
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Ipsilateral proximal femoral fracture surgery in patients after femoral amputation can be performed using a conventional traction operating table.
Case Report | Volume 10 | Issue 7 | JOCR October 2020 | Page 76-79 | Jun Takeba, Hiroshi Imai, Satoshi Kikuchi, Hironori Matsumoto, Naoki Moriyama, Yuki Nakabayashi. DOI: 10.13107/jocr.2020.v10.i07.1926
Authors: Jun Takeba[1], Hiroshi Imai[2], Satoshi Kikuchi[1], Hironori Matsumoto[1], Naoki Moriyama[1], Yuki Nakabayashi[1]
[1]Department of Emergency Medicine and Critical Care, Ehime University, Shitsukawa, Toon, Ehime 791-0295. Japan.
[2]Department of Bone and Joint Surgery, Graduate School of Medicine, Ehime University, Shitsukawa, Toon, Ehime 791-0295. Japan.
Address of Correspondence:
Dr. Jun Takeba,
Department of Emergency Medicine and Critical Care, Ehime University, Shitsukawa, Toon, Ehime 791-0295. Japan.
E-mail: juntake@m.ehime-u.ac.jp
Abstract
Introduction: It is difficult to use a traction table during surgery for an ipsilateral displaced femoral trochanteric fracture following above-the-knee amputation. However, there are few reports regarding such cases. We describe the simple method we used for positioning the traction table and reducing fracture site during fixation surgery for a displaced femoral trochanteric fracture in this patient following above-the-knee amputation.
Case Report: An 80-year-old man was injured in a head-on collision with an oncoming vehicle. We diagnosed him with traumatic gastric perforation, multiple right lower leg fractures, and right lower leg severe crush wound. We performed right above-the-knee amputation and laparoscopic gastrorrhaphy for lifesaving purposes. Thereafter we performed internal fixation for the right femoral trochanteric fracture on the 5th day after the injury. In that operation, we first inserted a 2.4 mm Kirschner wire under fluoroscopic guidance 3 cm proximal to the femoral cut end and attached a horseshoe and traction rope to it. Then, we tightened the rope to the foot piece of the traction table and secured it. Although shortening of the bone fracture was reduced by traction, rotation control was impossible; therefore, the horseshoe was manually controlled through clean sheets during surgery to reduce rotational displacement. We performed internal fixation surgery using a trochanteric femoral nail in the usual manner.
Conclusion: In the osteosynthesis surgery of displaced femoral trochanteric fractures following above-the-knee amputation, the method of inserting the Kirschner wire at the distal end of the patient’s femur and pulling it through the rope enables surgeons to reduce fracture shortening. Reduction of rotational displacement was possible by controlling the horseshoe by hand. In this way, intramedullary nail fixation could be performed without trouble under fluoroscopic guidance.
Keywords: Above-the-knee amputation, displaced femoral trochanteric fracture, surgery.
Introduction
It is difficult to use a traction table during surgery for an ipsilateral displaced femoral trochanteric fracture following above-the-knee amputation. How to reduce and maintain the fracture during surgery is problematic. In a patient with a severe right leg injury due to a traffic accident, we performed life-saving above-the-knee amputation on the day of the injury followed later by internal fixation for a displaced femoral trochanteric fracture on the ipsilateral side. Here, we describe the simple method we used for positioning the traction table during fixation surgery for a displaced femoral trochanteric fracture in this patient following above-the-knee amputation.
