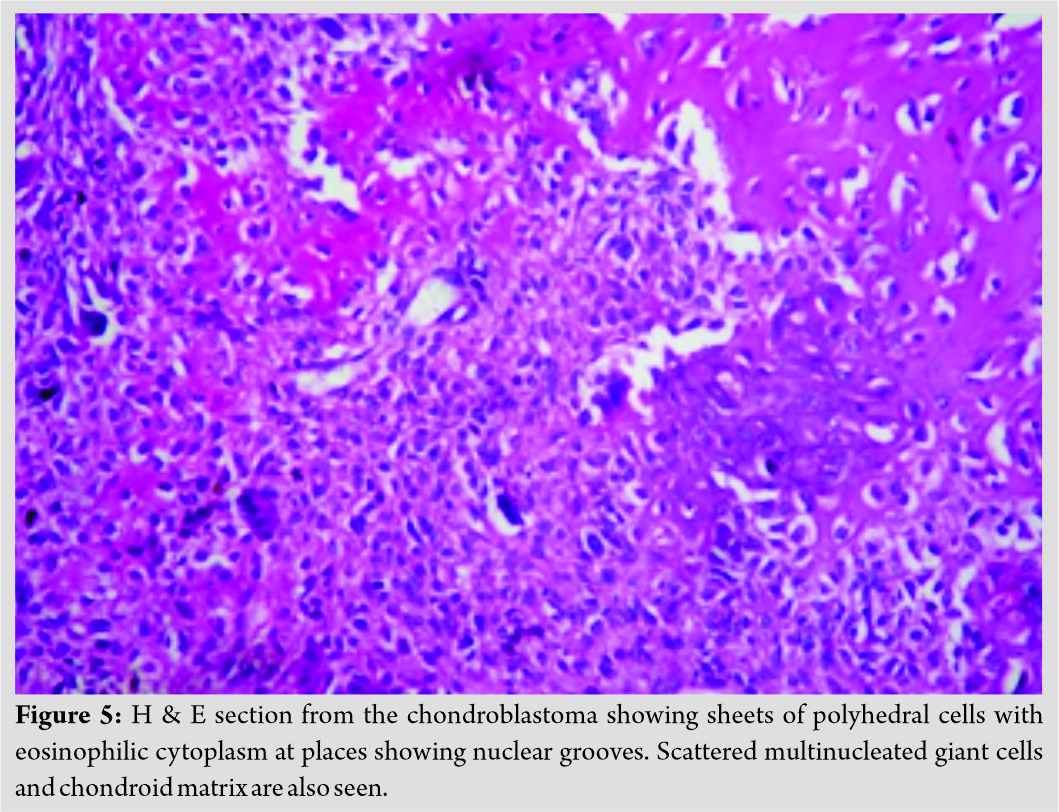 The patient was evaluated using the Modified Mayo Wrist Score (MMWS) [8] which consists a total of 100 points divided among the evaluator’s assessment of pain (25 points), active flexion/extension arc as a percentage of the opposite side (25 points), grip strength as a percentage of the opposite side (25 points), and the ability to return to regular employment or activities (25 points). An excellent result is defined as 90–100 points, good is 80–89, fair is 65–79 points, and poor is less than 65 points. Preoperatively, the patient had a MMWS of 75, which was fair, but postoperatively, patient had an excellent result with 100 points. No radiological sign of recurrence was found at 2 years follow-up and thereafter.
