
[box type=”bio”] Learning Point for the Article: [/box]
Glenoid fixation by simple, more stable new technique.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 65-67| Varun Chouhan, Atul Gupta. DOI: 10.13107/jocr.2250-0685.1112
Authors: Varun Chouhan[1], Atul Gupta[1]
[1]Department of Orthopaedics, Bombay Hospital, Indore, Madhya Pradesh, India.
Address of Correspondence:
Dr. Varun Chouhan,
10 Patrakar colony, 103 Anuj apartment, Indore, Madhya Pradesh, India.
E-mail: drvarunchouhan@yahoo.co.in
Abstract
Introduction: Intra-articular glenoid fracture is rare injury and conservatively treated significantly displaced intra-articular glenoid fractures have been found to have poor functional outcomes, and thus most are now treated with open reduction and internal fixation as this allows accurate reduction of the articular surface under direct vision. [8]. Here, we describe the case of an Ideberg Type 3 fracture treated with open reduction and internal fixation by cannulated cancellous screw through coracoid process in which it is used as a reduction tool and as a guide.
Case Report: We are presenting our case where a 29-year-old man presented with the left Type 3 intra-articular glenoid fracture and proximal humerus fracture. The fracture was treated with open reduction and transcoracoid internal fixation by cancellous cannulated screw system, with a follow-up of 3 months.
Conclusion: Intra-articular glenoid fractures are uncommon and difficult to treat. Open reduction and internal fixation in the presence of associated fractures using coracoid as a guide is very simple and safe technique.
Keywords: Type 3 glenoid fracture, transcoracoid screw, open reduction internal fixation, Ideberg classification.
Introduction
Scapular fractures account for just 0.7% of all fractures [1]; of these, only 10% are intra-articular, and 1% have significant displacement [2]. However, displaced intra-articular glenoid fractures treated conservatively have been found to have poor functional outcomes [3]. Most displaced intra-articular glenoid fractures are now treated with open reduction and internal fixation [4] which allows for direct reduction of the articular surface [5]. One must also look for other injuries to the superior shoulder suspensory complex such as a clavicle or acromial fracture, or acromioclavicular injury, which will destabilize the fracture fragment [6]. Here, we describe the case of an Ideberg Type 3 fracture treated with open reduction and internal fixation by cannulated cancellous screw through coracoid process in which it is used as a reduction tool and as a guide.
Case Report
In our case, a 29-year-old male sustained a left glenoid fracture with ipsilateral proximal humerus fracture alleged a history of two wheeler-four wheeler collision. X-rays of the shoulder showed a complex intra-articular scapula fracture with proximal humerus fracture with multiple rib fractures (Fig. 1). A computed tomography (CT) scan was done which identified a comminuted fracture of the glenoid with superior medial extension through the scapula spine, in fitting with an Ideberg Type 3 injury (Fig. 2). It also showed a 5 mm intra-articular step in the glenoid on the coronal views, with fracture of proximal humerus. The fracture was treated with open reduction and internal fixation with cannulated screw system; fracture is fixed through the coracoid.