Case Report
An 80-year-old man was injured in a head-on collision with an oncoming vehicle. He was transported to our hospital by doctor car. During the whole-body evaluation, we diagnosed him with traumatic gastric perforation, right femoral trochanteric fracture (AO 31-A3), right femoral shaft fracture (32-A3), right patellar open fracture (91.1-A1), right tibial plateau open fracture (41-C1), right tibial shaft open fracture (42-A3), right lower leg severe crush wound, right fibula fracture (42-B2), and left distal radius fracture(23-A2) (Fig. 1, 2). Hemorrhage from his right lower leg wound could not be controlled with compression, and his vital signs indicated that he was in shock. The mangled extremity severity score [1] was 8 points. Taking into consideration the abdominal trauma, his age, and the severity of the lower leg wound, we performed right above-the-knee amputation for lifesaving purposes and to decrease the treatment period. Following amputation, we performed laparoscopic gastrorrhaphy. Considering the patient’s general condition, we decided to perform the femoral trochanteric osteosynthesis operation in two stages. His whole-body management was completed in the intensive care unit. Because he experienced severe hip pain during body movements, after ensuring that his general condition was stable, we performed internal fixation for the right femoral trochanteric fracture on the 5th day after the injury.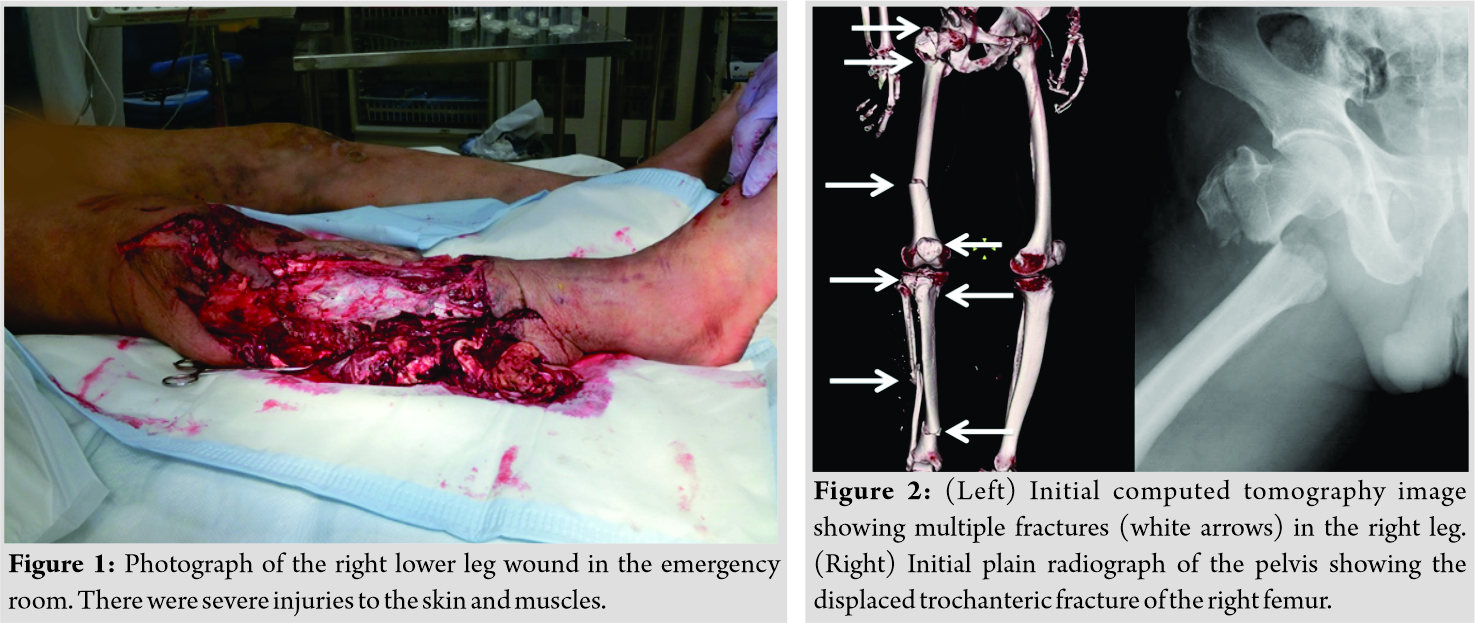
While the patient was under general anesthesia, we first inserted a 2.4 mm Kirschner wire under fluoroscopic guidance 3 cm proximal to the femoral cut end and attached a horseshoe and traction rope to it (Fig. 3). Then, we tightened the rope to the foot piece of the traction table and secured it (Fig. 4). 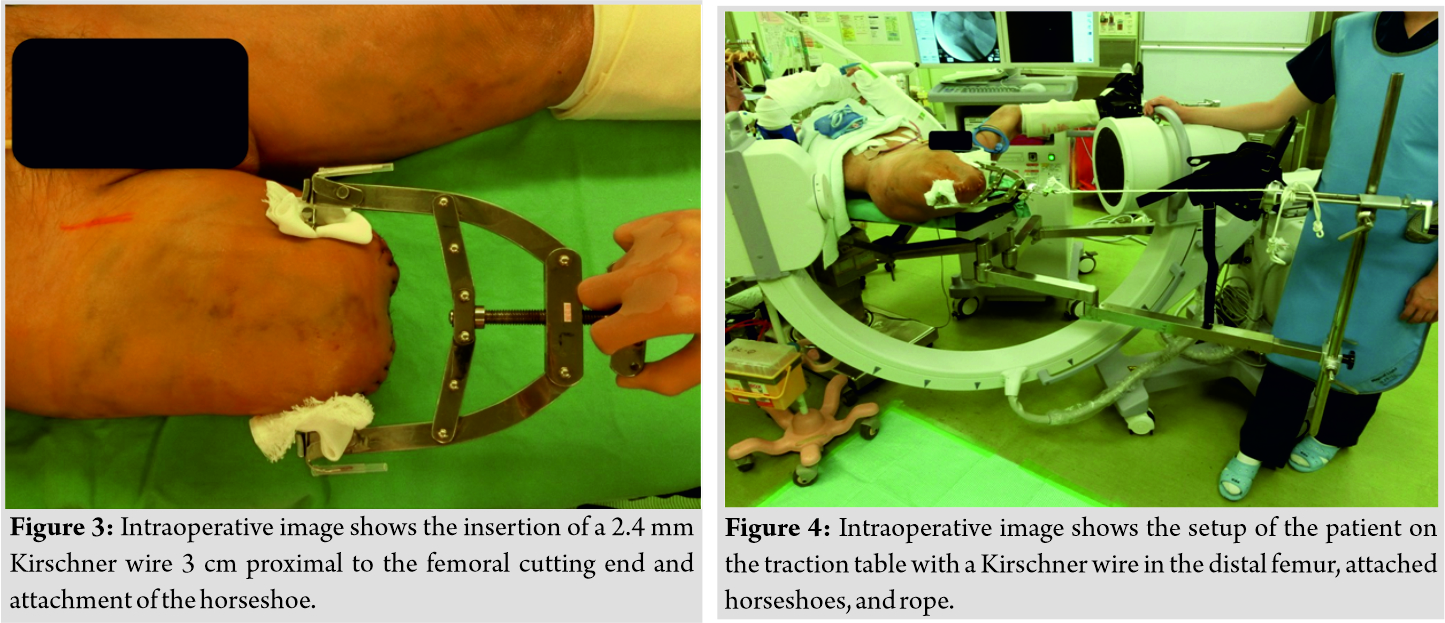 Since there is a risk of injury to the femoral arteriovenous vein when inserting the Kirschner wire, the position of the blood vessel was confirmed in advance by ultrasonography. Although shortening of the bone fracture was reduced by traction, rotation control was impossible; therefore, the horseshoe was manually controlled through clean sheets during surgery to reduce rotational displacement (Fig. 5). We performed internal fixation surgery using a trochanteric femoral nail in the usual manner (Fig. 6). The patient began transfer to a wheelchair with pain relief the day after surgery, and he started walker walking 2 days after surgery.
