
[box type=”bio”] What to Learn from this Article?[/box]
Signifies importance of ultra sonography in diagnosing and managing neonatal epiphyseal separation and also differentiate from dislocations.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 7-9 | Mallanagouda N Patil, Eranna Palled. DOI: 10.13107/jocr.2250-0685.332 .
Authors: Mallanagouda N Patil[1], Eranna Palled[2].
[1] Department of Orthopaedics, BIMS, Belgavi, Karnataka. India.
[2] Department of Radiology, BIMS, Belgavi, Karnataka. India.
Address of Correspondence
Dr. Mallanagouda N Patil,
Assistant professor, Dept of Orthopaedics, BIMS, Belgavi, Karnataka. India.
Email: mnpatil@gmail.com
Abstract
Introduction: Birth injuries are common phenomenon. But commonly encountered birth injuries are clavicle fracture, humerus fractures and uncommonly femur fracture. Incidence of Distal humerus Epiphyseal injuries as birth injury are rare. As the first secondary centre around elbow- capitellum appears at 3- 9 months, its radilological assessment of alignment with elbow or the radius shaft is not possible in neonates. It is difficult to differentiate elbow dislocation from epiphyseal injury in neonates.
Case Report: Here we are reporting a case of lower end humerus epiphyseal injury, as birth injury, detected in early neonatal period. This injury is unique for the reasons that detection by conventional radiography is difficult as it mimics elbow dislocation and on reduction it is unstable injury to treat by just closed reduction. The fine resolution sonography differentiates the epiphyseal separation from elbow dislocation. Till date few such cases are reported in English literature but only two in last 10 years. Though all the previously reported cases have been treated with just closed reduction, none have reported grossly unstable reduction. Here we are reporting the Lower end humerus epiphyseal injury in early neonatal period and use of thin k wire for stability for gross instability after reduction.
Conclusion: Epiphyseal injuries, though rare, are very deceptive. They have to be diagnosed properly and appropriately managed.
Keywords: neonate, epiphyseal seperation, elbow dislocation.
Introduction
Birth injuries are not uncommon incidences. Common among them are fractures of humerus, clavicle and femur. Injuries around the joint, and epiphyseal injuries are uncommon and are difficult to diagnose in view of late appearance of epiphyseal centres. For the diagnosis of these injuries, one has to have high level of suspicion, when the x ray is normal but clinical findings suggest otherwise. Distal humerus Epiphyseal injuries as birth injury are rare. As the first secondary centre around elbow- capitellum appears at 3- 9 months [1] , its radilological assessment of alignment with elbow or the radius shaft is not possible in neonates. It is difficult to differentiate elbow dislocation from epiphyseal injury in neonates.
Case Report
A three days old male baby presented to the Outpatient department with h/o excessive crying on movement of right upper limb. There was no history of fresh trauma, fever. Obstetric history was uneventful, in the form of normal vaginal delivery. Mother noticed decreased movements of right upper limb on second day of birth.
On examination, there was localized gross swelling in right elbow. There was no redness. Movements of right elbow were grossly painful with excessive crying of baby on attempt to move elbow joint. Bony land marks were not palpable in view of gross swelling. Other joints were examined and were apparently normal. Baby was afebrile on examination.
