
[box type=”bio”] Learning Point of the Article: [/box]
Hyperflexion and rotation trauma of the knee joint result rather in bony avulsions than in ligamentous lesions in paediatric patients.
Case Report | Volume 8 | Issue 5 | JOCR September – October 2018 | Page 32-35| Jan Dauwe, Olivier Van Kerkhove, Ines Unterfrauner, Dirk Dauwe. DOI: 10.13107/jocr.2250-0685.1198
Authors: Jan Dauwe[1], Olivier Van Kerkhove[2], Ines Unterfrauner[3], Dirk Dauwe[4]
[1]Department of Trauma Surgery, University Hospitals Leuven, Leuven, Belgium.
[2]Department of Medicine, Catholic University of Leuven, Leuven, Belgium.
[3]Department of Orthopaedic Surgery, Balgrist University Hospital, Zurich, Switzerland.
[4]Department of Orthopaedic and Trauma Surgery, AZ Delta Hospital, Campus Torhout, Belgium.
Address of Correspondence:
Dr. Jan Dauwe,
Department of Trauma Surgery, Herestraat 49, 3000 Leuven, Belgium.
E-mail: dauwejan@gmail.com/jan.dauwe@uzleuven.be
Abstract
Introduction: Avulsion fractures of the tibial intercondylar eminence are rare and occur mostly in children. The purpose of this paper is to present a case of this rare pathology and to underline the importance of early diagnosis.
Case Report: A male 8-year-old child presented with pain in his left knee and difficulties to walk after a combined injury of falling and contact trauma. Radiographic studies with conventional X-ray and computed tomography (CT) scan depicted a fracture of the intercondylar eminence. In this Type II fracture according to the classification of Meyers and McKeever, an operative treatment with knee arthroscopy was established to remove the loose bone. Post-operative, the knee was immobilized in extension for 4 weeks. Physiotherapy was initiated immediately after surgery. The follow-up CT scan 6weeks after injury showed a starting consolidation and the magnetic resonance imaging scan 8 weeks after injury a complete consolidation of the fracture.
Conclusion: Hyperflexion and rotation trauma result rather in bony avulsions than in ligamentous lesions in pediatric patients. Early diagnostic examination with conventional X-ray and CTscans is performed to not miss concomitant injuries. Depending on the type of eminentiaintercondylaris fracture, an operative or conservative treatment is indicated.
Keywords: Fracture, intercondylar eminence, anterior cruciate ligament, knee trauma, pediatric injury.
Introduction
Avulsion fractures of the tibial intercondylar eminence are rarely quoted in the literature. Epidemiology shows that these fractures mostly occur in children at a frequency of circa 3 per 100.000 [1,2]. Due to the ligaments’ capacity of resistance, intercondylar eminence avulsion fractures occur mostly in children. The bony tibial eminence fails before the anterior cruciate ligament (ACL) since the intercondylar eminence is not completely ossified [3]. Tibial eminence fractures are classified into four categories according to Meyers and McKeever and modified by Zaricznyj. Type I fractures are undisplaced, Type II means partially displaced or hinged, whereas Type III fractures are completely displaced [4]. Type IV tibial eminence fractures are comminuted fractures [5]. The purpose of this case presentation is to report a case of an 8-year-old male patient who underwent an anterior tibial eminence avulsion fracture as it is a relatively rare pathology affecting mostly children and adolescents. The aim is to underline the importance of early diagnosis. Furthermore, to the best of our knowledge, an evidence-based guideline is currently not present in medical literature.