Since there is a risk of injury to the femoral arteriovenous vein when inserting the Kirschner wire, the position of the blood vessel was confirmed in advance by ultrasonography. Although shortening of the bone fracture was reduced by traction, rotation control was impossible; therefore, the horseshoe was manually controlled through clean sheets during surgery to reduce rotational displacement (Fig. 5). We performed internal fixation surgery using a trochanteric femoral nail in the usual manner (Fig. 6). The patient began transfer to a wheelchair with pain relief the day after surgery, and he started walker walking 2 days after surgery.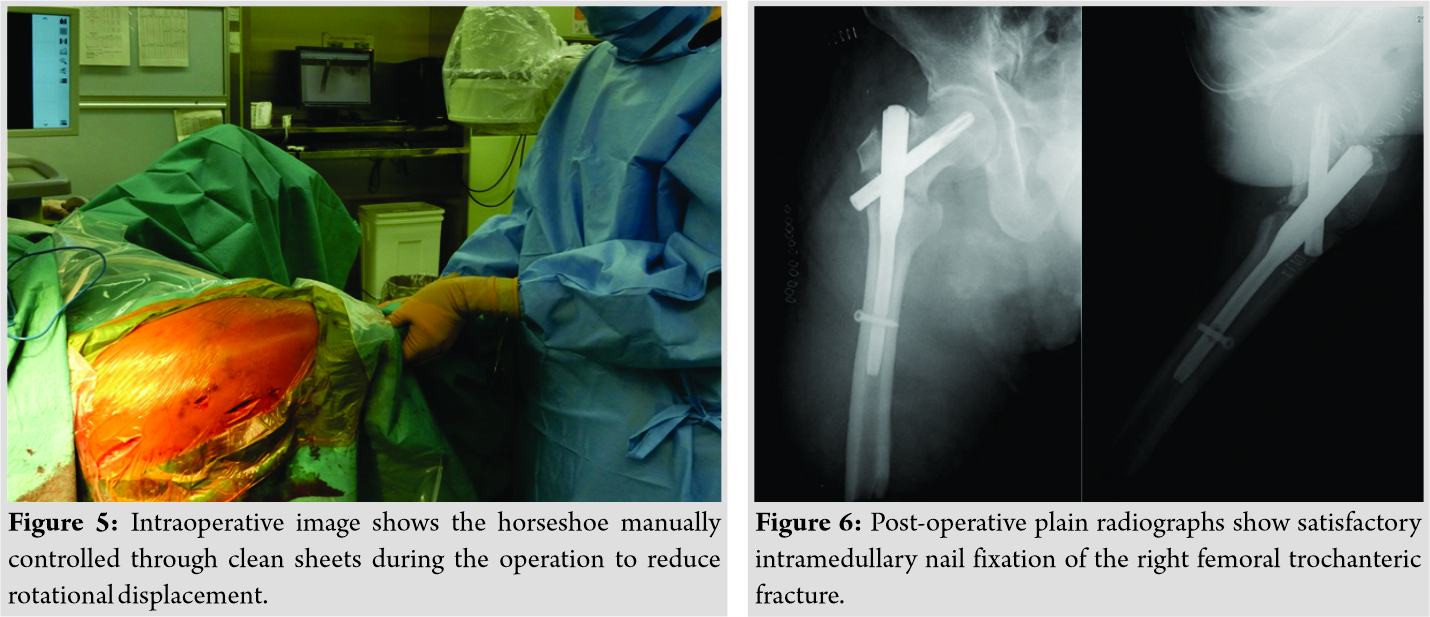
Discussion
Surgery for a femoral trochanteric fracture in a patient with an intact ipsilateral limb can be performed without trouble by positioning the patient on the traction table and reducing the fracture [2, 3]. However, in patients who have previously undergone above- or below-the-knee amputation, as in this case, positioning them on a traction table cannot be performed as usual, so special concerns are necessary. However, there are few reports regarding such cases. Al-Harthy et al. [4] reported a method of attaching the boot piece in the opposite direction at the knee flexion position. Berg and Bhatia [5] inserted a Steinmann pin in the distal femoral bone after above-the-knee amputation and then connected a traction bow and a plurality of clamps to it to enable rotational control. Although this method is useful to obtain shortening and rotation control, it is not adaptable to all patients and operating rooms. Aqil et al. [6] placed affected limbs on a radiolucent table and fixed them in situ. In terms of bone union, it is more advantageous to obtain anatomical reduction as much as possible. Davarinos et al. [7] reported that a femoral trochanteric fracture without displacement was fixed with a dynamic hip screw on the traction table using adhesive fabric tape and crepe bandage. They recommended that their technique could be useful for cases without dislocation because it is difficult to control rotation. Gamulin and Farshad [2] reported that a femoral periprosthetic fracture was fixed with locking plate on the traction table using Steinmann pin and external fixator. As our case was a femoral trochanteric fracture with shortened and rotational dislocation, we had to ensure powerful traction and rotational control during surgery. In addition, just before the patient had undergone above-the-knee amputation, we determined that intramedullary nail operation was desirable for minimally invasive purposes and that intraoperative fluoroscopy would be mandatory. Therefore, we inserted a Kirschner wire into the distal femur, attached horseshoes and rope as usual, and performed traction. Shortening was repositioned by the traction. Displacement on the medial and lateral sides could be reduced with a single blunt hook under a small incision. The reduction of rotational displacement was possible by controlling the horseshoe by hand, and the operation was performed without problems. Our method was useful in that it could be performed using only ordinary tools that are always in the hospital. One note of caution for using this method is that it is preferable to confirm the position of the blood vessel by ultrasonography because there is a risk of femoral arteriovenous injury when inserting the Kirschner wire into the distal femur [8]. The bone quality of patients who had undergone amputation surgery a long time previously is weakened [9, 10]. In such cases, care should be taken because Kirschner wires are likely to cut out during traction [2].