Surgical technique
The surgery was performed under general anesthesia with an interscalene nerve block. The patient was placed in a supine position with folded sheet placed under ipsilateral scapula. The arm was draped free without any traction. Preliminary radiographs were taken before draping to confirm adequate visualization of the glenoid. Deltopectoral approach taken. First Proximal humerus fracture fixation done with proximal humerus locking plate system.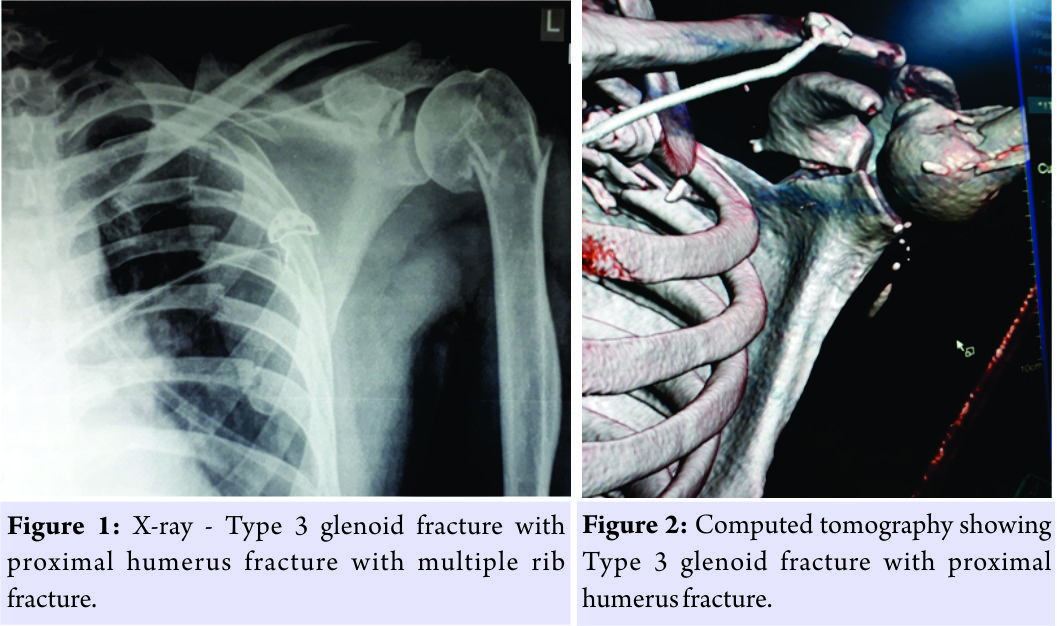 The CT scan had identified the major articular fragment to be continuous with the coracoid. The decision was made to use the coracoid as a joystick to aid indirect reduction. The subscapularis and anterior capsule were cut to open the shoulder joint. The coracoid was then held with two 3 mm K-wires (Fig. 3) and used as a joystick to manipulate and indirectly reduce the articular surface. Reduction was confirmed with direct visualization. Care was taken not to dissect 1 cm medial to the glenoid neck to avoid suprascapular nerve injury. 1.8 mm guide wires were passed through the coracoid to glenoid under direct vision. The K-wires were parallel to the coracoid and were used as a guide to show the exact trajectory for the guide wire through coracoids (Fig. 4).
The CT scan had identified the major articular fragment to be continuous with the coracoid. The decision was made to use the coracoid as a joystick to aid indirect reduction. The subscapularis and anterior capsule were cut to open the shoulder joint. The coracoid was then held with two 3 mm K-wires (Fig. 3) and used as a joystick to manipulate and indirectly reduce the articular surface. Reduction was confirmed with direct visualization. Care was taken not to dissect 1 cm medial to the glenoid neck to avoid suprascapular nerve injury. 1.8 mm guide wires were passed through the coracoid to glenoid under direct vision. The K-wires were parallel to the coracoid and were used as a guide to show the exact trajectory for the guide wire through coracoids (Fig. 4).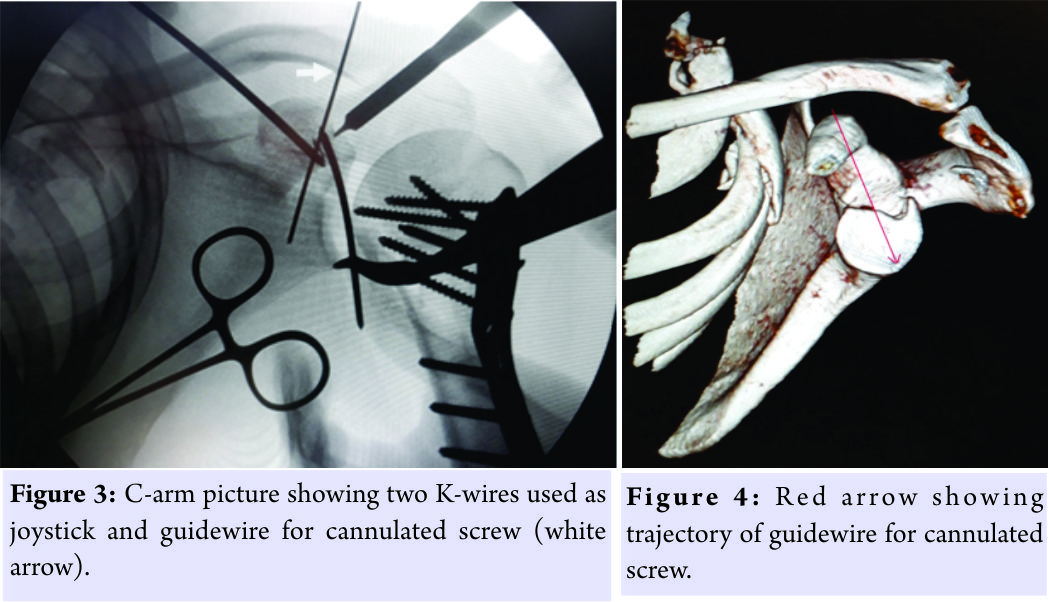 Care was taken while inserting the guide wires not to progress the wires beyond the inferior cortex of the glenoid neck to avoid injury to the axillary nerve. One self-drilling and self-tapping 4.5 mm cannulated screws were passed over the wire under fluoroscopic guidance, ensuring the screws did not breach the inferior cortex (Fig. 5). A congruent and stable articular reduction was confirmed with direct visualization and radiologically. Postoperatively, the shoulder was placed in a sling for 6 weeks with active-assisted movements commenced at 3 weeks, active abduction and internal and external rotation started at 6 weeks. Moreover, at the end of 3 months, active abduction is 100`. No implant-related issues.