Patient was investigated with antero-posterior and lateral X-rays of right elbow (Fig 1 & 2), routine haemogram including ESR, C-reactive protein were done. Blood investigations were within normal limits. X-ray showed loss of normal anatomical alignment between humerus and radius and ulna in the elbow region on right side, similar to elbow dislocation (Fig 1 &2).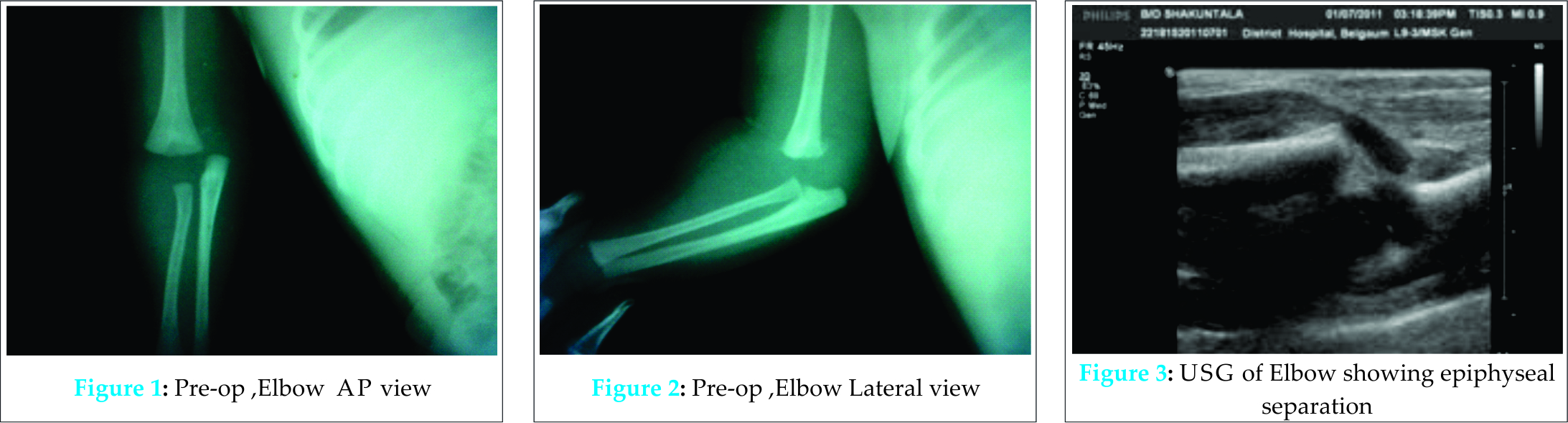
In view of rarity of elbow dislocation during this age group, patient was advised for ultra-sonography of elbow. Baby was subjected for high resolution ultrasonography (5-9MHz) examination. On ultrasound examination (Fig3), it was found that injury was distal humerus epiphyseal separation rather than the elbow dislocation, which was suspected before the scan.
Patient was posted for closed reduction under anaesthesia. On reduction, there was gross instability of physis, as evident on image intensifier as loss of humero-ulnar alignment. Hence, closed k-wiring (0.5mm diameter) was done (Fig 4 & 5). 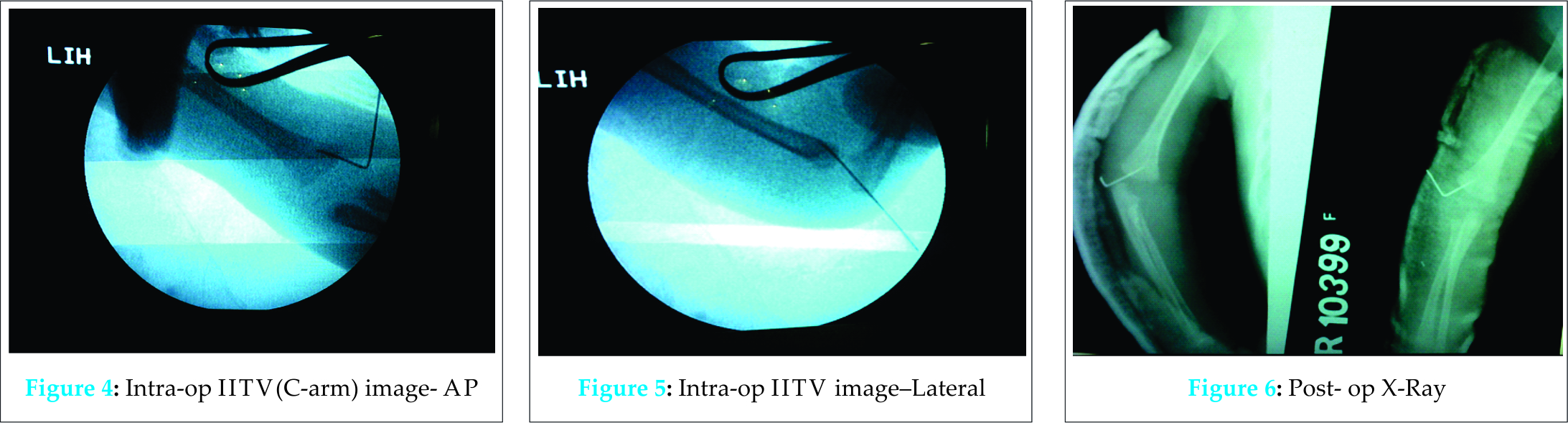 Wire was inserted with wire on T handle. Stability was achieved with wire, which was confirmed on image intensifier (Fig 4 & 5) i.e, reduction was maintained on leaving pressure. Post operatively ultrasonography was done to confirm the reduction. Post op X- rays were taken on same day (Fig 6), at 1 wk (Fig 7), 2 wks (Fig 8) and at 2 ½ months (Fig 9). This wire was kept for 2weeks. At 2 weeks there was bridging callus seen on X-ray and wire was removed. X-ray at two and half months showed complete re-modelling without deformity. Functionally, baby had full range of movements at 1 month follow up.
