
[box type=”bio”] Learning Point of the Article: [/box]
It is possible to treat adult neglected clubfoot with the Ponseti method.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 74-77 | Davi P. Haje. DOI: 10.13107/jocr.2020.v10.i04.1810
Authors: Davi P. Haje[1],[2]
[1]Department of Traumatoly and Orthopedics, Hospital de Base do Distrito Federal, Brasília, DF, Brazil,
[2]Centro Clínico Orthopectus, Brasília, DF, Brazil.
Address of Correspondence:
Dr. Davi P. Haje,
Centro Clínico Orthopectus, SMHN – Q. 2 Bl. A, Sala 804, Edifício de Clínicas, Asa Norte, Brasília, DF, Brazil.
E-mail: davihaje@yahoo.com.br
Abstract
Introduction: The Ponseti method has been universally adopted for the treatment of children’s neglected clubfoot, but not for adult patients. In low- and middle-income countries, there are adult patients with neglected CTEV that remains untreated because the patients have limited access to specialized treatment.
Case Report: The Ponseti method was applied in a 26-year-old adult female patient with neglected clubfoot with no previous treatment. The feet had functional mobility and no residual deformities at the end of follow-upperiod. An abduction foot orthosis was prescribed for 1 year after casting period. The patient returned to normal activities after an8-month follow-up period.
Conclusion: This unique therapeutic success in an adult patient with neglected idiopathic bilateral clubfoot showed that the Ponseti method was a good treatment option.
Keywords: Neglected clubfoot, Adult, Ponseti method, Treatment outcome.
Introduction
The treatment of neglected congenital talipes equinovarus (CTEV) in children and adolescents is well described in the literature [1, 2, 3, 4, 5, 6, 7], but the management in adult patients remains unclear. The treatment of CTEV with the Ponseti method for neglected cases was first reported in 2008 when good results were described in patients up to the age of 8 years [1]. Khan and Kumar reported positive outcomes with the Ponseti method in children suffering from neglected CTEV, with one of the patients being 11.1years old [2]. Haje previously reported successful treatment of a 12.9-year-oldpreadolescent patient [3], and Adegbehingbe et al. treated cases at a maximum age of 16 years [4]. The aim of this case report was to demonstrate a unique therapeutic success in an adult female patient with previously untreated, neglected idiopathic bilateral CTEV that was initiated with the Ponseti method at 26 years of age.
Case Report
Informed consent was obtained from the family of the patient. This included advice concerning the Ponseti method treatment and proposed submission of the case for publication. The treatment began in a public tertiary referral hospital. The family was socioeconomically challenged and faced difficulty gaining access to specialized treatment previously.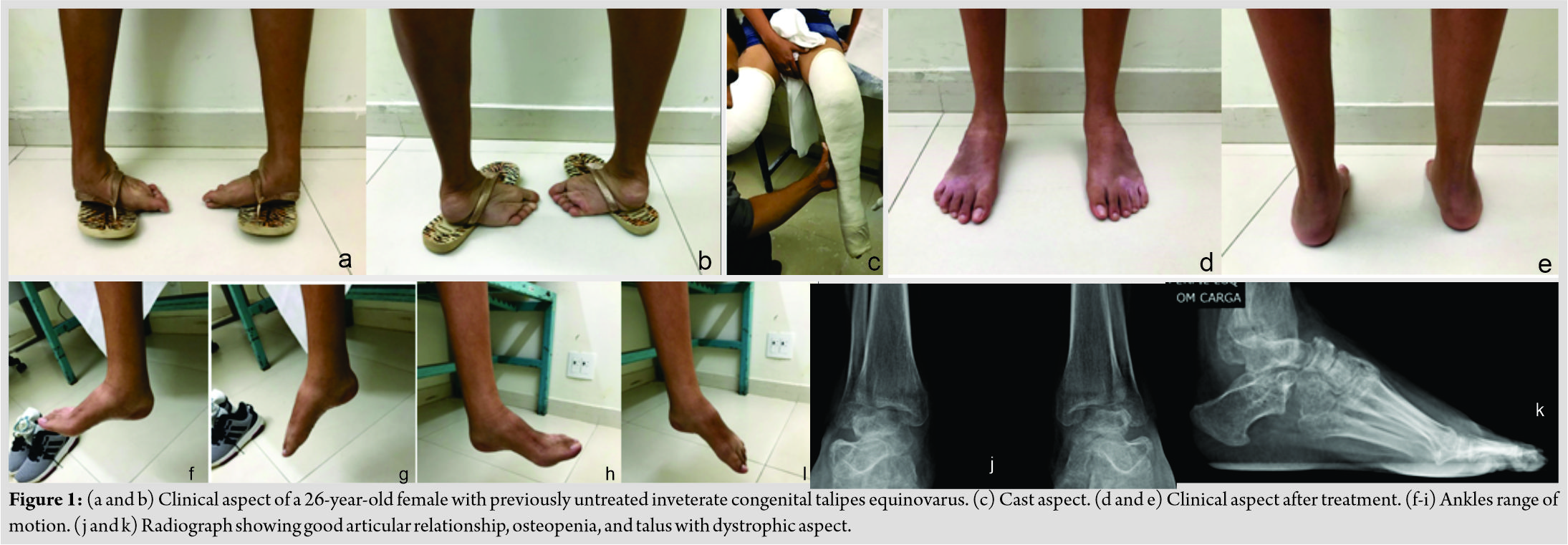