Conclusion
In the osteosynthesis surgery of displaced femoral trochanteric fractures following above-the-knee amputation, the method of inserting the Kirschner wire at the distal end of the patient’s femur and pulling it through the rope enables surgeons to reduce fracture shortening. Reduction of rotational displacement was possible by controlling the horseshoe by hand. In this way, intramedullary nail fixation could be performed without trouble under fluoroscopic guidance.
Clinical Message
In the osteosynthesis surgery of displaced femoral trochanteric fracture following above-the-knee amputation, the method of inserting the Kirschner wire at the distal end of the patient’s femur and pulling it through the rope and controlling the horseshoe by hand enables surgeons to reduce fracture shortening and rotational displacement. In this way, intramedullary nail fixation could be performed without trouble under fluoroscopic guidance.
References
1. Helfet DL, Howey T, Sanders R, Johansen K. Limb salvage versus amputation. Preliminary results of the mangled extremity severity score. Clin Orthop Relat Res 1990;256:80-6.
2. Gamulin A, Farshad M. Amputated lower limb fixation to the fracture table. Orthopedics 2015;38:679-82.
3. Zha GC, Chen ZL, Qi XB, Sun JY. Treatment of pertrochanteric fractures with a proximal femur locking compression plate. Injury 2011;42:1294-9.
4. Al-Harthy A, Abed R, Campbell AC. Manipulation of hip fracture in the below-knee amputee. Injury 1997;28:570.
5. Berg AJ, Bhatia C. Neck of femur fracture fixation in a bilateral amputee: An uncommon condition requiring an improvised fracture table positioning technique. BMJ Case Rep 2014;2014:bcr2013203504.
6. Aqil A, Desai A, Dramis A, Hossain S. A simple technique to position patients with bilateral above-knee amputations for operative fixation of intertrochanteric fractures of the femur: A case report. J Med Case Rep 2010;4:390.
7. Davarinos N, Ellanti P, McCoy G. A simple technique for the positioning of a patient with an above knee amputation for an ipsilateral extracapsular hip fracture fixation. Case Rep Orthop 2013;2013:875656.
8. Lowe JA, Rister J, Eastman J, Friend J. Injury to neurovascular structures with insertion of traction pins around the knee. J Orthop 2014;12:S79-82.
9. Schäfer ML, Böttcher J, Pfeil A, Hansch A, Malich A, Maurer MH, et al. Comparison between amputation-induced demineralization and age-related bone loss using digital X-ray radiogrammetry. J Clin Densitom 2012;15:135-45.
10. Rush PL, Wong JS, Kirsh J, Devlin M. Osteopenia in patients with above knee amputation. Arch Phys Med Rehabil 1994;75:112-5.
 |
 |
 |
 |
 |
 |
| Dr. Jun Takeba | Dr. Hiroshi Imai | Dr. Satoshi Kikuchi | Dr. Hironori Matsumoto | Dr. Naoki Moriyama | Dr. Yuki Nakabayashi |
| How to Cite This Article: Takeba J, Imai H, Kikuchi S, Matsumoto H, Moriyama N, Nakabayashi Y. A Simple Method for Positioning the Traction Table during Fixation Surgery for a Displaced Femoral Trochanteric Fracture in a Patient Following Ipsilateral Above-the-knee Amputation: A Case Report. Journal of Orthopaedic Case Reports 2020 October;10(7): 76-79. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