Wire was inserted with wire on T handle. Stability was achieved with wire, which was confirmed on image intensifier (Fig 4 & 5) i.e, reduction was maintained on leaving pressure. Post operatively ultrasonography was done to confirm the reduction. Post op X- rays were taken on same day (Fig 6), at 1 wk (Fig 7), 2 wks (Fig 8) and at 2 ½ months (Fig 9). This wire was kept for 2weeks. At 2 weeks there was bridging callus seen on X-ray and wire was removed. X-ray at two and half months showed complete re-modelling without deformity. Functionally, baby had full range of movements at 1 month follow up.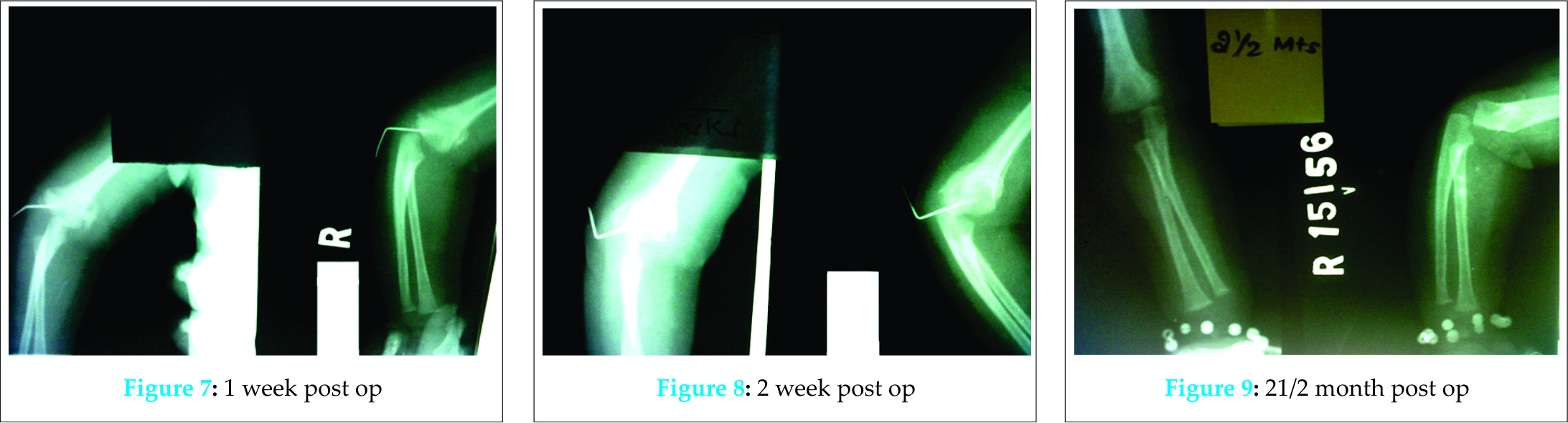
Discussion
Birth injuries are commonly seen in day to day orthopaedic practice. But distal humerus epiphyseal separation, as the birth injury is not commonly described injury. The challenge in such injury is proper diagnosis, because other common possibilities like septic arthritis of the elbow especially in premature children, where classical symptoms associated with septic arthritis are not obvious in premature children. Also, because of the swelling clinical findings of three point relationship of the elbow may not be readily appreciated in neonates. The X- ray image of such injury, may be misdiagnosed as elbow dislocation [13], as the ossification centre is not visible .Elbow dislocation is not common birth injury or injury in neonates. In this case, high resolution ultra sonography [10, 11] was very helpful tool to confirm diagnosis and plan treatment. Ultra sonography is simple investigation and this can be done in NICU facility as well. In such uncommon birth injuries, unbiased clinical examination, where ever possible, is very essential. Other differential diagnosis like ostegenesis imperfecta, child abuse should also be considered.