Care was taken while inserting the guide wires not to progress the wires beyond the inferior cortex of the glenoid neck to avoid injury to the axillary nerve. One self-drilling and self-tapping 4.5 mm cannulated screws were passed over the wire under fluoroscopic guidance, ensuring the screws did not breach the inferior cortex (Fig. 5). A congruent and stable articular reduction was confirmed with direct visualization and radiologically. Postoperatively, the shoulder was placed in a sling for 6 weeks with active-assisted movements commenced at 3 weeks, active abduction and internal and external rotation started at 6 weeks. Moreover, at the end of 3 months, active abduction is 100`. No implant-related issues.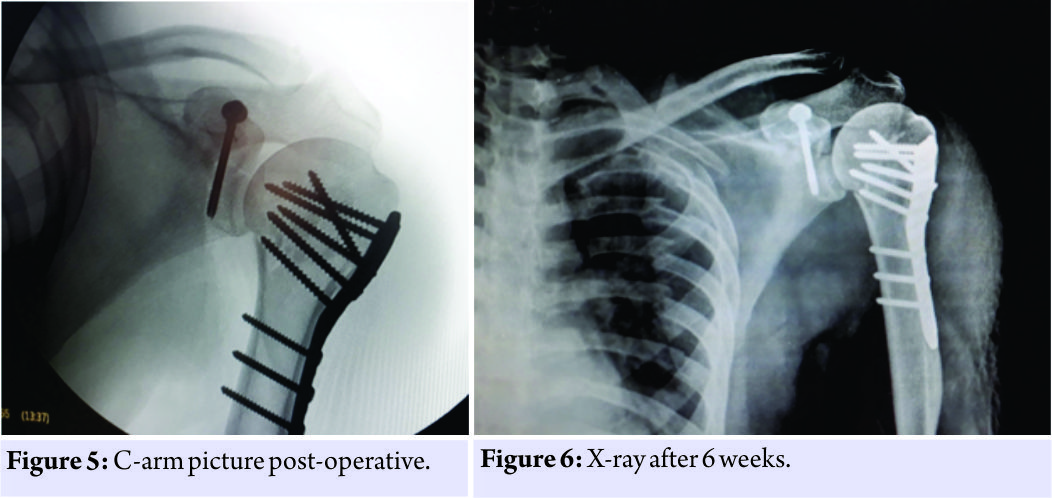
Discussion
Intra-articular displaced glenoid fractures with an articular step over 5 mm or any evidence of glenohumeral instability require anatomical articular reduction and rigid fixation to avoid early onset glenohumeral arthritis or chronic instability [3, 5]. Fracture fixation can be done through an open approach or arthroscopically assisted, with direct visualization of the articular surface and accurate reduction [3]. Arthroscopy is technically demanding and need more expertise in the presence of associated injuries such as capsular ruptures and humeral avulsion of glenohumeral ligaments. The possible complications described with arthroscopy include compartment syndrome due to fluid extravasation, anterior interoseous syndrome, and injury to neurovascular structures due to incorrect portal placement [7, 8]. In this case, reduction and fracture fixation was achieved using the coracoid process as a joystick to reduce the articular surface under direct visualization. Coracoid bony trajectory was a very convenient, simple, and more safer path for fracture fixation (Fig. 4). To the best of our knowledge, this is the first time transcoracoid definitive screw has been used to fix Type 3 glenoid fractures reported in the literature. However, Qin et al. [9] used the coracoids for temporary fixation of glenoid. The potential for neurovascular damage during guide wire or screw insertion has been highlighted in the literature. The suprascapular artery and nerve are main structure at risk [14, 15]. Hence, any blind procedure either open or arthroscopy assisted does not guarantee safety of neurovascular structures. The advantage of this new technique is that it is very simple and the guide wire and screw are within coracoid process with C-arm-assisted imaging techniques and meticulous observation, thus avoiding any potential neurovascular injury.