Case Report
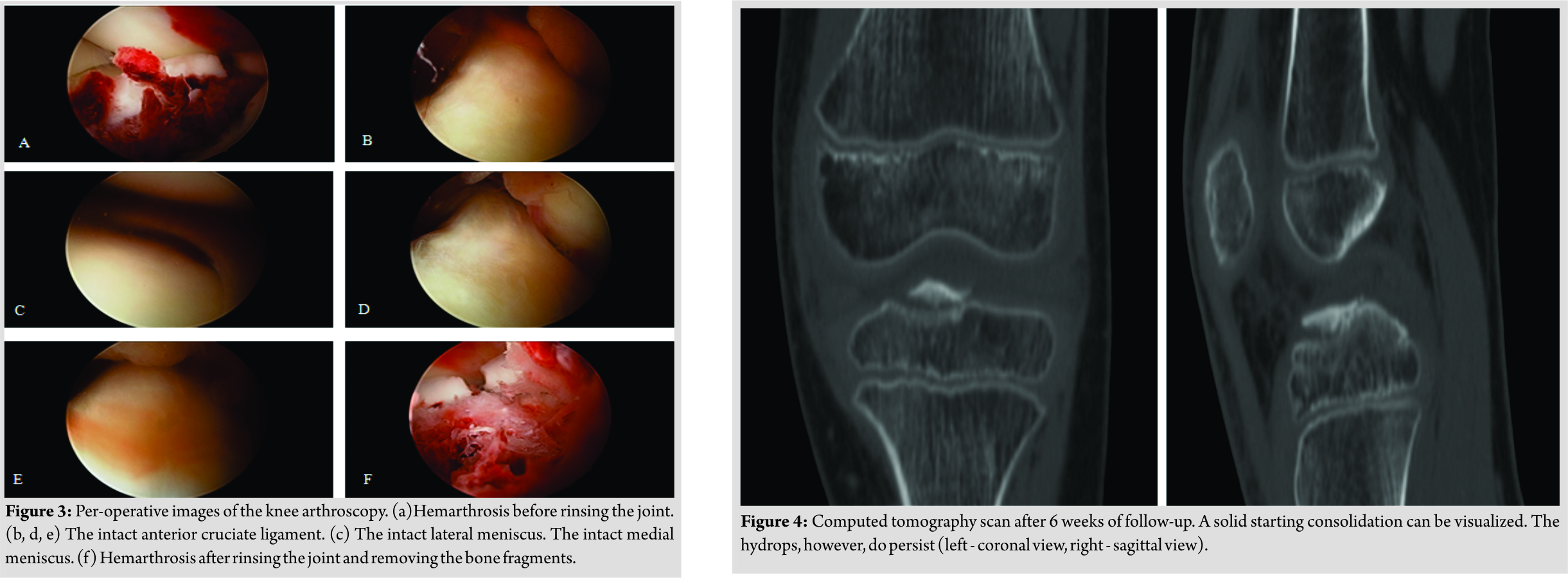
A male Caucasian 8-year-old child presented at the hospital’s emergency department in Belgium. The circumstances of the accident were reported as a fall on the left knee complicated by a contact trauma with another child. At consultation presenting, complaints were a sharp pain in his left knee and difficulties to walk. The pain was scored as 4/10 on the visual analogue scale. In clinical examination, anterior pressure pain, swelling, and a restricted range of motion(flexion up to 100° and extension deficit of 5°) were the main findings. Performing ananterior drawer test and Lachman test, no laxity was documented. On conventional anteroposterior and lateral view of the X-ray, a minimal displaced fracture of the intercondylar eminence, two loose bone fragments, and a bloated suprapatellar bursa indicating hemarthrosis could be evidenced (Fig. 1). A CT scan confirmed a fracture of the intercondylareminence (Fig. 2).