
[box type=”bio”] Learning Point of the Article: [/box]
Based on this study and previous rare reports, reverse Segond fracture may not be accompanied by PCL injuries in all cases.
Case Report | Volume 9 | Issue 3 | JOCR May-June 2019 | Page 90-92 | Hamidreza Yazdi, Alireza Yousof Gomrokchi, Sina Aminizade, Sara Sohrabi. DOI: 10.13107/jocr.2250-0685.1438
Authors: Hamidreza Yazdi[1], Alireza Yousof Gomrokchi[2], Sina Aminizade[2], Sara Sohrabi[3]
[1]Department of knee Surgery, Bone and Joint Reconstruction Research Center, Neuromusculoskeletal Research Center, Iran University of Medical Sciences, Tehran, Iran
[2]Department of Bone and Joint Reconstruction Research Center, Shafa Orthopedic Hospital, Iran University of Medical Science, Tehran, Iran
[3]Department of Clinical Research Development Center, Firoozgar Hospital, Iran University of Medical Science, Tehran, Iran
Address of Correspondence:
Dr. Alireza Yousof Gomrokchi,
Department of Bone and Joint Reconstruction Research Center, Shafa Orthopedic Hospital, Iran University of Medical Science, Tehran, Iran.
E-mail: arugomrokchi@gmail.com
Abstract
Introduction: Reverse Segond fracture is a cortical avulsion fracture off the medial tibial plateau of the knee, associated with tears of the posterior cruciate ligament (PCL), medial collateral ligament (MCL), medial meniscus, and probably the anterior cruciate ligament (ACL). Unlike Segond fracture, it is a very rare injury of the knee.
Case Report: Case one is a 24-year-old male with left tibial plateau and reverse Segond fracture with an magnetic resonance imaging (MRI) showing MCL avulsion, medial meniscus entrapped in fracture site and ACL tear but intact PCL. The second case is a 56-year-old female showing reverse Segond and lateral tibial plateau fracture confirmed by X-ray and computed tomography scan. MRI revealed intact PCL, detached medial meniscus from peripheral capsule and ACL injury.
Conclusion: Based on this study and previous rare reports, reverse Segond fracture may not be accompanied by PCL injuries in all cases.
Keywords: Reverse Segond fracture, posterior cruciate ligament injury, cortical avulsion fracture, medial tibial plateau.
Introduction
Hall and Hochman were first who described a reverse Segond type fracture as a small cortical avulsion fracture from the medial aspect of the proximal tibia just below the level of the tibial plateau [1], best demonstrated on anteroposterior view of the knee [2]. He described it as posterior cruciate ligament (PCL), medial collateral ligament (MCL), and medial meniscus tear. That may also be associated with anterior cruciate ligament (ACL) injury [1]. Segond fracture is more common than reverse Segond fracture [3, 4] and includes a triad of avulsion fracture of the lateral tibial plateau with ACL tear and lateral meniscus tear [5]. The mechanism of reverse Segond fracture is valgus and external rotation forces to the knee in flexion position that is completely different to Segond fracture [2]. In this study, we described two tibia plateau fractures with reverse Segond fracture with no PCL injuries which is only reported twice in separate studies in current English literature. We also reviewed all previously published cases of reverse Segond fracture and discussed its demographic and clinical characteristics, imaging findings, and treatment options.
Case Report
Case 1
A 24-year-old male was brought to the emergency room after suffering a motorcycle versus car accident. On the initial examination and radiographic evaluation, he had left tibial plateau and reverse Segond fracture (Fig. 1). He had normal vascular and neurologic examination at initial and following evaluations. Computed tomography (CT) scan showed a large fragment avulsed from peripheral rim of medial tibial plateau in addition to lateral tibial plateau fractures (Fig. 2). Magnetic resonance imaging (MRI) showed MCL avulsion, medial meniscus entrapment and ACL tear but intact PCL (Fig. 3). The patient was approached with two separate incisions, and both fractures were fixed (Fig. 4)The medial meniscus was pulled out from fracture site and repaired. No treatment was done for ACL in acute phase. He had full knee range of motion and complete union of fractures after 12 weeks.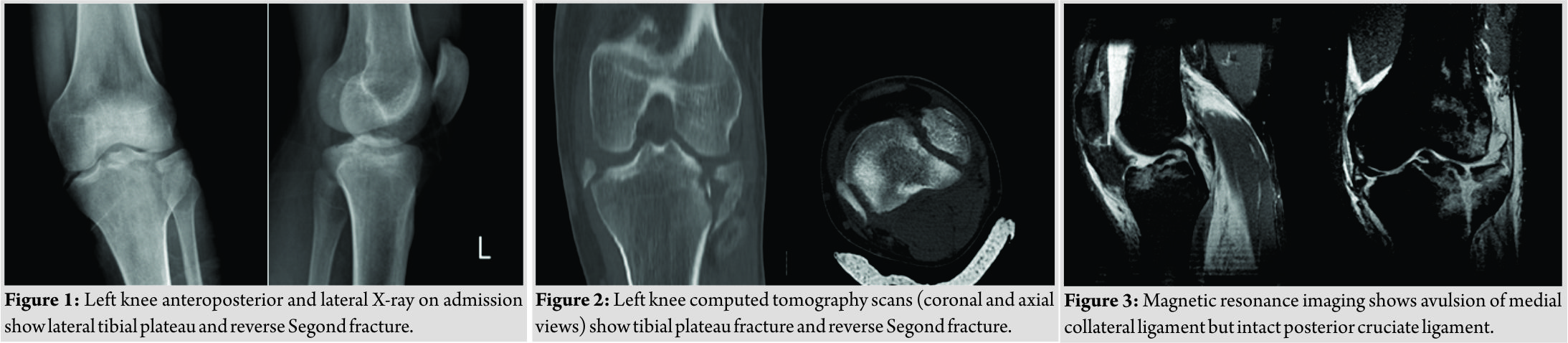