The patient was evaluated using the Modified Mayo Wrist Score (MMWS) [8] which consists a total of 100 points divided among the evaluator’s assessment of pain (25 points), active flexion/extension arc as a percentage of the opposite side (25 points), grip strength as a percentage of the opposite side (25 points), and the ability to return to regular employment or activities (25 points). An excellent result is defined as 90–100 points, good is 80–89, fair is 65–79 points, and poor is less than 65 points. Preoperatively, the patient had a MMWS of 75, which was fair, but postoperatively, patient had an excellent result with 100 points. No radiological sign of recurrence was found at 2 years follow-up and thereafter.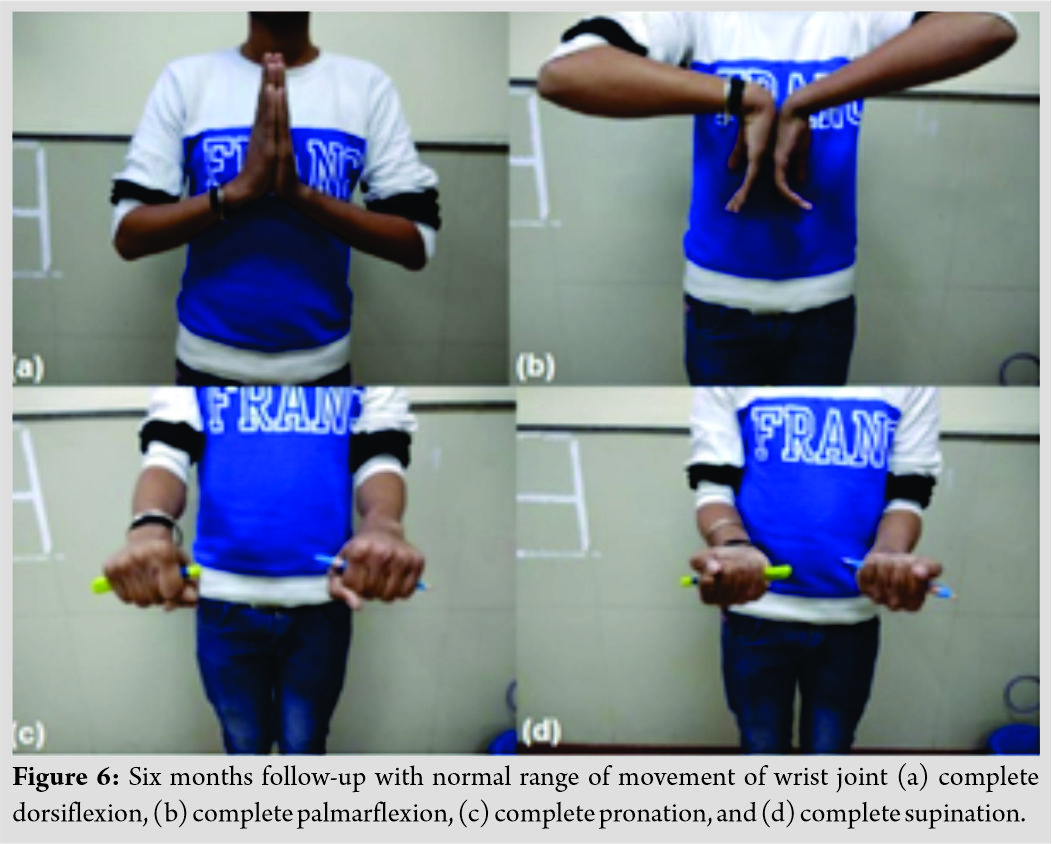
Discussion
Chondroblastomas most frequently arise in the epiphyses of long bones, with 70% occurring in the humerus (most frequent), femur, and tibia. Approximately 10% are found in the hands and feet [9]. Moreover, cases of chondroblastoma in the carpals, which have been reported [10], are scaphoid, n = 6; capitate, n = 4; lunate, n = 2; triquetrum, n = 3; trapezium, n = 2; and hamate, n = 1. To the best of knowledge, till date, there is no case reported in the literature about chondroblastoma of the pisiform. Most often, chondroblastoma is confused with giant cell tumor of bone in terms of clinical, histopathological, and radiological presentation. In general, giant cell tumors of bone tend to occur in a slightly older age range (third to the fourth decade of life, after the closure of epiphyses), which are usually larger in size and have less well-defined borders without peripheral sclerosis. Histopathologically, giant cell tumor of bone demonstrates more numerous and evenly distributed giant cells, whereas the presence of chondroblasts, chondroid matrix, chicken wire calcification, and S100 protein or DOG1 positivity suggests a chondroblastoma. Another tumor entity which can be a close mimic is chondromyxoid fibroma (CMF) which can also present as a bland cartilaginous proliferation arising in the bone of a younger individual (second to the third decade of life). CMF, however, typically arises in a metaphyseal location rather than in the epiphysis. In addition, hypercellular areas containing spindled or stellate cells in a myxoid background are characteristically seen at the periphery of a CMF, a finding that is absent in a chondroblastoma. Clear cell chondrosarcoma is an uncommon variant of chondrosarcoma that classically presents as a lytic lesion in the epiphysis of the proximal humerus or femur [11]. Although the mean age of presentation is slightly older than in chondroblastoma (third-fifth decades), the age range overlaps, and the radiologic appearance may not allow reliable distinction between the two entities. Clear cell chondrosarcoma demonstrates larger, more atypical cells with clear cytoplasm, whereas chondroblastoma is a tumor comprised of smaller round to polygonal cells with eosinophilic cytoplasm and limited cytological atypia, and thus, a good and experienced histopathologist are required to differentiate both the tumors. A chondroblastoma-like variant of osteosarcoma (CBTOS) has been reported occasionally in the literature and may difficult to distinguish from chondroblastoma [12], as both tumors can present in young patients as a lytic lesion in an epiphyseal location. CBTOS usually demonstrates small round-oval cells with eosinophilic cytoplasm and scattered giant cells and, therefore, may cause confusion with CBT, especially on a small biopsy specimen. Although generally benign, chondroblastoma is placed in the “intermediate, rarely metastasizing” category in the 2013 World Health Organization classification of bone tumors [13]. The tumor is also known to have a relatively high local recurrence rate in the order of 14% to 18% [4]. The local recurrence rate is somewhat dependent on-site; tumors in the skull and other bones with limited resectability are understandably more difficult to excise completely. Bone grafting and cryotherapy after surgical curettage decrease the risk of recurrence. Metastasis to the lung, bone, and soft tissue can occur in chondroblastoma [14], although such cases are rare (2%), and tend to show indolent growth with no significant effect on mortality. It is a very rare case and only case reported in the available literature. Among tumors involving pisiform, chondroblastoma should also be kept as a differential diagnosis. Hence, timely diagnosis and treatment may lower the risk of recurrence and improve the prognosis by retaining wrist and hand functions.