Conclusion
Intra-articular glenoid fractures are uncommon and difficult to treat. Open reduction and internal fixation in the presence of associated fractures using coracoid as a guide is very simple and safe technique.
Clinical Message
Coracoid process can be used as a safe guide for open reduction internal fixation of Type 3 glenoid fractures.
References
1. Cole PA, Freeman G, Dubin JR. Scapula fractures. Curr Rev Musculoskelet Med 2013;6:79-87.
2. Adam FF. Surgical treatment of displaced fractures of the glenoid cavity. Int Orthop 2002;26:150-3.
3. Gramstad GD, Marra G. Treatment of glenoid fractures. Tech Shoulder Elbow Surg 2002;3:102-10.
4. Cole PA, Gauger EM, Schroder LK. Management of scapular fractures. J Am Acad Orthop Surg 2012;20;130-41.
5. Kavanagh BF, Bradway JK, Cofield R. Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-84.
6. Goss TP. Double disruptions of the superior shoulder suspensory complex. J Orthop Trauma 1993;7:99-106.
7. Carro LP, Nunez MP, Llata JI. Arthroscopic-assisted reduction and percutaneous external fixation of a displaced intra-articular glenoid fracture. Arthroscopy 1999;15:211-4.
8. Sisco M, Dumanian GA. Anterior interosseous nerve syndrome following shoulder arthroscopy: A report of three cases. J Bone Joint Surg Am 2007;89:392-5.
9. Qin H, Hu CZ, Zhang XL, Shen LX, Xue ZC, An ZQ. Surgical treatment of ideberg Type III glenoid fractures with associated superior shoulder suspensory complex injury. Orthopedics 2013;36:e1244-50.
10. Owens BD, Goss TP. Surgical approaches for glenoid fractures. Tech Shoulder Elbow Surg 2004;5:103-15.
11. Gauger EM, Cole PA. Surgical technique: A minimally invasive approach to scapula neck and body fractures. Clin Orthop Relat Res 2011;469:3390-9.
12. Ao R, Yu B, Shi J, Li Z, Zhu Y. Acromial approach for treating glenoid fractures: A report of two cases and a literature review. Exp Ther Med 2015;10:1653-6.
13. Yang HB, Wang D, He XJ. Arthroscopic-assisted reduction and percutaneous cannulated screw fixation for Ideberg Type III glenoid fractures: A minimum 2-year follow-up of 18 cases. Am J Sports Med 2011;39:1923-8.
14. Marsland D, Ahmed HA. Arthroscopically assisted fixation of glenoid fractures: A cadaver study to show potential applications of percutaneous screw insertion and anatomic risks. J Shoulder Elbow Surg 2011;20:481-90.
15. Lantry JM, Roberts CS, Giannoudis PV. Operative treatment of scapular fractures: A systematic review. Injury 2008;39:271-83.
 |
 |
| Dr. Varun Chouhan | Dr. Atul Gupta |
| How to Cite This Article: Chouhan V, Gupta A. Transcoracoid Screw Fixation for Ideberg Type 3 Glenoid Fracture: Surgical Technique. Journal of Orthopaedic Case Reports 2018. May- June; 8(3): 65-67. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Successful Management of Atypical Bilateral Galeazzi Fractures with Unique Dorsal Displacement: A Case Report
June 1, 2025 Successful Management of Atypical Bilateral Galeazzi Fractures with Unique Dorsal Displacement: A Case Report June 1, 2025 Outcome of Clavicle Fractures Treated by Various Modalities
June 1, 2025 Outcome of Clavicle Fractures Treated by Various Modalities August 6, 2024 Functional and Radiological Outcome after Internal Fixation of Intra-articular Calcaneal Fractures
August 6, 2024 Functional and Radiological Outcome after Internal Fixation of Intra-articular Calcaneal Fractures April 10, 2024 Wide-Awake Local Anesthesia for a Proximal Humerus Fracture: A Case Report
April 10, 2024 Wide-Awake Local Anesthesia for a Proximal Humerus Fracture: A Case Report