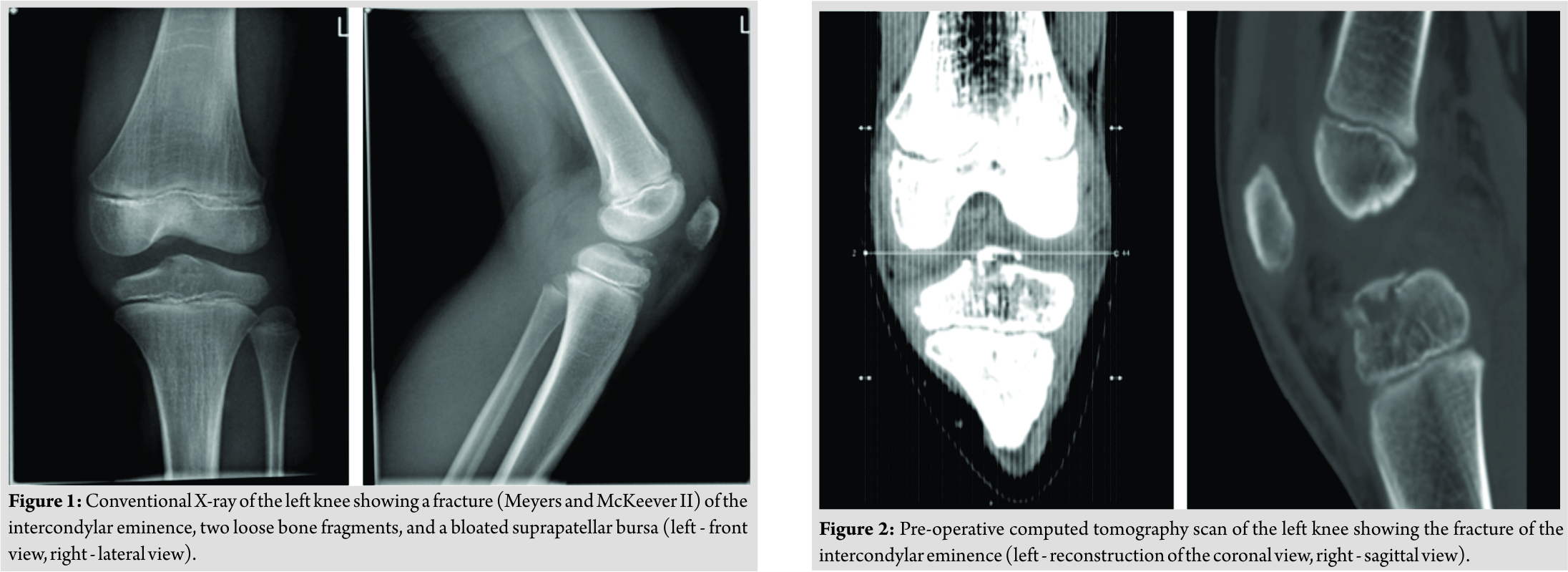 The fracture was classified as Meyers and McKeever Type II [4]. The initial treatment provided an adequate pain management with appropriate analgesics and plaster immobilization in 0–5° of flexion. Based on the clinical and radiological findings, a knee arthroscopy was performed 3daysafter injury. The indication for arthroscopic surgery was removal of the intra-articular bony fragments and to evaluate whether the fracture was stable. The fracture of the proximal tibia was visualized through arthroscopy (Fig. 3).
The fracture was classified as Meyers and McKeever Type II [4]. The initial treatment provided an adequate pain management with appropriate analgesics and plaster immobilization in 0–5° of flexion. Based on the clinical and radiological findings, a knee arthroscopy was performed 3daysafter injury. The indication for arthroscopic surgery was removal of the intra-articular bony fragments and to evaluate whether the fracture was stable. The fracture of the proximal tibia was visualized through arthroscopy (Fig. 3).