Conclusion
Chondroblastoma is most commonly found in the epiphysis of long tubular bones, especially proximal tibia or femur, distal femur, and proximal humerus, but the rare presentation is a possibility; therefore, surgeon should always keep in mind the possibility of the tumor and accurately diagnose the tumor with the help of imaging modalities and biopsy. The treatment remains the same that is bony excision and curettage.
Clinical Message
Carpal bones, including pisiform, are rare site for a tumor presentation such as chondroblastoma, for which a high index of suspicion is required and further radiological and histopathological confirmation is performed. Tumor excision/curettage is performed to treat such tumors.
References
1. Ewing J. A Treatise on Tumors. 3rd ed. Philadelphia, PA: WB Saunders; 1928. p. 293.
2. Edel G, Ueda Y, Nakanishi J, Brinker KH, Roessner A, Blasius S, et al. Chondroblastoma of bone. A clinical, radiological, light and immunohistochemical study. Virchows Arch A Pathol Anat Histopathol 1992;421:355-66.
3. Kurt AM, Unni KK, Sim FH, McLeod RA. Chondroblastoma of bone. Hum Pathol 1989;20:965-76.
4. Turcotte RE, Kurt AM, Sim FH, Unni KK, McLeod RA. Chondroblastoma. Hum Pathol 1993;24:944-9.
5. Xu H, Nugent D, Monforte HL, Binitie OT, Ding Y, Letson GD, et al. Chondroblastoma of bone in the extremities: A multicenter retrospective study. J Bone Joint Surg Am 2015;97:925-31.
6. Murray PM, Berger RA, Inwards CY. Primary neoplasms of the carpal bones. J Hand Surg Am 1999;24:1008-13.
7. De Silva MV, Reid R. Chondroblastoma: Varied histologic appearance, potential diagnostic pitfalls, and clinicopathologic features associated with local recurrence. Ann Diagn Pathol 2003;7:205-13.
8. Cooney WP, Bussey R, Dobyns JH, Linscheid RL. Difficult wrist fractures. Perilunate fracture-dislocations of the wrist. Clin Orthop Relat Res 1987;214:136-47.
9. Erickson JK, Rosenthal DI, Zaleske DJ, Gebhardt MC, Cates JM. Primary treatment of chondroblastoma with percutaneous radio-frequency heat ablation: Report of three cases. Radiology 2001;221:463-8.
10. Konishi E, Okubo T, Itoi M, Katsumi Y, Murata H, Yanagisawa A. Chondroblastoma of trapezium with metacarpal involvement. Orthopedics 2008;31:395.
11. Present D, Bacchini P, Pignatti G, Picci P, Bertoni F, Campanacci M. Clear cell chondrosarcoma of bone. A report of 8 cases. Skeletal Radiol 1991;20:187-91.
12. Aycan OE, Vanel D, Righi A, Arikan Y, Manfrini M. Chondroblastoma-like osteosarcoma: A case report and review. Skeletal Radiol 2015;44:869-73.
13. Fletcher CD, Bridge JA, Hogendoorn PC, Mertens F. WHO Classification of Tumours of Soft Tissue and Bone. 4th ed., Vol. 5. Lyon, France: IARC Press; 2013. p. 240.
14. Chen W, DiFrancesco LM. Chondroblastoma: An update. Arch Pathol Lab Med 2017;141:867-71.
 |
 |
 |
 |
 |
 |
| Dr. Ashish Rustagi | Dr. Saumya Agarwal | Dr. Geetika Khanna | Dr. L G Krishna | Dr. Jatin Talwar | Dr. Shivank Prakash |
| How to Cite This Article: Rustagi A, Agarwal S, Khanna G, Krishna LG, Talwar J, Prakash S. A Rare Case Report of Chondroblastoma Pisiform in Adolescent. Journal of Orthopaedic Case Reports 2020 September;10(6): 9-13. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