Case 2
A 56-year-old female was brought to the emergency room after suffering a motorcycle versus pedestrian accident. She had severe left knee pain and swelling. Vascular and neurologic examination was normal at initial and following evaluations. In that case, X-ray and CT scan showed reverse Segond fracture with lateral tibial plateau fracture (Fig. 5). MRI revealed MCL and ACL injuries but intact PCL (Fig. 6). The lateral plateau fracture was fixed, but reverse Segond fracture was kept intact because of small fragment. The MCL and ACL injuries were treated conservatively. The results were excellent after 12 weeks.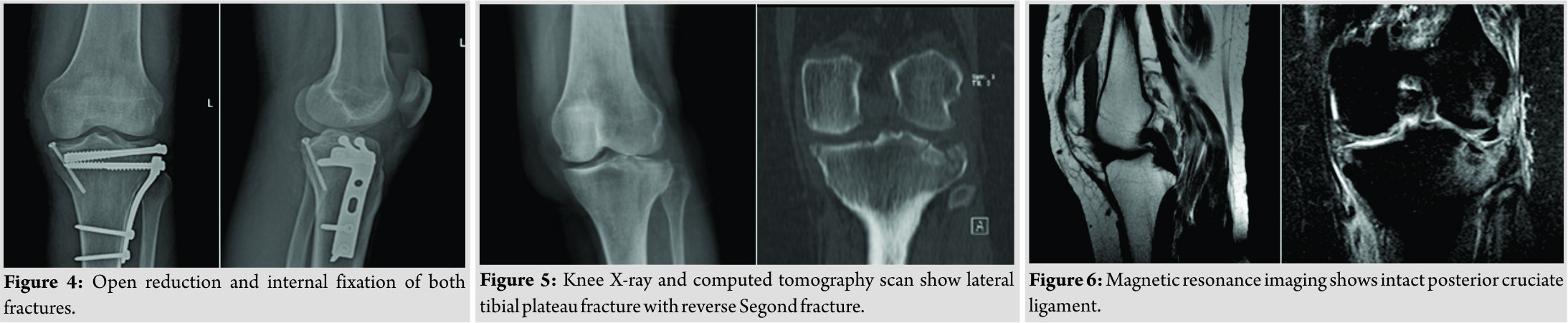
Discussion
Reverse Segond fracture is a cortical avulsion fracture off the medial tibial plateau of the knee, and it is associated with complex injuries of the knee including the (1)tears of the PCL, (2)MCL, (3)the medial meniscus, and occasionally also (4)ACL.The reverse Segond fracture has been shown to have an association with specific injury complex of the knee joint, just like the Segond fracture [1]. Reverse Segond fracture almost always results from high-energy trauma to the knee and usually affects young adults [6]. The mechanism of the previously reported cases has been postulated to be an injury causing valgus stress with the knee in flexion and external rotation [4]. Hall and Hochman considered the reverse Segond fracture as a radiographic clue for a significant internal derangement of the knee, and they showed that reverse Segond fracture is associated with PCL rupture and medial meniscal tear [1]. However, a wide variety of associated injuries has been reported so far [1, 7, 8, 9, 10, 11, 12, 13, 14, 2]. Unlike its original description, PCL rupture is not always an essential component of this injury complex. Varney [11] and Kwon et al. [14] showed intact PCL in their cases based on MRI findings which confirmed at surgery. Our study also showed the same results. One possible reason in our cases may be lateral tibial plateau fracture that compensates the force and preserves the PCL, but it needs to be evaluated more. Based on literature, medial meniscal tear is not an essential component of this complex [6, 9, 10, 11, 13, 2]. Many studies also showed intact ACL in cases with reverse Segond injuries [1, 7, 8, 9, 10, 11, 12 ,13 ,14, 2]. A general principle in treating reverse Segond fracture is the possibility of knee dislocation [6]. The surgeon should be aware of this possibility to prevent related complications. In previous studies, the appropriate treatment for reverse Segond fragment was to ignore small fragments on medial side [6]. However, if the fragment is large and compromising anteromedial knee stability and meniscal function, fixation of the fragment is advocated [6]. We fixed the large bony fragment in one case and ignore small one in another patient. High-grade injury of the MCL and the complete separation of the medial meniscus from the capsule represented by the reverse Segond fracture suggest that surgical intervention would be necessary to restore the anatomy of these medial structures [8]. In both of our cases, the detached medial meniscus was repaired. Although limited reports on the treatment of combined PCL and MCL injuries are in the literature, many clinicians would like not to manage them by operative procedures. The high-grade damage of the MCL and medial meniscus and combined PCL injury accompanied in reverse Segond fracture suggest surgical intervention to restore the anatomy of these structures [8]. In our patients, the PCL was intact, so there was no need special treatment.