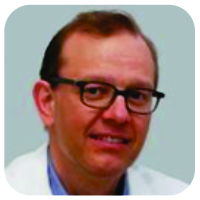
The ACL was still intact yet showed a discrete laxity. No other fractures or injuries were visualized. Furthermore, the joint was rinsed and the loose bone fragments were removed to improve thee xtension and deep flexion. Peroperatively, the ROM was tested and was complete. Postoperatively, the knee was immobilized in extension with a hard cast. Weight-bearing was not allowed. Physiotherapy was established to strengthen and stabilize the knee. In the first follow-upconsultation 1 week after surgery, a new hard cast was applied for one more week. The patient was instructed to continue the isometric exercises for adequate revalidation. After 2 weeks of cast immobilization, an extension brace was applied for another 2–3 weeks. 6 weeks after the initial trauma, clinical examination showed a positive clinical course. A follow-up CT scan was performed (Fig. 4) that could show a starting consolidation. A CT scan examination was discussed with the family of our patient since his wish was to start sporting (football) early. Furthermore, CT scan is superior to X-ray with the disadvantage of a higher radiation dose. The extension brace was removed and a soft walking brace was applied. The patient was allowed to walk by full weight-bearing, taking pain and stability into account. A T1-weighted magnetic resonance imaging (MRI) scan was performed at 8weeks of follow-up (Fig. 5).This examination was initially performed because of a new trauma and was ordered by the general practitioner. However, it is useful to present the result of the MRI in this case report. The MRI showed an almost complete consolidation alongside very limited edema of the bone (Fig. 5a and b). The ACL and posterior cruciate ligament (PCL)weretotally intact (Fig. 5c and d). Clinically, the knee showed normal stability. The walking brace was permanently removed, and the patient was allowed to perform routine daily activities including all sportive activities. No more follow-up consultations were planned.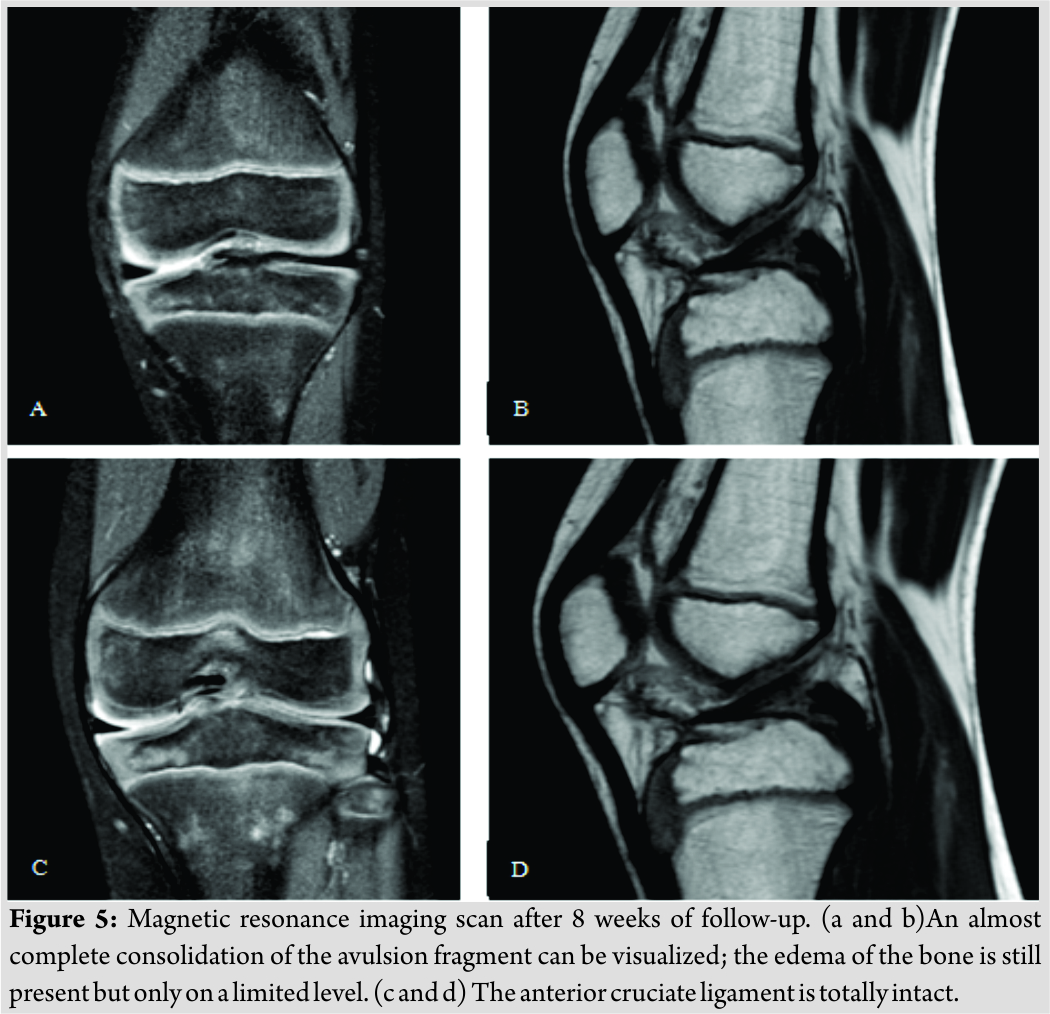
Discussion
The knee joint is a very inspiring but anatomically challenging joint as it has multiple intra-articular structures for stabilization and optimization of its movements. The cruciate ligaments are two important stabilizing factors. The ACL attaches on the medial tuberosity of the intercondylar eminence of the tibia. This eminence is the interarticular part of the two neighboring plateaus of the tibia. The PCL attaches more dorsally immediately behind the region of the eminence in the posterior intercondylar area [3]. The insertion of the medial meniscus is located ventral compared to the insertion of the ACL, whereas its lateral counterpart is sited lateral to the attachment of the ACL. Both cruciate ligaments are partially covered by the synovial membrane but are not included inside the joint capsule. Thus, the ACL has an intra-articular, yet extrasynovial position [6]. It is also important to note that the anterior portion of the ACL does not have a single anatomic