In the initial pre-treatment examination, the patient showed good gait agility, weight-bearing primarily over the dorsolateral region of the feet, with cutaneous callus aggregation over the region. The Pirani score was 6 at the first consultation. Manual manipulation and casting were performed as described by Ponseti [8, 9], with no modifications. While the above-the-knee cast was changed, the deformed foot was manipulated exactly as described by Ponseti [8, 9] by the orthopedist for around 2 min shortly before new casting was applied. Successive cast changes at 7-day intervals were carried out until all deformities were corrected, except for the equinus deformity. Seven bilateral non-weight-bearing casts applied over 45 days were needed before the tenotomy of the calcaneal tendon. There were no complications associated with cast application. The patient, when asked about the presence of pain, reported that she experienced light pain during 2 days after casting. After the fifth cast, pain progressed to moderate levels, and 30mg daily oral codeine was prescribed for management. Over correction of forefoot abduction was obtained and the residual equinus deformity remained at about 20°bilaterally. Calcaneal tenotomy was performed under local anesthesia, and only one cutaneous suture was required for sound wound closure. During tenotomy, the patient denied pain, and ankle dorsiflexion to around 0° was achieved bilaterally. The surgeon was not able to passively manipulate the feet to achieve additional dorsiflexion range of motion due to the patient reports of severe pain. Due to the substantial pain reported by the patient, 0.5 mg/kg propofol was administered through slow drip IV, which allowed for ankle dorsiflexion to around 20°. Following the procedure on the tendon, the patient was kept in an above-the-knee cast with the ankle positioned in talar neutral for an additional 21 days. After removal of the cast, an abduction foot orthosis was prescribed to minimize the chance of recurrence and was recommended for using only at night for 1 year of follow-up. A home exercise program was developed and included a mixture of active movement and passive stretching. In addition, walking with comfortable sneakers was recommended for periods without the orthosis. Visits to the outpatient clinic were scheduled with maximum intervals of 1 month over the first 8 months of follow-up; during this period, the adequacy of the abduction foot orthosis was observed, with evaluation criteria including distance between ankles, bar angled 10° apex distal with attached shoes that were positioned in 40° of outward rotation. The patient reported compliance with the use of the abduction foot orthosis at the last follow-up review, approximately 12 months post-tenotomy, when she was advised to stop using it. The cutaneous calluses over the dorsolateral regions of the feet, which had developed as a result of abnormal weight-bearing distribution, showed full spontaneous regression on correction of the deformity. The patient demonstrated plantar grade range of motion bilaterally at the final follow-up, with progressing joint mobility and muscle strength. There were no residual deformities or cutaneous calluses over the sole. The range of active and passive joint motion at the last evaluation was plantar flexion to 15°, dorsiflexion to 10°, inversion to10°, and eversion to 7°. Ranges of motion were bilateral and symmetrical. (Fig. 1) describes pre- and post-treatment clinical aspects of the feet, including radiographs after cast removal. The patient returned to her normal daily activities with 6 months follow-up.