Conclusion
Based on this study and previous rare reports, reverse Segond fracture may not be accompanied by PCL injuries in all cases.
Clinical Message
It could be mentioned that general principle in treating reverse Segond fracture is the possibility of knee dislocation. The surgeon should be aware of this possibility to prevent related complications.
References
1. Hall FM, Hochman MG. Medial Segond-type fracture: Cortical avulsion off the medial tibial plateau associated with tears of the posterior cruciate ligament and medial meniscus. Skeletal Radiol 1997;26:553-5.
2. Faroug R, Hasan A. Reverse Segond fracture: A case report. Inj Extra 2009;6:109-11.
3. Bilge O, Yel M, Karalezli N, Doral MN. Reverse segond fracture variant without posterior cruciate ligament injury: Report of an extremely rare case. Orthop J Sports Med 2014;2Suppl 3:2325967114S00230.
4. Bedeir YH. Reverse Segond fracture associated with anteromedial tibial rim and tibial attachment of anterior cruciate ligament avulsion fractures. Case Rep Orthop 2017;2017:4.
5. Virk JS. A unique variant of reverse Segond fracture: A case report and review of literature. Int J Orthop 2016;2:95-7.
6. Kose O, Ozyurek S, Turan A, Guler F. Reverse Segond fracture and associated knee injuries: A case report and review of 13 published cases. ActaOrthopTraumatolTurc 2016;50:587-91.
7. Gottsegen CJ, Eyer BA, White EA, Learch TJ, Forrester D. Avulsion fractures of the knee: Imaging findings and clinical significance. Radiographics 2008;28:1755-70.
8. Escobedo EM, Mills WJ, Hunter JC. The “reverse Segond” fracture: Association with a tear of the posterior cruciate ligament and medial meniscus. Am J Roentgenol 2002;178:979-83.
9. Archbold HA, Sloan S, Nicholas R. A tibial plateau fracture in a knee dislocation: A subtle sign of major ligamentous disruption. Injury 2004;35:945-7.
10. Cohen AP, King D, Gibbon AJ. Impingement fracture of the anteromedial tibial margin: A radiographic sign of combined posterolateral complex and posterior cruciate ligament disruption. Skeletal Radiol 2001;30:114-6.
11. Varney JB. Reverse Segond fracture without PCL injury. Radiol Case Rep 2012;7:537.
12. Engelsohn E, Umans H, DiFelice GS. Marginal fractures of the medial tibial plateau: Possible association with medial meniscal root tear. Skeletal Radiol 2007;36:73-6.
13. Angelini FJ, Malavolta EA, D’Elia CO, Pécora JR, Hernandez A, Camanho GL. Avulsion fracture of the medial tibial plateau (reverse Segond injury). ActaOrtop Bras 2007;15:169-70.
14. Kwon OS, Park MJ, Tjoumakaris FP. Medial and lateral Segond fractures in a skeletally immature patient: A radiographic marker for the multiply injured knee. Orthopedics 2011;34:e772-5.
 |
 |
 |
| Dr. Hamidreza Yazdi | Dr. Alireza Yousof Gomrokchi | Dr. Sara Sohrabi |
| How to Cite This Article: Yazdi H, Yousof Gomrokchi A, Aminizade S, Sohrabi S. Reverse Segond Fracture without Posterior Cruciate Ligament Injury – A report of Two Cases and Review of the Literature. Journal of Orthopaedic Case Reports 2019 May-June; 9(3): 90-92. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