insertion to both menisci. Instead, these anterior fibers merge with the anterior horns of both menisci[3]. Avulsion fractures of the intercondylar eminence are more common in children since it is not completely ossified. That is why in pediatric patients the eminence breaks before the ACL get damaged when stressed. This compromises the cruciate integrity and causes fractures in a significant portion of the weight-bearing part of the tibia [3]. In 1959, Meyers and McKeever classified tibial eminence fractures into three categories. Type I fractures are undisplaced, Type II means partially displaced or hinged, whereas Type III fractures are completely displaced [4]. This classification was modified by Zaricznyj who described Type IV tibial eminence fractures as comminuted fractures [5]. The literature quotes a clinical study about tibial intercondylar eminence fractures. 19 patients were included in the study. Kieser et al. [7]found hyperflexion and rotation the most common trauma mechanism, leading to tibial intercondylar eminence fractures. Circa half of those patients were skeletally immature. In seven of these 19 patients, direct trauma was the mechanism of injury. A review of 83 patients conducted by Aderinto et al. showed that falling, motor vehicle accidents, skiing, and soccer were the most common activities, leading to this type of injury [8]. This matched with our case where the trauma mechanism was direct, caused by a fall. In most cases, the first diagnostic examination consisted of a conventional X-ray [1, 9, 10]. Further radiographic studies, such as CT or MRI, were carried out in some cases [1, 10]. In the present case, the same technical examinations have been established. Treatment of tibial intercondylar fractures can be conservative or surgical. Conservative management comprises knee immobilization in extended position under continuous follow-up consultations, whereas operative treatment consists of arthroscopic debridement [7, 8, 9] or fracture reduction and fixation [9, 10, 11, 12, 13, 14, 15]. In the present case report, arthroscopic debridement of the bony fragments after a tibial spine fracture with intact ACL fibers documented a successful treatment.
Conclusion
Based on the present case, it may be concluded that hyperflexion and rotation trauma result in pediatric patients rather in bony than in ligamentous lesions. However, concomitant injuries should not be missed. Therefore, early diagnostic examination and appropriate therapy should be established.
Clinical Message
Hyperflexion and rotation trauma result rather in bony avulsions than in ligamentous lesions in pediatric patients. Early diagnostic examination with conventional X-ray and CT scans is performed to not miss concomitant injuries. Depending on the type of eminentiaintercondylaris fracture, an operative or conservative treatment is indicated.
References
1. Atsumi S, Arai Y, Nakagawa S, Inoue H, Ikoma K, Fujiwara H, et al. A case of nonunion avulsion fracture of the anterior tibial eminence. Case Rep Orthop2016;2016:9648473.
2. Hargrove R, Parsons S, Payne R. Anterior tibial spine fracture-an easy fracture to miss. AccidEmergNurs2004;12:173-5.
3. Wiley JJ, Baxter MP. Tibial spine fractures in children. Clin OrthopRelat Res 1990;255:54-60.
4. Meyers MH, Mckeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1959;41-A:209-20.
5. Zaricznyj B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J Bone Joint Surg Am 1977;59:1111-4.
6. Schünke M, Schulte E, Schumacher U, Voll M, Wesker K. Prometheus Anatomische Atlas. Deel 1 Algemene Anatomie en Bewegingsapparaat. 2th ed. Houten: Bohn Stafleu van Loghum; 2010.
7. Kieser DC, Gwynne-Jones D, Dreyer S. Displaced tibial intercondylar eminence fractures. J Orthop Surg (Hong Kong) 2011;19:292-6.
8. Aderinto J, Walmsley P, Keating JF. Fractures of the tibial spine: Epidemiology and outcome. Knee 2008;15:164-7.
9. Falstie-Jensen S, Søndergård Petersen PE. Incarceration of the meniscus in fractures of the intercondylar eminence of the tibia in children. Injury 1984;15:236-8.
10. Horibe S, Shi K, Mitsuoka T, Hamada M, Matsumoto N, Toritsuka Y. Nonunited avulsion fractures of the intercondylar eminence of the tibia. Arthroscopy 2000;16:757-62.
11. Shelbourne KD, Urch SE, Freeman H. Outcomes after arthroscopic excision of the bony prominence in the treatment of tibial spine avulsion fractures. Arthroscopy 2011;27:784-91.
12. Panni AS, Milano G, Tartarone M, Fabbriciani C. Arthroscopic treatment of malunited and nonunited avulsion fractures of the anterior tibial spine. Arthroscopy 1998;14:233-40.
13. Casalonga A, Bourelle S, Chalencon F, De Oliviera L, Gautheron V, Cottalorda J. Tibial intercondylar eminence fractures in children: The long-term perspective. OrthopTraumatol Surg Res 2010;96:525-30.
14. Ahn JH, Yoo JC. Clinical outcome of arthroscopic reduction and suture for displaced acute and chronic tibial spine fractures. Knee Surg Sports TraumatolArthrosc2005;13:116-21.
15. Vargas B, Lutz N, Dutoit M, Zambelli PY. Nonunion after fracture of the anterior tibial spine: Case report and review of the literature. J PediatrOrthop B 2009;18:90-2.
 |
 |
 |
 |
| Dr. Jan Dauwe | Dr. Olivier Van Kerkhove | Dr. Olivier Van Kerkhove | Dr. Dirk Dauwe |
| How to Cite This Article: Dauwe J, Kerkhove O V, Unterfrauner I, Dauwe D. Avulsion Fracture of the Anterior Intercondylar Eminence in an Eight-year-old Child: A Case Report. Journal of Orthopaedic Case Reports 2018 Sep-Oct; 8(5): 32-35. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Popliteal Artery Injury Associated with Proximal Tibia Fracture: A Case Report
June 1, 2025 Popliteal Artery Injury Associated with Proximal Tibia Fracture: A Case Report June 1, 2025 Assessment of Population Knowledge and Awareness of Nursemaid’s Elbow in Children: A Cross-Sectional Study in Al-Baha Region, Saudi Arabia
June 1, 2025 Assessment of Population Knowledge and Awareness of Nursemaid’s Elbow in Children: A Cross-Sectional Study in Al-Baha Region, Saudi Arabia May 1, 2025 Surgical Decision-Making in Thoracolumbar Fractures: A Systematic Review of Anterior and Posterior Approach
May 1, 2025 Surgical Decision-Making in Thoracolumbar Fractures: A Systematic Review of Anterior and Posterior Approach April 1, 2025 A Rare Case of Xanthogranulomatous Osteomyelitis of Radius Presenting as Pathological Fracture – A Case Report
April 1, 2025 A Rare Case of Xanthogranulomatous Osteomyelitis of Radius Presenting as Pathological Fracture – A Case Report