Treatment of such epiphyseal injuries has different approaches. Many of the case reports have suggested closed reduction and immobilization in plaster. Some case reports have indicated- no treatment for such injuries with supposed good results without any treatment. But closed reduction alone in unstable injuries has not been explained. In such cases, rather than leaving the injury unreduced (grossly mal-aligned) and hoping for the re-modelling to correct all the deformity, a thin (o.5mm) k wire for stability can be used. Since these injuries are very fast to heal in neonates, removal of wire at two weeks can be planned.
Conclusion
Epiphyseal separation of distal humerus, as birth injury is not commonly seen. Other possibilies viz septic arthritis, child abuse are part of differential diagnosis. When X ray as imaging modality is inconclusive, ultrasonography is simple and useful tool in diagnosis. In grossly unstable epiphyseal injury of distal humerus, it is better to stabilize the injury with thin K wire than hoping nature to correct the deformity completely.
Clinical Message
Utilization of ultrasonography is a useful tool in neonatal as well as, epiphyseal injuries. Its role is already proved in CDH. Proper diagnosis and simple procedure like K wiring will go a long way getting acceptable results in case of neonatal epiphyseal injuries.
References
- Rogers LF, Rockwood CA Jr. Separation of the entire distal humeral epiphysis. Radiology 1973;106:393–400.
- Camera U. Total, pure, traumatic detachment of inferior humeral epiphysis. Chir Org Movemento 1926;294–316.
- DeLee JC, Wilkins KE, Rogers LF, Rockwood CA. Fracture-separation of the distal humeral epiphysis. J Bone Joint Surg Am 1980;62:46-51.4. Downs DM, Wirth CR. Fracture of the distal humeral chondroepiphysis in the neonate. A case report. ClinOrthopRelat Res 1982;169:155–8.
- Ekengren K, Bergdahl S, Ekstrom G. Birth injuries to the epiphyseal cartilage. ActaRadiolDiagn (Stockh) 1978;19:197–204.
- Berman JM, Weiner DS. Neonatal fracture separation of distal humeral chondroepiphysis: a case report. Orthopaedics 1980;3:875–9.
- Princic J, Tonin M, Ales A. Birth trauma as the cause of fracture of the distal epiphysis of the humerus. A case report [in German]. Unfallchirurg 1995;98:487–8.
- Siffert RS. Displacement of the distal humeral epiphysis in the newborn infant. J Bone Joint Surg Am 1963;45:165–9.
- Akbarnia BA, Silberstein MJ, Rende RJ, Graviss ER, Luisiri A. Arthrography in the diagnosis of fractures of the distal end of The humerus in infants. J Bone Joint Surg Am 1986;68:599–602.
- Dias JJ, Lamont AC, Jones JM. Ultrasonic diagnosis of neonatal separation of the distal humeral epiphysis. J Bone Joint Surg Br 1988;70:825–8.
- Ziv N, Litwin A, Katz K, Merlob P, Grunebaum M. Definitive diagnosis of fracture-separation of the distal humeral epiphysis in neonates by ultrasonography. PediatrRadiol 1996;26:493–6.
- Sawant MR, Narayanan S, O’Neill K, Hudson I. Distal humeral epiphysis fracture separation in neonates—diagnosis using MRI scan. Injury 2002;33:179–81.
- Sabat D, Maini L, Gautam VK Neonatal separation of distal humeral epiphysis during Caesarean section: a case report Journal of Orthopaedic Surgery 2011;19(3):376-8
| How to Cite This Article: Patil MN, Palled E. Epihyseal Separation of Lower end Humerus in A Neonate- Diagnostic and Management Difficulty. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 7-9. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-332-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