Discussion
The limit of age for applying the Ponseti technique for patients with neglected CTEV is challenging to predict. We believe that the age of our patient, 26 years at the onset of treatment, will not be the limit for applying the Ponseti method in neglected idiopathic cases. The 2 min foot manipulation time before casting was sufficient for our case, but Lourenço and Morcuende recommended a longer time and advocated fortnightly cast changes, as these allow a longer foot remodeling period than weekly changes [1]. Our findings agree with Khan and Kumar; weekly changes, which allow for a shorter treatment time, produce satisfactory outcomes in cases of neglected CTEV [2]. Although Sinha et al. reported an increasing number of casting episodes required for maximal correction with increasing age, treating 30 patients between 1and 10 years [5], only seven casts were required before tenotomy in the present case. The risk of complications following the percutaneous sectioning of the Achillestendon in older children with neglected clubfoot has been widely reported as low [1, 2, 3, 4, 5, 6]. The upper limit of age has not been established for a complete percutaneous sectioning of the Achilles tendon in clubfoot [7, 10, 11]. Further studies will be important to assess the need for general anesthesia, due to possible pain during ankle passive dorsiflexionduring the procedure and triceps surae muscle strength following tenotomy in adult patients. Unfortunately, it remains unknown if the use of a bilateral foot abduction brace is needed to prevent relapses, especially in adult cases. We believe that it is possible to modify the Ponseti method protocol to include prescription of foot abduction orthosis, which must be individualized in adult neglected cases, with a maximum time of use of 1 year. Unlike Lourenço and Morcuende, who advocate the use of an ankle-foot orthoses instead of the foot abduction orthosis, we did not encounter any difficulties in compliance with the use of the latter until the final follow-up [1]. Although the follow-up in the present case was brief, the main purpose of this study was to report that an adult could be treated successfully by the Ponseti method. Studies with a longer follow-up and more subjects are needed to ascertain if this technique is reproducible and also better determine long-term outcomes following Ponseti method treatment in adult neglected cases. Further study should also aim to verify success rate of the tenotomy procedure, recurrence rate, best bracing protocol, the incidence of arthritis, and the necessity of future arthrodesis.
Conclusion
In low- and middle-income countries, there are adult patients with neglected CTEV that remains untreated because the patients have limited access to surgical centers or there are no skilled surgeons available to treat those deformities. The Ponseti method could be an option for the treatment of adult neglected CTEV cases.
Clinical Message
The Ponseti method could be a good treatment option for adult neglected CTEV, although the author does not know if the treatment results are going to be reproducible in all adult patients, especially in the older ones.
References
1. Lourenço AF, Morcuende JA. Correction of neglected idiopathic club foot by the Ponseti method. J Bone Joint Surg Br 2007;89:378-81.
2. Khan SA, Kumar A. Ponseti’s manipulation in neglected clubfoot in children more than 7 years of age: A prospective evaluation of 25 feet with long-term follow-up. J Pediatr Orthop B 2010;19:385-9.
3. Haje DP. Neglected idiopathic bilateral clubfoot successfully treated with the Ponseti method: A case report. JBJS Case Connect 2013;3:e9.
4. Adegbehingbe OO, Adetiloye AJ, Adewole L, Ajodo DU, Bello N, Esan O, et al. Ponseti method treatment of neglected idiopathic clubfoot: Preliminary results of a multi-center study in Nigeria. World J Orthop 2017;8:624-30.
5. Sinha A, Mehtani A, Sud A, Vijay V, Kumar N, Prakash J. Evaluation of Ponseti method in neglected clubfoot. Indian J Orthop 2016;50:529-35.
6. Spiegel DA, Shrestha OP, Sitoula P, Rajbhandary T, Bijukachhe B, Banskota AK. Ponseti method for untreated idiopathic clubfeet in Nepalese patients from 1 to 6 years of age. Clin Orthop Relat Res 2009;467:1164-70.
7. Digge V, Desai J, Das S. Expanded age indication for Ponseti method for correction of congenital idiopathic talipes equinovarus: A systematic review. J Foot Ankle Surg 2018;57:155-8.
8. Ponseti IV. Treatment of congenital club foot. J Bone Joint Surg Am 1992;74:448-54.
9. Ponseti IV, Smoley EN. The classic: Congenital club foot: The results of treatment. Clin Orthop Relat Res 2009;467:1133-45.
10. Maranho DA, Nogueira-Barbosa MH, Simao MN, Volpon JB. Ultrasonographic evaluation of Achilles tendon repair after percutaneous sectioning for the correction of congenital clubfoot residual equinus. J Pediatr Orthop 2009;29:804-10.
11. Maranho DA, Leonardo FH, Herrero CF, Engel EE, Volpon JB, Nogueira-Barbosa MH. The quality of Achilles tendon repair five to eight years after percutaneous tenotomy in the treatment of clubfoot: Clinical and ultrasonographic findings. Bone Joint J 2017;99:139-44.
 |
| Dr. Davi P. Haje |
| How to Cite This Article: Haje DP. Method: A Case Report of an Adult Patient who Started Treatment at 26 Years of Age. Journal of Orthopaedic Case Reports 2020 July;10(4): 74-77. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Cadaveric Dissection of Adult Neglected Talipes Equinovarus
July 1, 2026 Cadaveric Dissection of Adult Neglected Talipes Equinovarus June 1, 2026 Clinicoradiological Outcomes after Percutaneous Radiofrequency Ablation of Benign Bone Tumors: A Prospective Observational Study
June 1, 2026 Clinicoradiological Outcomes after Percutaneous Radiofrequency Ablation of Benign Bone Tumors: A Prospective Observational Study June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study
June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing